Keywords
Celiac plexus; Nerve Block; Pancreatic Diseases;
Pancreatitis, Calcific; Visual Analog scale
Abbreviations
CCP chronic calcific pancreatitis; DPPHR duodenumpreserving
pancreatic head resection; LPJ lateral pancreatic
jejunostomy; NCPB neurolytic celiac plexus block; QOL quality of life
INTRODUCTION
Background and Objectives
In chronic calcific pancreatitis (CCP), the most
worrisome feature is debilitating chronic abdominal pain
(90-100%) which increases analgesic requirement and
leads to poor quality of life [1]. Around 40-50% of patients
can be managed conservatively, but the remaining 50-60%
eventually requires surgical therapy [2, 3].
Lateral pancreatico jejunostomy provides symptomatic
relief in 50-70% of patients especially in those who have
a wide duct (>7 mm), suggesting that this procedure
addresses only the ductal hypertension theory [4, 5].
Randomized controlled trials comparing resectional and non resectional procedures have proved that Frey’s
procedure is superior since it was introduced in 1987 [6].
Although it addresses both ductal hypertension and the
pacemaker theory, it provides only 80 to 90% pain relief
[7, 8]. Small duct disease, alcoholic pancreatitis, longer
disease duration, multiple prior endoscopic interventions,
centralized (non-visceral) pain state and pre-operative
opioid usage are factors found to be associated with failure
of surgical therapy [9, 10]. However, the reason for the 10-
20% of failure is probably due to unaddressed or partially
addressed neurogenic mechanisms of pain.
Neuro ablation can be considered not only for
malignancy but also for CCP without pancreatic duct
dilation [11]. In identifying the neurogenic cause as the main
culprit for failure of Frey’s procedure the efficacy of intra
operative celiac plexus neurolysis was tested by conducting a
randomized trial. Until the present, there are no prospective
studies comparing this technique in combination with the
Frey’s procedure in the treatment of CCP.
METHODS
This study was started after getting approval from
institutional ethical committee of Madras Medical College,
Chennai, Tamil Nadu, India. This trial was registered at
clinical trials.gov: NCT- 02735330.
Sample Size
This study was based on a retrospective study
undertaken by Carlos Chan et al. [12]. Pain control was
the primary endpoint. Based on the literature pain control
was recorded as 85% for Frey’ procedure. To have 95%
confidence interval and 10% clinically expected variability,
136 subjects would be required, 68 in each arm of the
study.
Formula used for this trial is,
N = [Z / d]2 × P × Q
N = 67.79 (68)
N = size per group; p = the response rate of standard
treatment group. Q = Complement of P. d = the real
difference between two treatment effect.
Inclusion Criteria
Patients considered for inclusion were those CCP
patients between 13 to 65 years of age, with a pain score
greater than 7, preoperative opioid use, must have desisted
from alcohol and smoking for at least 6 months and with
good performance status (ECOG ≤1- Eastern Cooperative
Oncology Group).
Exclusion Criteria
Patients with mild to moderate pain score, continuous
substance abuse, poor performance status (ECOG>1) were
excluded from the study.
Primary Outcome
Post-operative pain relief measured by Visual Analogue
Scale (VAS) (Range, 0-10) was the primary end-point of
this study.
Secondary Outcome
Izbicki pain score [8] improvement, decrease in opioid
analgesic consumption, weight gain, improvement in
exocrine and exocrine function, as well as improvement in
QOL were the secondary indicators.
Method of Study
The study comprised a single center, randomized
(simple), double- blind, placebo- controlled, parallel arm,
superiority trial. Randomization was undertaken at the
time of surgery by an office staff using a random number
table created with computerized software by a statistician
not involved in the study. Blinding and allocation
concealment was performed by using pre numbered
containers previously filled with either absolute alcohol
or saline according to the randomization chart which was
kept sealed by office staff until the end of the study. Both
subjects and response assessor were blinded.
Morphological and ductal anatomy was defined by
contrast enhanced computed tomography (CT) / magnetic
resonance cholangio pancreatography (MRCP). Pancreatic
head mass was defined if antero-posterior diameter of
head was >35 mm on CT. Type-1 pain was defined as shorter episodes of pain separated by pain-free intervals
of several months. Type-2 pain was defined as prolonged
periods of persistent (daily) or clusters of recurrent severe
pain exacerbations. The small duct disease was defined as
those having duct diameter of less than or equal to 5mm at
the neck [12, 13].
Intra operatively anesthetists were informed
while performing the NCPB/Placebo. Peripancreatic
inflammation was diagnosed as inflammation extending
beyond pancreas involving retropritoneum and adjacent
structures noted by CT scan and confirmed during surgery.
Analgesics were given in the early post-operative
period in the form of epidural bupivacaine and tramadol
and beyond post-operative period given according to
WHO ladder (paracetamol, week opioids like tramadol and
strong opioids like morphine).
The pain score was recorded every 3 months by the
primary investigator Patients who had a VAS score of >3
and requiring increased opioid analgesics were considered
as failures of the procedure. Patients are considered as
opioid dependent when they required opioids even though
having mild pain score (<3) after surgery. The patients with
poor surgical outcome (failure) were referred to pain clinic
Izbicki et al. proposed a scoring system in CCP using
4 variables with scores ranging between 0-100 for each
variable namely frequency of pain attacks, VAS sore,
analgesic medication(morphine related analgesic potency,
time of disease related inability to work [8]. Secondary
outcome measures were noted at the end of every 6
months. The mean values at the last follow up were taken
as end-points for assessment of secondary outcomes.
Standard questionnaire format of SF 12 Version-2 with
4 weeks recall protocol was used for QOL assessment.
Data Collection
The preoperative baseline details such as etiology,
morphology, associated complications and VAS pain score,
Izbicki pain score, weight loss, endocrine status, exocrine
status (fecal elastase) were collected on admission.
Additional procedures, the presence of chronic
peripancreatic inflammatory changes [1] as evidenced by
difficult Kocharisation due to adherent capsule and intraoperative
complications were recorded during surgery.
Follow up details including pain relief measured by
VAS score and Izbicki pain score, analgesics requirement
weight gain, improvement in steatorrhoea (improvement
in fecal elastase>200 μg/g of stool when associated
with subjective reduction in foul smelling oily diarrhea),
improvement in diabetic status (insulin& oral hypoglycemic
agents requirement, HgbA1c), new onset diabetes (fasting
glucose, GTT) mortality and morbidity were noted.
Follow up data were collected every 3 months on an
outpatient basis. QOL assessment was done with a face to
face interview as outpatient basis every 6months. The last
follow up scores were used for analysis.
Statistical Analysis
Statistical analysis was performed in SPSS version 20.
Continuous variables were presented as mean, standard
deviation and 95% confidence interval; categorical
variables were presented as frequencies. The chi-square
test and the Fisher exact test were used to analyze
categorical variables. The unpaired Student t test was
used to analyze continuous variables. Missing values are
treated with last observed value carried forward method.
P value <0.05 was considered statistically significant.
Factors found significant on univariate logistic regression
analysis were incorporated in to the multivariate logistic
regression analysis for odds ratio with 95% confidence
intervals to analyze the significant factors affecting the
outcome of surgery.
Procedure
All patients underwent Frey’s procedure irrespective
of the presence or abcence of pancreatic headmass [14].
Additional procedures were performed as indicated to
address specific complications. Operative procedures
were performed by a single team with 2 experienced
surgeons having more than 20 years of experience in
this field. NCPB was performed after the head coring but
before pancreatico jejunostomy, to avoid undue tension
over anastamosis.The fascia overlying the aorta and celiac
axis was not disected to facilitate diffusion of the drug or
placebo. NCPB was performed either with 20 ml absolute
alcohol diluted to 40 ml(50%) in study group or with 20
ml of saline mixed with 20 ml of distilled water in placebo
group using a 22 gauge spinal needle injected just below
the crus of the diaphragm, 20 ml on either side of celiac
axis in a four quadrant fashion.
RESULTS
Study Population
165 consecutive CCP patients admitted in our
department since January 2013 were screened for
eligibility (Figure 1). 29 patients were excluded (25
were not meeting the inclusion criteria and 4 patients
not willing to participate). After exclusion 136 patients
were included in our study. They were randomized in to
2 groups, one group was treated by Frey’s procedure with
NCPB (Group-I) and the other by Frey’s procedure with
saline as placebo (Group-II).
Figure 1: Consort Study Design.
ITT intention to treat analysis; HPE histopathological examination
All patients in this study were taking opioid
preoperatively either continuously or intermittently
depending upon the type of pain. Pancreatic pain was the
most common indication for surgery. Type 2 pain was more
common in alcoholic CCP and in those with associated
complications (Table 1).
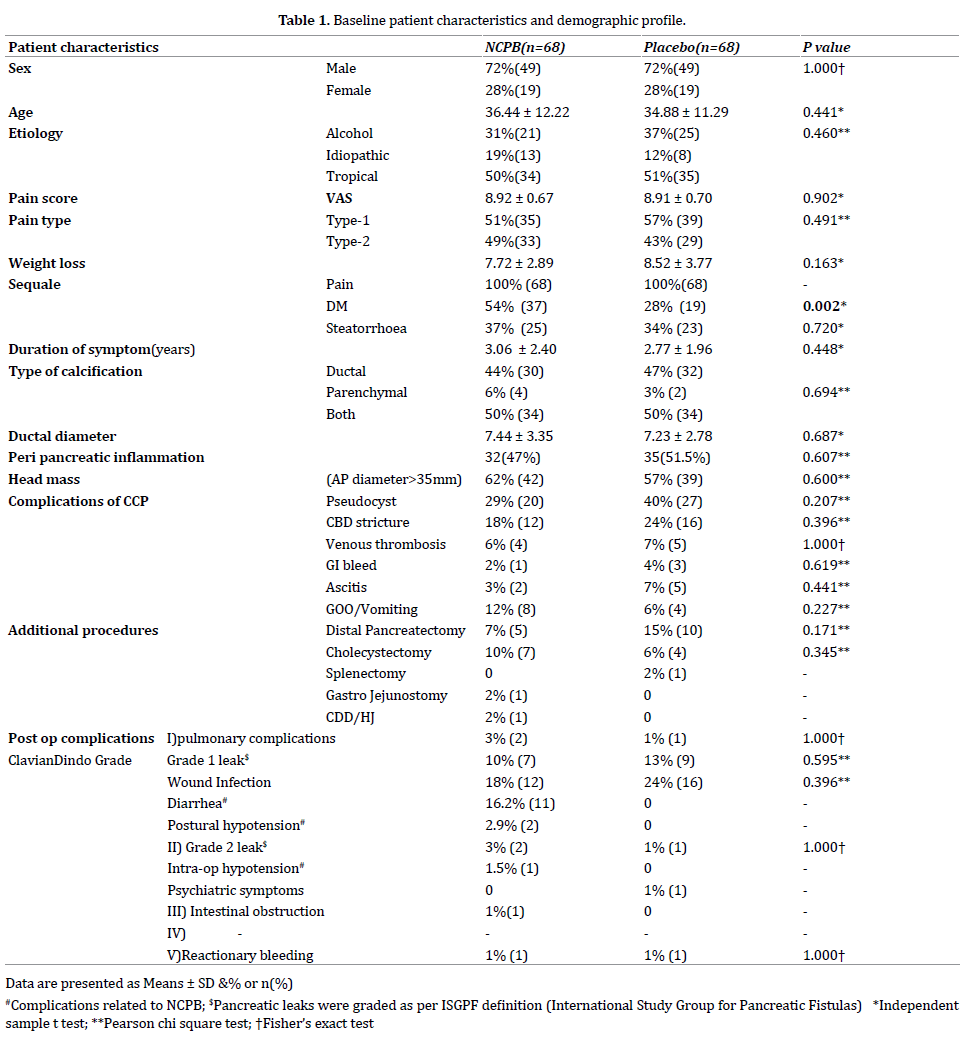
Combined ductal and parenchymal calcification pattern
(50%) was more common rather than pure ductal (45.5%)
and parenchymal (4.5%) calcification. Mean ductal diameter
was 7.3 mm. 36% of patients had small duct disease 60% of
the study populations had a pancreatic head mass. 50 % of
patients had peripancreatic inflammation.
Pseudocyst was the most common complication
followed by CBD stricture, venous thrombosis, GI bleeding,
ascitis, and gastric outlet obstruction (GOO). Most of the
CBD strictures were only radiological evidence of smooth
narrowing of distal intra pancreatic bile duct without any
biochemical changes like jaundice or elevated ALP (in which
the decompression of the head itself will produce good
relief) except in one case where persistent biochemical
changes were present which necessitated surgical bypass.
Notably the functional gastric outlet obstruction (gastro
paresis) was more (8.8%) with those having small duct
disease. Alcoholic CCP patients had more complications in
this study.
In addition to Frey’s procedure, additional
procedures were performed for complications of CCP.
After randomization the baseline variables are equally
distributed in both groups except for diabetes mellitus
which were more in NCPB group (p=0.002).
Morbidity and Mortality
One patient had intra operative hypotension. Grade
1 pancreatic leaks (n=2) were managed conservatively.
There were two grade 1 pancreatic leaks which resolved
on conservative management. One Grade 2 leak resolved
with percutaneous drainage under ultrasound guidance
and octreotide infusion. Pulmonary complications and
wound infections were more common in the placebo
group. The most common complication associated with
NCPB was diarrhea and postural hypotension usually
after the 2nd postoperative day. All were successfully
treated conservatively with crystalloids infusion
(Table 1).
There were two postoperative deaths within 30 days
(1.4%),one in each group. One patient (group I) sustained
reactionary hemorrhage following Frey’s procedure
combined with distal pancreatectomy and splenectomy.
The second patient (group II) experienced splenic
vein thrombosis without varices but did not undergo
splenectomy, however developed massive gastrointestinal
haemorrhage and shock 28 days after surgery.One patient
(group I) died in a road traffic accident 6 months after the
procedure.
PRIMARY OUTCOME ASSESSMENT
There was a significant decrease (P<0.0001) in VAS
mean pain score in group I (NCPB) up to3 years of postoperative
assessment (Figure 2). Few patients had milder
pain (VAS≤3) in the postoperative period either due to
complications or wound pain due to surgical procedures
in both groups. Even in this recurrence group, there was a
significant pain free interval of 4 months in group I. There
were twelve patients considered as treatment failures but
only one in group 1 (Figure 3a).
Figure 2: The mean values of VAS pain score up to the last follow up period are represented with linear graphical lines and the number of paints at a given point of time are given at the top of each block.
Out of twelve treatment failure patients seven
underwent successful CT guided celiac plexus neurolysis
and 4 had failed neurolysis (Figure 3b). One patient in
group 2 underwent revisional surgery and intraoperative NCPB. This patient was having centralized pain state and
was experiencing recurrence of pain every 2 months.
He underwent CT guided NCPB on three occasions and
continued to have a requirement for morphine.
Figure 3: Recurrence and Reinterventions. (a). Recurrence in both groups with etiological subtypes. Failure rates are depicted as percentage. (b). Reinterventions performed for the poor outcome patients. Failed attempts for 4 patients indicate difficulty in placing the needle due to altered anatomy in the postoperative period.
SECONDARY OUTCOME ASSESSMENT
There was a significant reduction of all variables in
Izbicki score, when compared to preoperative value in both
groups, except for analgesic intake which was significantly
altered only in the NCPB group (85% vs. 13%, P<0.0001)
(Table 2). The overall improvement in Izbicki score was
86% in the NCPB group compared to 58% in placebo group
[P<0.0001] (Figure 4).
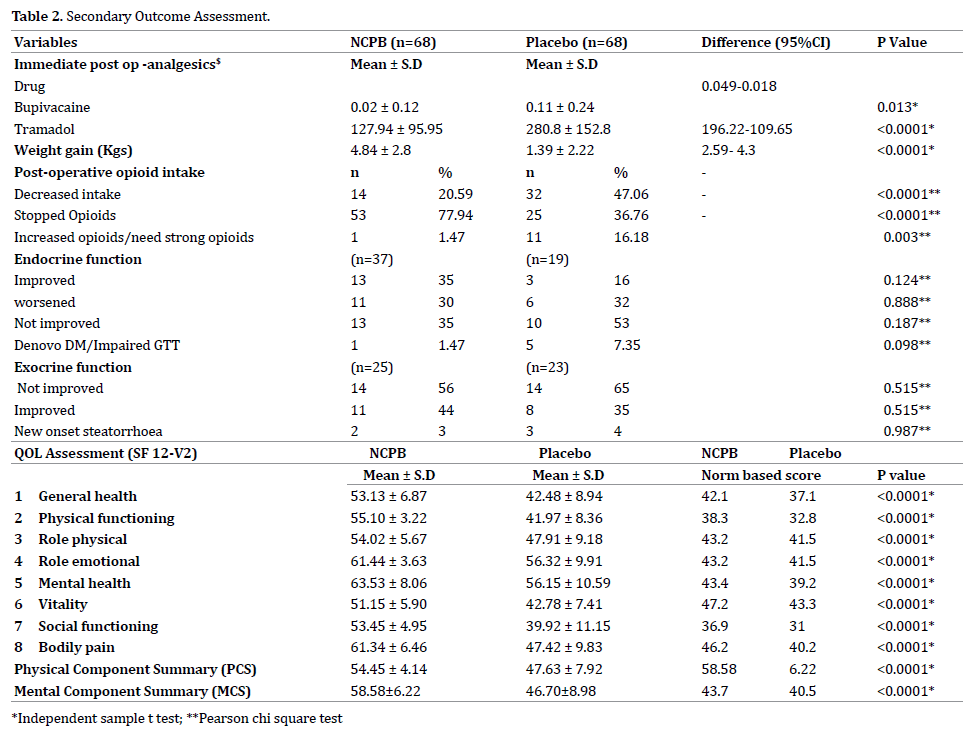
Figure 4: The reduction in the Izbicki score in percentage when comparing the preoperative values of both groups is represented.
There was a significant reduction in dose and number
of patients requiring post-operative epidural analgesics
injection. 77.9% of patients in group I had completely
stopped opioids compared to only 36.8% in group II
(p=<0.0001). In group II 44.6% of patients had opioid
dependency when compared to 15.6% in group I. One
patient in group I (1.47 %) and 11 patients in group II
(16.18%) required increased dose of opioids or required
stronger opioids which represented a failure of the
procedure. Mean weight gain significantly high in group
I. In both groups there was an improvement in exocrine
function but this was not statistically significant (P=0.833).
There was a non-significant decrease (35%) in insulin/
OHA intake in group I. Interestingly; all six new onset DM
patients underwent distal resection (40%).
Quality of Life (QOL)
The QOL at 6 months of follow up showed a significant
improvement in group I patients (p<0.05). Both Physical
and Mental Health Composite Scales were better in group
I (Table 2).
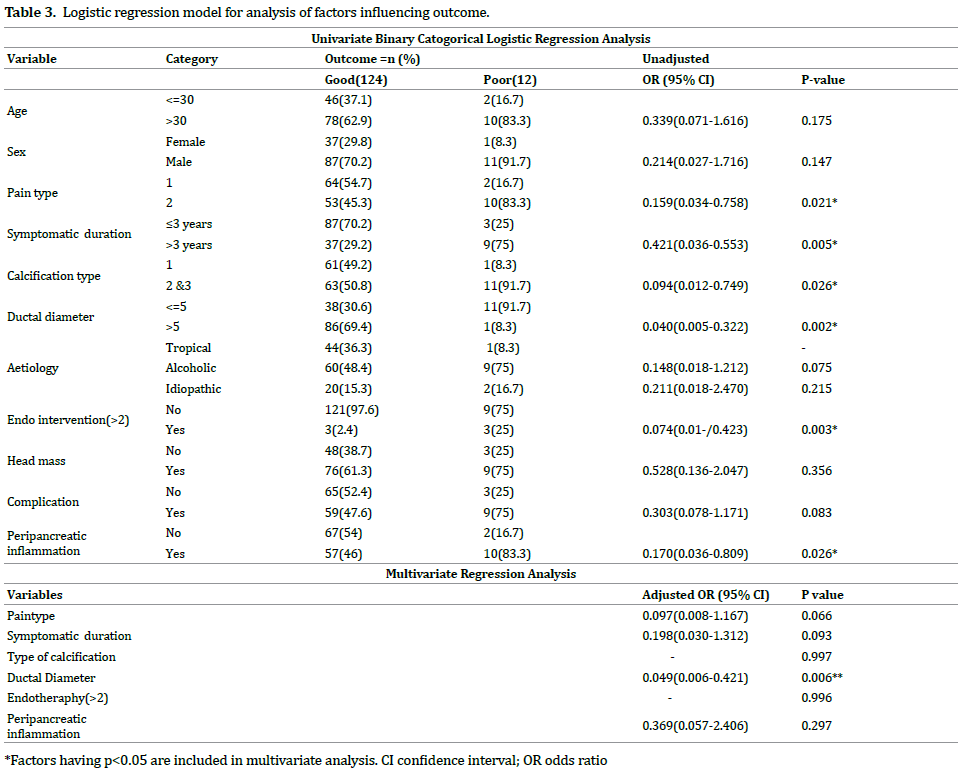
FINAL OUTCOME ANALYSIS
The final success rate of the procedure was 98.5 %
in group I and 83.8% in group II (P=0.003). Even though
univariate analysis showed six parameters were having
an association with outcome, (Table 3) multivariate
analysis showed significance only for those having small
duct disease (p=0.006, OR 0.049; 95% CI, 0.006-0.421) as
shown in previous studies [15].
Non stratified Post–hoc analysis of the sub group of
patients having small ductal diameter (n=49) was done
to know which group of patients are good responders to
treatment (Table 4, Figure 5). In patients with ductal
diameter of 4.6-5 mm the pain relief was significant
(p=0.036). The relative risk reduction (RRR) was high for
4.1-4.5 mm diameter and least when the diameter was
between 4.6-5mm (0.34).

Figure 5: Forest plot, representing the Odds ratio with 95% CI for the subgroup of patients with small ductal diameter.
DISCUSSION
Concept of Multimodal Surgical Approach
There are three well known proposed theories for pain
in chronic pancreatitis namely ductal and parenchymal
hypertension, pacemaker and neurogenic theories [1, 16]. Other mechanisms are pancreatic ischemia, acute
exacerbations of CP, and complications from the pancreas.
The various mechanisms of pain namely nociceptive pain,
neuropathic, neurogenic inflammation, neuro immune
interactions are described in various articles [16, 17, 18, 19, 20]. All these mechanisms of pain when suspected must
be addressed to achieve a better result. Requirement of
multidisciplinary approach in the treatment of pain in chronic
pancreatitis is stressed by many authors (SDC.1) [21].
Large duct disease with >7 cm diameter responds well
to drainage procedures. Managing the chronic pancreatitis
with small duct disease is always a daunting task. The
predominant factor in pathogenesis of pain is neurological
[12]. Small ductal diameter is the independent predictor of
poor outcome following Frey’s procedure [15]. Few studies
have claimed that modified ventral pancreas excision
described by Izbicki [8, 12] and drainage procedures
with head coring show promising long term results but
at the cost of parenchymal loss [22]. Thoracoscopic
splanchnicectomy was extensively studied in the treatment
of small duct disease with good results [23].
Randomized controlled trials comparing surgery with
endotherapy have proved that surgery provides long
term pain relief (>80%) [24, 25]. Retrospective studies
[3] have shown that early surgery will benefit the patient
by delaying the endocrine and exocrine insufficiency and
providing better quality of life. As on current practice
the treatments followed after failure of Frey’s procedure
are increasing the dose of opioid analgesics, celiac plexus
block, if needed redo surgery for residual disease [26],
which either increases the cost as an additional procedure
in a separate setting, or increases the dependence of
opioids there by severely affecting the mental well being of the patient. Hence adding celiac plexus neurolysis to the
current standard procedure in a single sitting as a part of
multimodal approach will provide additional benefit to the
patient not only by improving the psychological wellbeing
but also by reducing the opioid intake thereby leading to a
better quality of life (Figure 6).
Figure 6: Multimodal approach, Multifactorial theories of pain in CCP are depicted at the center with the needed procedures at the corner. NCPB should be added to all patients as the extent of the neurogenic component is poorly understood.
Intra Operative Neurolytic Celiac Plexus Block
Celiac plexus is the relay station for all visceral afferent
fibers [2]. There are two groups of celiac ganglia (right and
left) and its most reliable location is in relation to the celiac trunk [27]. Pain caused by cancer or by chronic pancreatitis
which relay through celiac plexus can be treated using
NCPB [28]. It is traditionally used in the form of either USG,
CT or EUS guided techniques [29]. Intraoperative method
of NCPB was used originally for inoperable pancreatic
or advanced GI malignancies for effective pain relief and
offered good QOL [30, 31]. Surgical splanchnicectomy
offered good long term pain relief of about 46% up to
48 months after splanchnicectomy [32]. This technique
is extensively used for small duct disease. NCPB has a
better pain control compared with splanchnicectomy [33]. Intraoperative method of NCPB in combination with
lateral pancreatico jejunostomy was originally studied
for treatment of pain in CCP with a 94.4% pain relief in a
retrospective study of 34 patients. But this study was done
only on patients with large duct disease [12].
Various studies on CPB have shown conflicting results
with an average of 10%-40% long-term benefit beyond 24
weeks [34, 35, 36] with EUS guided techniques scoring over
image guided methods of block [37, 38]. Most of the studies
were done by plexus block using steroids/bupivacaine
rather than neurolysis. Alcohol as neurolytic agent was
studied mainly in pancreatic malignancy with 73%-85%
significant response [39]. But long term results beyond 1
year were not available when alcohol is used as neurolytic
for malignancy as this method is used only in those with
advanced malignancy. Regarding concentration of alcohol
solution we have used only 50% hydrated solution as
alcohol concentration greater than 50% might cause
neurological complications [17, 27]. Bilateral injection is
favored by most of the studies compared to unilateral and
central injections [38].
The basis for celiac plexus block is it abolishes the
visceral afferent sympathetic fibers that pass through the
celiac plexus and ganglion [39]. Upward migration leads to
coronary branch of vagus ablation and leads to hypotension and more downward migration leads to ablation of plexus
around SMA which leads to more diarrheas. Splanchnic
vasodilatation caused by sympathetic blockade produces
both diarrhea &postural hypotension. It is usually mild
and manageable with crystalloid solutions [40, 41]. Its
incidence was higher when more injections injected below
the level of celiac axis and when a bilateral neurolysis was
performed. Hence we always inject more (30 ml) above
the celiac axis and 10 ml below in a 4 quadrant manner
and maintaining the patient in 45 degree head up position
for about 15 minutes meanwhile preparing the jejunal
loop for anastomosis to avoid upward diffusion of drug.
Possibly this could have produced lesser incidence of
intra operative hypotension in our series but with more
incidence of diarrhea and postural hypotension. The local
injection related pain, referred shoulder pain, paraplegia,
chronic debilitating diarrhea [27, 41] were never occurred
in our study population.
Benefit of celiac plexus block (CPB) was least with
previous pancreatic surgery and repeat blocks were
unhelpful [34]. Hence it is always better to assess the
patients at risk of developing recurrent pain and do it
intra-operatively in a single sitting. In contrast to previous
studies in which the effect of percutaneous NCPB is less
in chronic pancreatitis when compared to malignancy due to adhesions which limits the diffusion of drug40, our
study has proved that neurolysis in chronic pancreatitis
using intraoperative method is effective as the diffusion
of drug is better when injecting the drug at 4 quadrants
in a controlled manner, when compared with radiological
and endoscopic techniques. If recurrence of pain occurs
repeated blocks after a neurolysis can be done even
though we had difficulty in 36% using conventional
percutaneous method. We want to express our view that
there is a difference in pain relief according to the mode
of neurolysis and this intra operative method is an easy,
controlled and better way of neurolysis even though it is
operator dependent. The diffusion of the drug is better,
bilateral injections can be done without change in position
unlike in EUS and percutaneous techniques and it can be
easily done by the operating surgeon himself without a
need for an endoscopic or interventional expertise more
importantly without adding much cost to the procedure in
a single sitting.
NCPB achieves better results in patients with small duct
disease. Smaller the diameter better is the response. But
if the patient is not responding to any kind of analgesics
and neurolysis prior to surgery (centralized pain state
[19]) the response to NCPB is still poor. The success rate
of the procedure in placebo group is fairly comparable to
previous study results (80-90%).There is even decrease in
early post-operative pain in NCPB group. The exact reason
for this is not known. But the possible mechanism that could
have caused this difference may be, less post-operative
ileus thereby decrease in the abdominal distension and
eventually the parietal wound pain.
NCPB improves weight gain significantly. It may be
explained by very good pain control and increased caloric
intake. The 35% decrease in insulin/OHA intake in group
I may be explained by the improved nutrition and mental
wellbeing with possible effect on diabetic status.
NCPB improves the QOL in all types of pancreatitis.
Various studies and RCTs on celiac plexus block also have
shown to improve QOL in both chronic pancreatitis and
unresectable pancreatic cancer [2, 41, 42]. SF36 is routinely
used for assessing the QOL in pancreatic pathology. SF -12
version 2 questionnaire is equally good compared to SF 36
and EORTC Qlq–C30 for evaluation of QOL in pancreatic
pain due to CP [43, 44, 45]. It is more reliable and easier
to use.
Since opiate dependency with annoying side effects,
increases the chances of centralized pain state [19] we
strongly believe that adding neurolysis definitely had
an additional benefit to these patients when combined
with a standard procedure especially addressing the
unidentifiable neurogenic mechanism rather than as an
adjunct to incomplete surgery.
CONCLUSIONS
In accordance with the suggested multifactorial origin
of pancreatitis pain and to address all well-known theories thereby improving the QOL, we suggest combined NCPB
with Frey’s procedure for a complete solution in a single
sitting without affecting the morbidity and mortality.
LIMITATIONS & SUGGESTIONS TO IMPROVE
The injection of alcohol is operator dependent. Better
methods to identify the plexus/ganglion intraoperatively
and finding better agent for neurolysis may improve the
long term effectiveness of the neurolysis. This article may
shed some light on future combinations like neurolysis
with intraoperative lithotripsy [46], splanchnicectomy etc.
which can also theoretically give better results.
ACKNOWLEDGEMENTS
I sincerely thank our patients for participating in this
study. Dr. Moses Vikraman Amarjyothi helped in English
verification of the manuscript. Ms. Jegadeeswari helped in
the data collection. Dr. Mohammed Ali & Dr. Heber David
helped in statistical verification.
This trial was registered at clinical trial.gov.
NCT02735330.The interim analysis data were presented
at AP-HPBA meet at Singapore March 2105 and awarded
as best paper.
Conflict of Interest
The authors have no conflicts of interests to declare.
References
- Sakorafas GH, Tsiotou A, Peros G. Mechanisms and Natural History of Pain in Chronic Pancreatitis. J Clin Gastroenterol 2007; 41:689-699. [PMID: 17667054]
- Erdek MA, Halpert DE, González Fernández M, Cohen SP. Assessment of Celiac Plexus Block and Neurolysis Outcomes and Technique in the Management of Refractory Visceral Cancer Pain. Pain Med 2010; 11:92- 100. [PMID: 20002595]
- Ahmed Ali U, Nieuwenhuijs VB, van Eijck CH, Gooszen HG, van Dam RM, Busch OR, et al. Clinical Outcome in Relation to Timing of Surgery in Chronic Pancreatitis. Arch Surg 2012; 147. [PMID: 23117832]
- Adams D, Ford MC, Anderson MC. Outcome after Lateral Pancreaticojejunostomy for Chronic Pancreatitis. Ann Surg 1994; 219:481-489. [PMID: 8185399]
- Nealon WH, Thompson JC. Progressive Loss of Pancreatic Function in Chronic Pancreatitis Is Delayed by Main Pancreatic Duct Decompression A Longitudinal Prospective Analysis of the Modified Puestow Procedure. Ann Surg 1993; 217:458-468. [PMID: 8489308]
- Strate T, Taherpour Z, Bloechle C, Mann O, Bruhn J, Schneider C, et al. Long-term Follow-up of a Randomized Trial Comparing the Beger and Frey Procedures for Patients Suffering From Chronic Pancreatitis. Ann Surg 2005; 241:591-598. [PMID: 15798460]
- Izbicki J, Bloechle C, Knoefel W, Kuechler T, Binmoeller K, Broelsch C. Duodenum-Preserving Resection of the Head of the Pancreas in Chronic Pancreatitis A Prospective, Randomized Trial. Ann Surg 1995; 221:350- 358. [PMID: 7726670]
- Izbicki JR, Bloechle C, Knoefel WT, Kuechler T, Binmoeller KF, Broelsch CE. Longitudinal V-Shaped Excision of the Ventral Pancreas for Small Duct Disease in Severe Chronic Pancreatitis. Ann Surg 1998; 227:213-219.[PMID: 9488519]
- Negi S, Singh A, Chaudhary A. Pain relief after Frey's procedure for chronic pancreatitis. Br J Surg 2010; 97:1087-1095. [PMID: 20632276]
- Sinha A, Patel Y, Cruise M, Matsukuma K, Zaheer A, Afghani E, et al. Predictors of Post-Operative Pain Relief in Patients with Chronic Pancreatitis Undergoing the Frey or Whipple Procedure. J Gastrointest Surg 2016; 20:734-740. [PMID: 26813017]
- Ni Q, Yun L, Roy M, Shang D. Advances in surgical treatment of chronic pancreatitis. World J Surg Onc 2015; 13:34. [PMID: 25845403]
- Chan C, Vilatobá M, Bartolucci A, Vickers S. Improved reduction in pain in chronic pancreatitis with combined intraoperative celiac axis plexus block and lateral pancreaticojejunostomy. Curr Surg 2001; 58:220-222. [PMID: 11275249]
- Basinski A. Effect of NCPB and VSPL on pain and quality of life in chronic pancreatitis patients. World J Gastroenterol 2005; 11:5010. [PMID: 16124055]
- Rajendran R, Amudhan A, Prabhakaran R, Duraisamy B, Vellaisamy R, Kannan D, et al. Head coring for chronic calcific pancreatitis without pancreatic head mass: Short-term outcome analysis. Int J Hepatobiliary Pancreat Dis 2014; 4:62-69.
- Amudhan A, Balachandar T, Kannan D, Rajarathinam G, Vimalraj V, Rajendran S, et al. Factors affecting outcome after Frey procedure for chronic pancreatitis. HPB 2008; 10:477-482. [PMID: 19088936]
- Di Sebastiano P, di Mola FF, Bockman DE, Friess H, Büchler MW. Chronic pancreatitis: the perspective of pain generation by neuroimmune interaction. Gut 2003; 52:907-911. [PMID: 12740353]
- Puylaert M, Kapural L, Van Zundert J, Peek D, Lataster A, Mekhail N, et al. 26. Pain in Chronic Pancreatitis. Pain Pract 2011; 11:492-505. [PMID: 21676159]
- Xu GY, Winston JH, Shenoy M, Yin H, Pasricha PJ. Enhanced excitability and suppression of A-type K+ current of pancreas-specific afferent neurons in a rat model of chronic pancreatitis. Am J Physiol Gastrointest Liver Physiol 2006; 291:G424-G431. [PMID: 16645160]
- Buscher HC, Wilder-Smith OH, van Goor H. Chronic pancreatitis patients show hyperalgesia of central origin: A pilot study. Eur J Pain 2006; 10:363-363. [PMID: 16087373]
- Vera-Portocarrero L, Westlund K. Role of Neurogenic Inflammation in Pancreatitis and Pancreatic Pain. Neurosignals 2005; 14:158-165. [PMID: 16215298]
- Ihse I, Andersson R, Axelson J. Pancreatic Pain: Is There a Medical Alternative to Surgery? Digestion 1993; 54:30-34. [PMID: 7693532]
- Ramesh H, Jacob G, Lekha V, Venugopal A. Ductal drainage with head coring in chronic pancreatitis with small-duct disease. J Hepatobiliary Pancreat Surg 2003; 10:366-372. [PMID: 14598137]
- Bradley EL 3rd, Reynhout JA, Peer GL. Thoracoscopic splanchnicectomy for small duct chronic pancreatitis: case selection by differential epidural analgesia. J Gastrointest Surg 1998; 2:88-94. [PMID: 9841973]
- Díte P, Ruzicka M, Zboril V, Novotný I. A Prospective, Randomized Trial Comparing Endoscopic and Surgical Therapy for Chronic Pancreatitis. Endoscopy 2003; 35:553-558. [PMID: 12822088]
- Cahen DL, Gouma DJ, Nio Y, Rauws EA, Boermeester MA, Busch OR, et al. Endoscopic versus Surgical Drainage of the Pancreatic Duct in Chronic Pancreatitis. N Engl J Med 2007; 356:676-684. [PMID: 17301298]
- Shrikhande S, Kleeff J, Friess H, Buchler M. Management of Pain in Small Duct Chronic Pancreatitis. J Gastrointest Surg 2006; 10:227-233. [PMID: 16455455]
- Leung JW, Bowen-Wright M, Aveling W, Shorvon PJ, Cotton PB. Coeliac plexus block for pain in pancreatic cancer and chronic pancreatitis. Br J Surg 1983; 70:730-732. [PMID: 6640255]
- Bradley EL 3rd, Bem J. Nerve Blocks and Neuroablative Surgery for Chronic Pancreatitis. World J Surg 2003; 27:1241-1248. [PMID: 14534823]
- Davies DD. Incidence of Major Complications of Neurolytic Coeliac Plexus Block. J R Soc Med 1993; 39:341. [PMID: 8505748]
- Flanigan DP, Kraft RO. Continuing Experience with Palliative Chemical Splanchnicectomy. Arch Surg 1978; 113:509. [PMID: 7683868]
- Gardner AM, Solomou G. Relief of the pain of unresectable carcinoma of pancreas by chemical splanchnicectomy during laparotomy. Ann R Coll Surg Engl 1984; 66:409. [PMID: 6210013]
- Buscher HC, Jansen JB, van Dongen R, Bleichrodt RP, van Goor H. Long-term results of bilateral thoracoscopic splanchnicectomy in patients with chronic pancreatitis. Br J Surg 2002; 89:158-162. [PMID: 11856127]
- Basinski A, Stefaniak T, Vingerhoets A, Makarewicz W, Kaska L, Stanek A, et al. Effect of NCPB and VSPL on pain and quality of life in chronic pancreatitis patients. World J Gastroenterol 2005; 11:5010. [PMID: 16124055]
- Gress F, Schmitt C, Sherman S, Ciaccia D, Ikenberry S, Lehman G. Endoscopic ultrasound-guided celiac plexus block for managing abdominal pain associated with chronic pancreatitis: a prospective single center experience. Am J Gastroenterol 2001; 96:409-416. [PMID: 11232683]
- Gress F, Schmitt C, Sherman S, Ikenberry S, Lehman G. A prospective randomized comparison of endoscopic ultrasound- and computed tomography-guided celiac plexus block for managing chronic pancreatitis pain. Am J Gastroenterol 1999; 94:900-905. [PMID: 10201454]
- Harada N, Wiersema M, Wiersema L. Endosonography guided celiac plexus neurolysis (EUS CPN) for abdominal pain: Comparison of results in patients with chronic pancreatitis versus malignant disease. Gastrointestinal Endoscopy 1997; 45:AB30.
- Markowitz JS, Rattner DW, Warshaw AL. Failure of Symptomatic Relief After Pancreaticojejunal Decompression for Chronic Pancreatitis. Arch Surg 1994; 129:374. [PMID: 8154964]
- Wyse J, Chen YI, Sahai AV. Celiac plexus neurolysis in the management of unresectable pancreatic cancer: When and how? World J Gastroenterol 2014; 20:2186-92. [PMID: 24605017]
- Arcidiacono PG, Rossi M. Celiac Plexus Neurolysis. JOP. 2004; 5:315- 321. [PMID: 15254367]
- Leung JW, Bowen-Wright M, Aveling W, Shorvon PJ, Cotton PB. Coeliac plexus block for pain in pancreatic cancer and chronic pancreatitis. Br J Surg 1983; 70:730-732. [PMID: 6640255]
- Polati E, Luzzani A, Schweiger V, Finco G, Ischia S. The Role of Neurolytic Celiac Plexus Block in the Treatment of Pancreatic Cancer Pain. Transplant Proc 2008; 40:1200-1204. [PMID: 18555148]
- Wong G, Schroeder D, Carns P, Wilson J, Martin D, Kinney M, et al. Effect of Neurolytic Celiac Plexus Block on Pain Relief, Quality of Life, and Survival in Patients With Unresectable Pancreatic Cancer. JAMA 2004; 291:1092. [PMID: 14996778]
- Pezzilli R, Bini L, Fantini L, Baroni E, Campana D, Tomassetti P, et al. Quality of life in chronic pancreatitis. World J Gastroenterol 2006; 12:6249. [PMID: 17072944]
- Pezzilli R, Morselli-Labate A, Fantini L, Campana D, Corinaldesi R. Assessment of the quality of life in chronic pancreatitis using Sf-12 and EORTC Qlq-C30 questionnaires. Dig Liver Dis 2007; 39:1077-1086. [PMID: 17692582]
- D'Haese JG, Ceyhan GO, Demir IE, Tieftrunk E, Friess H. Treatment options in painful chronic pancreatitis: a systematic review. HPB 2014; 16:512-521. [PMID: 24033614]
- Rios GA, Adams DB. Does intraoperative electro hydraulic lithotripsy improve outcome in the surgical management of chronic pancreatitis? Am Surg 2001; 67:533-7; discussion 537-8. [PMID: 11409800]







