Keywords
Carcinoma, Pancreatic Ductal; Disease Management; Neoplasms, Cystic, Mucinous, and Serous
What Did We Know Before ASCO 2014?
Intraductal papillary mucinous neoplasm (IPMN) is a cystic neoplasm of the epithelium of the main pancreatic duct and its branches. It is believed to be a precursor of invasive ductal carcinoma. The risk of malignancy is predicted to be between 20 and 50 % [1]. In one review of the natural history of IPMN, it was concluded that IPMNs involving the branches of the main pancreatic duct are less aggressive than main-duct IPMNs (invasive carcinoma and carcinoma in situ were present in approximately 70% of surgically removed main-duct IPMNs) [2].
The International Association of Pancreatology (IAP) advises resection of main-duct IPMN but recommends guiding the treatment of branch-duct IPMN based on several features of the disease that are likely to indicate invasiveness [1]. The Sendai Consensus Guidelines were also developed to help guide therapy of IPMN. They were first released in 2006 and then modified in 2012 and recommend resection of main-duct IPMN while encourage a more conservative approach in the management of branch-duct IPMN which depends on certain aspects of the neoplasm (size, duct caliber, presence of pancreatitis, characteristics of nodules, etc) [1].
Despite the available data on malignant risk prediction, it remains challenging to stratify IPMN and thus chose the optimal treatment strategy.
What Did We Learn at ASCO 2014?
Comparative Outcomes of Patients with Intraductal Papillary Mucinous Neoplasm Associated Cancer (IPMN-Ca) to Those with Pancreatic Ductal Carcinoma (PDAC) Following Resection [3]
Krishna et al. presented comparative data from a retrospective review that looked at outcomes after resection of Pancreatic Ductal Carcinomas and pancreatic cancer associated with IPMN (IPMN associated cancer) (Table 1)[3]. The review consisted of 225 patients who had resection of Pancreatic Cancer; 186 had PDAC and 39 had IPMN-Ca. After performing univariate analysis of two broad categories of variables (Categorical and Continuous variables), PDAC was more likely to be found in younger patients, present in the head of the pancreas, cause perineural and lymphovascular invasion, differentiate poorly, have a more advanced T and N stages and was more likely to recur. The difference in time to recurrence and clear surgical margin did not reach statistical significance (p of 0.52, and p of 0.23, respectively).
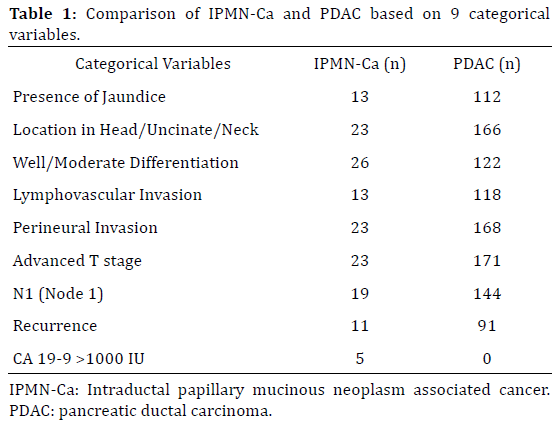
The authors then conducted that multivariate analysis by using only the variables which showed statistically significant difference between PDAC and IPMN-Ca and concluded that both conditions were not significantly different in survival or recurrence.
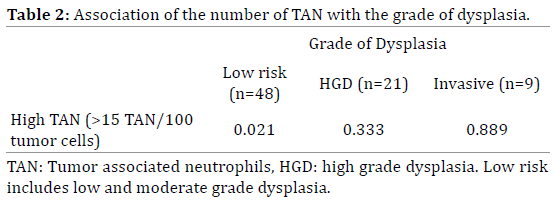
Infiltrating Neutrophils and Malignant Progression in Intraductal Papillary Mucinous Neoplasms (IPMN): An Opportunity for Identification of High-Risk Disease [4]
Sadot et al. studied the relationship between the number of tumor associated neutrophils (TAN) in IPMN and malignant progression [4]. They divided 78 samples of IPMN into three groups based on the degree of dysplasia: low risk (included both low and moderate grade dysplasia), high grade dysplasia and invasive carcinoma. The number of TAN was measured per 100 tumor cells (Table 2). The authors reported higher numbers of TAN in tumors with higher grades of dysplasia. They also quantified the concentrations of inflammatory proteins (IP) including IFN-g, TIMP-1, MIF, TNF-a, and MMP-9 in the cyst fluid and noted that higher numbers of TAN are associated with higher concentrations of IP and higher grades of dysplasia. They concluded that the number of TAN and the risk of malignant progression are strongly correlated.
Discussion
IPMNs have a potential to become malignant, therefore the need to better characterize this class of tumors to guide management.
Regarding diagnosis, different imaging modalities have been implemented with EUS along with FNA being widely used for diagnosis. Iannicelli et al. mentioned the use of MRCP with Secretin stimulation to be able to better visualize the communication between the neoplasm and the ductal system and thus confirm the diagnosis [5]. Chen et al. found that contrast-enhanced sonography proved to be helpful in discerning branch duct IPMN from serous cystadenomas [6].
Managing IPMN’s remains challenging. The Sendai Consensus Guidelines (SCG) have been widely used but they remain controversial regarding the approach to the treatment of branch duct IPMN. Goh et al. looked into the effectiveness of the SCG in predicting the risk of malignant progression. The positive predictive value (PPV) of SCG positive neoplasms stretched from 11 to 52 % and the negative predictive value (NPV) of SCG negative neoplasms was shown to be 90 to 100 %. They concluded by stating that the PPV of the SCG was low and therefore cannot detect effectively high risk branch duct IPMN [7]. Consequently, understanding the molecular biology of the disease may be a better means to reveal high risk tumors which was reinforced by Shi et al. [8].
What we know so far about the molecular pathogenesis of IPMN is limited. KRAS has been found mutated in approximately 50 % of IPMNs [9]. BRAF and PIK3CA are also found frequently in IPMNs but at a lower frequency than KRAS [10, 11].
The abstract #4137 discusses a novel method of predicting malignancy risk in IPMN. A higher number of infiltrating neutrophils inside the tumor and higher levels of inflammatory proteins inside the cystic fluid seem to correlate with the degree of dysplasia and carcinoma [4]. This finding broadens our understanding of the disease and validates that knowledge of the molecular pathogenesis of the disease is key to identify high risk disease and thus guide therapy.
Winner et al. concluded that invasive tumors recur more often [12].
The comparison of outcomes of invasive IPMN and sporadic pancreatic adenocarcinoma was performed by Wasif et al. They deduced that lymph node-negative invasive IPMN had better survival than lymph node-negative pancreatic adenocarcinoma but outcomes were not different for lymph node-positive invasive IPMN and lymph nodepositive pancreatic adenocarcinoma [13]. Another comparative study was done by Woo et al. and elucidated that nonmetastatic invasive IPMN carries a better survival (a 5-year survival of 33.9%) than nonmetastatic pancreatic adenocarcinoma (a 5-year survival of 9%) but the latter observation did not apply to metastatic IPMN [14].
The comparative study conducted by Krishna et al. was different in that compared IPMN related cancer and pancreatic ductal carcinoma after resection. It showed no significant difference in survival between pancreatic ductal carcinoma and IPMN related cancer after resection. The authors closed by stating that IPMN related Ca should be included in adjuvant trials for Pancreatic cancer as it is not different from pancreatic ductal carcinoma in terms of survival. The latter conclusion might affect the inclusion criteria of adjuvant therapy trials in the future [3].
In summary, our knowledge of IPMN has been growing markedly and will be more directed toward understanding the molecular biology of the disease which will help stratify patients and provide optimal treatment. Invasive IPMN seems to have a poor prognosis similar to that of ductal carcinoma, more efforts should be made to better characterize it.
Conflict of Interest
The authors have no potential conflict of interest.
References
- Correa-Gallego C, Do R, Lafemina J, Gonen M, D'Angelica MI, DeMatteo RP, Fong Y, et al. Predicting dysplasia and invasive carcinoma in intraductal papillary mucinous neoplasms of the pancreas: development of a preoperative nomogram. Ann Surg Oncol. 2013; 20: 4348-55. [PMID:24046103]
- Bassi C, Sarr MG, Lillemoe KD, Reber HA. Natural history of intraductal papillary mucinous neoplasms (IPMN): current evidence and implications for management. J Gastrointest Surg. 2008; 12: 645-50. [PMID:18097728]
- Krishna K, Bloomston M, Muscarella P, Krishna S, Wei L, Conwell D, Bekaii-Saab TS. Comparative outcomes of patients with intraductal papillary mucinous neoplasm associated cancer (IPMN-Ca) to those with pancreatic ductal carcinoma (PDAC) following resection. J Clin Oncol. 2014; 32. Abstract e15227.
- Sadot E, Basturk O, Klimstra DS, Gonen M, et al. Infiltrating neutrophils and malignant progression in intraductal papillary mucinous neoplasms (IPMN): An opportunity for identification of high-risk disease. J Clin Oncol. 2014; 32: 5s. Abstract 4137.
- Iannicelli E, Carbonetti F, Di Pietropaolo M, Federici GF, Capurso G, David V. Magnetic resonance cholangiopancreatography with secretin stimulation in the diagnosis of intraductal papillary mucinous neoplasm: a paradigmatic case report. Case Rep Radiol. 2014; 2014: 820359. [PMID:24716074]
- Chen F, Liang JY, Zhao QY, Wang LY, Li J, Deng Z, Jiang TA. Differentiation of branch duct intraductal papillary mucinous neoplasms from serous cystadenomas of the pancreas using contrast-enhanced sonography. J Ultrasound Med. 2014; 33: 449-55. [PMID:24567456]
- Goh BK, Tan DM, Ho MM, Lim TK, Chung AY, Ooi LL. Utility of the Sendai Consensus Guidelines for Branch-Duct Intraductal Papillary Mucinous Neoplasms: A Systematic Review. J Gastrointest Surg. 2014; 18: 1350-7 [PMID:24668367]
- Shi C, Hruban RH. Intraductal papillary mucinous neoplasm. Hum Pathol. 2012; 43: 1-16. [PMID:21777948] 9. Grutzmann R, Niedergethmann M, Pilarsky C, Kloppel G, Saeger HD. Intraductal papillary mucinous tumors of the pancreas: biology, diagnosis, and treatment. Oncologist. 2010; 15: 1294-309. [PMID:21147870]
- Grutzmann R, Niedergethmann M, Pilarsky C, Kloppel G, Saeger HD. Intraductal papillary mucinous tumors of the pancreas: biology, diagnosis, and treatment. Oncologist. 2010; 15: 1294-309. [PMID:21147870]
- Schönleben F, Qiu W, Bruckman KC, Ciau NT, Li X, Lauerman MH, Frucht H, et al. BRAF and KRAS gene mutations in intraductal papillary mucinous neoplasm/carcinoma (IPMN/IPMC) of the pancreas. Cancer Lett. 2007; 249: 242-8. [PMID:17097223]
- Schonleben F, Qiu W, Remotti HE, Hohenberger W, Su GH. PIK3CA, KRAS, and BRAF mutations in intraductal papillary mucinous neoplasm/ carcinoma (IPMN/C) of the pancreas. Langenbecks Arch Surg. 2008; 393: 289-96. [PMID:18343945]
- Winner M, Epelboym I, Remotti H, Lee JL, Schrope BA, Chabot JA, Allendorf JD. Predictors of recurrence in intraductal papillary mucinous neoplasm: experience with 183 pancreatic resections. J Gastrointest Surg. 2013; 17: 1618-26. [PMID:23813047]
- Wasif N, Bentrem DJ, Farrell JJ, Ko CY, Hines OJ, Reber HA, Tomlinson JS. Invasive intraductal papillary mucinous neoplasm versus sporadic pancreatic adenocarcinoma: a stage-matched comparison of outcomes. Cancer. 2010; 116: 3369-77. [PMID:20564064]
- Woo SM, Ryu JK, Lee SH, Yoo JW, Park JK, Kim YT, Yoon YB. Survival and prognosis of invasive intraductal papillary mucinous neoplasms of the pancreas: comparison with pancreatic ductal adenocarcinoma. Pancreas. 2008; 36: 50-5. [PMID:18192881]

