Keywords
Carcinoma, Pancreatic Ductal; Cytokines; Early Detection of Cancer; T-Lymphocytes, Regulatory
INTRODUCTION
Intraductal papillary mucinous neoplasms (IPMN) have been reported to account for approximately 7% of clinically diagnosed pancreatic neoplasms and up to 50% of incidentally detected pancreatic cysts [1]. Since the initial description of IPMN by Ohashi et al. [2], the incidence of these mucin-producing epithelial tumors of the exocrine pancreas has been increasing [3]. This is probably attributed to improvements in technology and diagnostic imaging as well as more distinct nomenclature [1]. The World Health Organization (WHO) introduced the term “intraductal papillary mucinous tumor” in 1996, which was later renamed as IPMN in 2000 [4, 5].
IPMN may manifest as recurrent pancreatitis, with or without hyperamylasemia, steatorrhea, diabetes, and weight loss. On the other hand, patients may be entirely asymptomatic, with a tumor found on imaging performed for a different indication. On imaging, IPMN appears as a dilated pancreatic duct, full of mucin, which extrudes through a bulging papilla. Tumors may arise from the main duct, side-branches, or they may display a mixed pattern of involvement. They also exhibit a wide range of histopathological behavior, from benign adenoma to invasive adenocarcinoma, with borderline tumors and carcinoma in situ in between these extremes [6]. In a recent study, 42% of main duct IPMNs were found to be malignant, and 27% of patients with main duct tumors were asymptomatic [7]. Of less concern are branch duct IPMNs, without mural nodes, as they seem to be very slow to develop into adenocarcinoma and some recommend against surgery if they are found [8, 9]. New screening tools, in addition to endoscopic ultrasound and magnetic resonance imaging are needed to assist in classification of premalignant lesions having a high likelihood for progression and which will benefit from wider surgical margins.
Here, we review some new information on potential biomarkers for classifying IPMNs by examining cyst aspirate cytokine levels (Abstract #133) [10] and peripheral Foxp3/CD4/CD25 levels (Abstract #148) [11] in patients with newly discovered IPMNs (Table 1).

Updates from the 2010 ASCO Gastrointestinal Cancers Symposium
Abstract #133: Cyst fluid cytokines to distinguish lowand high-risk intraductal papillary mucinous neoplasms (IPMN) [10]
Cyst formation in the pancreas may induce or produce an immunological response and could result in release of cytokines or other soluble factors into cyst fluid that could correlate with the risk of having a high risk IPMN. Before surgical resection, pancreatic cyst fluid was aspirated from 40 patients. Patients were then grouped based on the grade of dysplasia in resected tissue. Cyst fluid cytokine levels (IL-2, 4, 5, 8, 10, 12, 13, TNF-alpha, IFN-gamma) were determined using a multiplex ELISA methodology.
Of the cytokines measured, both IL-1beta and IL-8 levels were found elevated in patients’ cyst fluid with high-grade dysplasia. IL-1beta levels in low-grade dysplasia were 0.2±0.1 pg/mL and 539±255 pg/mL in high grade group. Cyst IL-8 levels were 2,893±836 pg/mL and 8,089±2,288 pg/mL in low vs. high grade lesions respectively.
IL-1beta is a cytokine produced principally by mononuclear phagocytes but also by various other cells types including keratinocytes, epithelium and cells of the central nervous system. Elevated levels of IL-1beta have been implicated in sepsis, cachexia, rheumatoid arthritis, chronic myelogenous leukemia, asthma, psoriasis, inflammatory bowel disease, anorexia, AIDS, and graft-versus-host disease associated with bone marrow transplants. In addition, medical literature indicates that IL-1beta is one of the key mediators of immunobiological responses to physical stress. IL-8 is produced by stimulated monocytes, macrophages, fibroblasts, endothelial cells, keratinocytes, melanocytes, hepatocytes, chondrocytes, and a number of tumor cell lines. Elevated concentrations of IL-8 have been observed in patients with psoriasis, rheumatoid arthritis, chronic polyarthritis, tumor development and hepatitis C.
The source of these cytokines could be interesting and future studies may want to investigate the immunophenotype of cells found in cyst in addition to immunohistological localization of these cytokines and associated cells in the tumor microenvironment to see how they are interrelated and if there are any other biomarkers that may be predictive of malignant IPMN.
Abstract #148: Evaluation of Foxp3/CD4/CD25/t cell (Treg) in peripheral blood as a biomarker for the aggressiveness of intraductal papillary mucinous neoplasm [11]
Differentiating and predicting the benign and potentially malignant forms of IPMN located in ductal adenomas is sometimes a challenge. More methods are needed to help in predicting benign from malignant forms of IPMN. Recent studies have found increased Foxp3/CD25/CD4 cells in IPMN tumors and their presence heralds a worse prognosis [12]. Foxp3/CD25/CD4 cells can also be found in peripheral blood, and Ikemoto et al. previously reported that the percentage of peripheral Foxp3+, CD4+, CD25 T-cells were increased in patients with advanced pancreatic cancer [13].
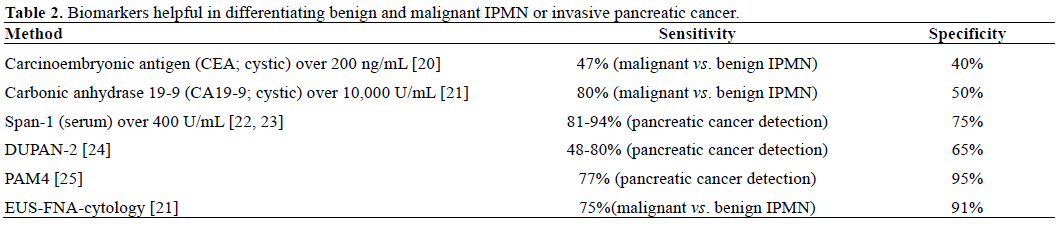
The work presented at the 2010 ASCO Gastrointestinal Cancers Symposium is a continuation of this line of research in the setting of benign and cancerous IPMN types focusing on the percentage of peripheral Foxp3+ T-regulatory cells in tumor and blood in relation to histological aggressiveness of resected IPMNs and recurrence. They were able to show that patients with peripheral T-regulatory cells levels below 2.5% had no recurrence after surgery. Conventional tumor markers, CEA, CA 19-9, Span-1, and DUPAN-2 showed no correlation to the aggressive nature of the IPMNs and preoperative imaging only had a weak correlation. Histological aggressiveness was also positively correlated with the number of Foxp3+ T-regulatory cells in resected tumors.
These results are promising because the peripheral Foxp3 levels seemed to correlate better than many conventional tumor markers with tumor aggressiveness. Since cyst fluid contains cytokines and other factors that may help recruit T-regulatory cells, it would be interesting to isolate these T-regulatory cells and determine what type of immunokines they are producing to see if any of these are potential biomarkers for malignant potential of IPMN (Table 2).
Discussion
IPMN is a disease of the ductal epithelium. There is a progression in the degree of dysplasia from IPMN adenoma, to borderline IPMN with dysplasia, to IPMN with carcinoma in situ, to invasive carcinoma. This progression is similar to the progression from adenoma to carcinoma that is seen in colorectal carcinoma and the progression of pancreatic intraepithelial neoplasm seen in solid epithelial tumors of the pancreas (Figure 1) [14]. An accumulation of molecular abnormalities is associated with progression from IPMN adenoma to invasive carcinoma, but the time course for progression and the malignant potential for each lesion are unknown. According to early reports [15, 16] invasive carcinoma was present in 35% to 50% of patients diagnosed with IPMN.
Figure 1. Hypothetical progression of IPMN to adenocarcinoma.
Reproduced and modified by permission from Cancer Control,
journal of the Moffitt Cancer Center [26].
The data from these two abstracts raise some interesting possibilities for determining the nature of IPMNs found incidentally or even from symptomatic patients. Cystic cytokines obtained from EUS-FNA, along with peripheral and tissue CD4-regulatory cells, represent two additional markers to help classify the malignant potential of IPMNs and also giving us a window into what is evolving in the tumor microenvironment and host to allow the tumor to progress. Recent work has helped us to appreciate that the tumor microenvironment can be an active participant in the formation or maintenance of a malignancy [17]. Local and systemic cytokines and Tregulatory cells are known to be players in development and maintenance of a malignant phenotype [18, 19]. The ability to monitor these changes locally in the case of cystic cytokines and systemically, in the case of peripheral Foxp3/CD4/CD25 cells is promising. Because of genomic instability, it is likely that IPMNs will evolve different ways to manipulate the local and systemic environment to favor their survival, and in all likelihood, there are other biomarkers which may be discovered that are common in the development of malignant IPMN. As more data is gathered, algorithms combining multiple parameters will help give physicians greater confidence regarding the nature of newly discovered IPMNs. These two abstracts are promising and clinicians should initiate more studies to determine sensitivity and specificity compared to other methodologies to see if incorporating these two biomarkers offers any improvements in classifying IPMNs.
Conflict of interest
The authors have no potential conflicts of interest
References
- Andrejevic-Blant S, Kosmahl M, Sipos B, Kl?ppel G. Pancreatic intraductal papillary-mucinous neoplasms: a new and evolving entity. Virchows Arch 2007; 451:863-9. [PMID 17899180]
- Ohashi K, Murakami Y, Murayama M, Taketoshi T, Ohta T, Ohashi I. Four cases of mucin-secreting cancer of the pancreas on specific findings of the papilla of Vater. Prog Dig Endosc 1982; 20:348.
- Winter JM, Cameron JL, Campbell KA, Arnold MA, Chang DC, Coleman J, et al. 1423 pancreaticoduodenectomies for pancreatic cancer: A single-institution experience. J GastrointestSurg 2006; 10:1199-210. [PMID 17114007]
- Kloppel G, Solcia E, Longnecker DS, Capella C, SobinLH. International histological typing of tumors of the exocrine pancreas. Springer, Berlin 1996.
- Longnecker DS, Adler G, Hruban RH, Kloppel G. Intraductal papillary mucinous neoplasms. In: Hamilton SR, Aaltonen LA (eds): World Health Organization Classification of Tumors Pathology and Genetics of Tumors of the Digestive System Lyon, IARC Press, 2000, pp 237-241.
- Tseng JF, Fernandez-del Castillo C, et al. The cystic neoplasms of the pancreas. In: Blumgart H, Editor, Surgery of the liver, biliary tract, and pancreas, Saunders, London (2006).
- Salvia R, Fern?ndez-del Castillo C, Bassi C, Thayer SP, Falconi M, Mantovani W, et al. Main-duct intraductal papillary mucinous neoplasms of the pancreas: clinical predictors of malignancy and long-term survival following resection. Ann Surg 2004; 239:678-85. [PMID 15082972]
- Tanno S, Nakano Y, Nishikawa T, Nakamura K, Sasajima J, Minoguchi M, et al. Natural history of branch duct intraductal papillary-mucinous neoplasms of the pancreas without mural nodules: long-term follow-up results. Gut 2008; 57:339-43. [PMID 17660227]
- Adsay NV, Volkan N. Intraductal Papillary Mucinous neoplasms of the pancreas from pathogenesis to pathology. Digestive Diseases Week. 2005.
- Maker AV, Brennan MF, DeMatteo RP, D'Angelica MI, Fong Y, JarnaginWR, Allen P. Cyst fluid cytokines to distinguish lowand high-risk intraductal papillary mucinous neoplasms (IPMN). 2010 ASCO Gastrointestinal Cancers Symposium. Abstract No. 133.
- Ikemoto T, Shimada M, Utsunomiya T, Imura S, Morine Y, Hanaoka J, et al. Evaluation of Foxp3/CD4/CD25/t cell (Treg) in peripheral blood as a biomarker for the aggressiveness of intraductal papillary mucinous neoplasm. 2010 ASCO Gastrointestinal Cancers Symposium. Abstract No. 148.
- Hiraoka N, Onozato K, Kosuge T, Hirohashi S. Prevalence of FOXP3+ regulatory T cells increases during the progression of pancreatic ductal adenocarcinoma and its premalignant lesions. Clin Cancer Res 2006; 12:5423-34. [PMID 17000676]
- Ikemoto T, Yamaguchi T, Morine Y, Imura S, Soejima Y, Fujii M, et al. Clinical roles of increased populations of Foxp3+CD4+ T cells in peripheral blood from advanced pancreatic cancer patients. Pancreas 2006; 33:386-90. [PMID 17079944]
- Hruban RH, Goggins M, Parsons J, Kern SE. Progression model for pancreatic cancer. Clin Cancer Res 2000; 6:2969-72. [PMID 10955772]
- Kimura W, Makuuchi M, Kuroda A. Characteristics and treatment of mucin-producing tumor of the pancreas. Hepatogastroenterology 1998; 45:2001-8. [PMID 9951854]
- Yamao K, Ohashi K, Nakamura T, Suzuki T, Shimizu Y, Nakamura Y, et al. The prognosis of intraductal papillary mucinous tumors of the pancreas. Hepatogastroenterology 2000; 47:1129-34. [PMID 11020896]
- Maffini MV, CalabroJM, Soto AM, Sonnenschein C. Stromal regulation of neoplastic development: age-dependent normalization of neoplastic mammary cells by mammary stroma. Am J Pathol 2005; 167:1405-10. [PMID 16251424]
- Hsiao YW, Liao KW, Hung SW, Chu RM. Tumor-infiltrating lymphocyte secretion of IL-6 antagonizes tumor-derived TGF-beta 1 and restores the lymphokine-activated killing activity. J Immunol 2004; 172:1508-14. [PMID 14734728]
- Yu P, Lee Y, Liu W, Krausz T, Chong A, Schreiber H, Fu YX. Intratumor depletion of CD4+ cells unmasks tumor immunogenicity leading to the rejection of late-stage tumors. J Exp Med 2005; 201:779-91. [PMID 15753211]
- Correa-Gallego C, Warshaw AL, Fernandez-del Castillo C. Fluid CEA in IPMNs: A useful test or the flip of a coin? Am J Gastroenterol 2009; 104:796-7. [PMID 19223886]
- Pais SA, Attasaranya S, Leblanc J, Sherman S, Mchenry L, Schmidt M, Dewitt J. Utility of EUS-FNA and cyst fluid analysis in the diagnosis of intraductal papillary mucinous tumors: correlation with histopathology in 74 patients. GastrointestEndosc 2006; 63:AB268.
- Kiriyama S, Hayakawa T, Kondo T, Shibata T, Kitagawa M, Ono H, Sakai Y. Usefulness of a new tumor marker, Span-1, for the diagnosis of pancreatic cancer. Cancer 1990; 65:1557-61. [PMID 2311067]
- Chung YS, Ho JJ, Kim YS, Tanaka H, Nakata B, Hiura A, et al. The detection of human pancreatic cancer-associated antigen in the serum of cancer patients. Cancer 1987; 60:1636-43. [PMID 3476183]
- Goonetilleke KS, Siriwardena AK. Systematic review of carbohydrate antigen (CA19-9) as a biochemical marker in the diagnosis of pancreatic cancer. Eur J SurgOncol 2007; 33:266-70. [PMID 17097848]
- Gold DV, Modrak DE, Ying Z, Cardillo TM, Sharkey RM, Goldenberg DM. New MUC1 serum immunoassay differentiates pancreatic cancer from pancreatitis. J ClinOncol 2006; 24:252-8. [PMID 16344318]
- Klapman J, Malafa MP. Early detection of pancreatic cancer: why, who, and how to screen. Cancer Control 2008; 15:280-7. [PMID 18813195]


