Takatomi Oku1, Masahiro Maeda1, Yuko Wada4, Eriko Waga4, Kaoru Ono4, Yasuhiro Nagamachi1, Shigeyuki Fujii1, Miri Fujita2, Kenjiro Misu3, Naoto Senmaru3, Yasuhiro Suzuki3, Kazuo Nagashima2, Yoshiro Niitsu4
Departments of 1Gastroenterology, 2Pathology, and 3Surgery, Shinnittetsu Muroran General
Hospital. Muroran, Japan
4Department of Internal Medicine (Section 4), Sapporo Medical
University, School of Medicine. Sapporo, Japan
- *Corresponding Author:
- Takatomi Oku
Department of Gastroenterology
Shinnittetsu Muroran General Hospital
1-45 Chiribetsu-cho
Muroran, Hokkaido
050-0076 Japan
Phone: +81-143.44.4650
Fax: +81-143.47.4354
E-mail: takatomioku@hotmail.com
Received January 3rd, 2006 - Accepted January 16th, 2006
Keywords
Adenoma; Oxyphil Cells; Pancreas
Abbreviations
IOPN: intraductal papillary oncocytic neoplasm; MCN: mucinous cystic neoplasm; MPD: main pancreatic duct
INTRODUCTION
Oncocyte is the generally accepted term for cells exhibiting a phenotype which features an abundant eosinophilic granular cytoplasm and ultrastructurally an increase in the number of mitochondria.
In 1932 Jaffe [1] introduced the term oncocytoma to designate a tumor of the salivary glands which predominantly consisted of oncocytes. Although oncocytomas have since been reported in other organs including the thyroid, parathyroid and pituitary glands, the kidney, the ovaries and lungs, tumors predominantly composed of oncocytic cells in the pancreas are extremely rare [2]. Adsay et al. [3] proposed a new disease entity known as an intraductal oncocytic papillary neoplasm (IOPN) of the pancreas in 1996. With only 17 cases reported to date, the clinical and pathological details of IOPNs are still unclear. We herein add one case with different characteristics from those of past reports. To our knowledge, this is the first case report of IOPN with clinical characteristics of a mucinous cystic neoplasm (MCN).
CASE REPORT
A 76-year-old woman presented at our hospital in December 2005 complaining of nausea. Abdominal ultrasonography (US) and enhanced computed tomography (CT) revealed a cystic mass with a maximum diameter of approximately 40 mm located in the body of the pancreas. At the time, she rejected the recommendation for further examinations. Three months later, in March 2006, she was hospitalized when a second CT showed that the rapidly growing cystic mass had a maximum diameter of approximately 60 mm. Her family history and past history were unremarkable. On physical examination, she was 156 cm tall and weighed 62 kg; blood pressure was 120/74 mmHg; pulse was 70 beats/min; and body temperature was 36.4 ºC. There were no abnormal findings in the chest or abdomen.
Laboratory data at admission were within the normal ranges, including peripheral blood leukocyte count (5,550 μL-1, reference range: 3,800-8,000 μL-1), hematocrit (37.1%, reference range: 36.0-52.0%), total bilirubin (0.5 mg/dL, reference range: 0.1-1.0 mg/dL), transaminase (asparatate aminotransferase, AST, 16 IU/L, reference range: 1-38 IU/L; alanine aminotransferase, ALT, 7 IU/L, reference range: 2-40 IU/L), alkaline phosphatase (208 IU/L, reference range: 111-336 IU/L), and serum amylase (163 IU/L, reference range: 54-168 IU/L). Tumor markers were also normal with regard to carcinoembryonic antigen (2.4 ng/mL, reference range: 0-5.0 ng/mL) and carbohydrate antigen CA 19-9 (11.7 U/mL, reference range: 0-37.0 U/mL).
US and endoscopic ultrasonography (EUS) revealed a monolocular cystic mass of approximately 60 mm in the body of the pancreas which contained a 30 mm nodule with a high echo spot indicating calcification, and displacing the splenic and left renal veins (Figure 1). Enhanced CT (Figure 2) showed that the nodular region inside the monolocular cystic mass had a slightly higher density than the cystic region and was not enhanced. The rapid growth of the mass was assessed by comparing findings from March 2006 with previous images from December 2005. Displacement of the splenic and left renal veins was detected as well as findings of EUS. Magnetic resonance imaging revealed that the cystic region generated very high signal intensity on T1-weighted images and high signal intensity on T2-weighted images whereas the nodular part showed a mixture of high and low signal intensities on T2-weighted images (Figure 3). Endoscopy showed that the orifice of the papilla of Vater was normal. Endoscopic retrograde cholangiopancreatography (ERCP) showed stenosis of the main pancreatic duct (MPD) in the body of the pancreas, and mild dilatation of the MPD in the tail. Furthermore, no communication between the mass and the MPD was found (Figure 4). Splenic arteriography did not reveal any encasement or tumor stain, but displacement by the tumor (Figure 5).
Figure 1. a. Abdominal ultrasonography revealing a
monolocular, apparently cystic mass in the body of the
pancreas. This mass contained a 30 mm nodule with a
high echo spot, indicating calcification. Endoscopic
ultrasonography showed findings similar to
ultrasonography (b.) and displacement of the splenic
(c.) and left renal veins (d.).
Figure 2. Enhanced CT images from December 2005
(a., b.) and March 2006 (c., d.). Enhanced CT shows a
monolocular cystic mass with a higher density nodule
relative to a cystic region which was not enhanced. The
rapid growth of the mass was determined by comparing
the findings from December 2005 to those of March
2006. Displacement of the splenic and left renal veins
was found as well in the findings of endoscopic
ultrasonography.
Figure 3. Magnetic resonance imaging revealed very
high signal intensity in T1-weighted images of the
cystic region (a.) and high signal intensity in
T2-weighted images (b.). The nodular region showed a
mixture of high and low signal intensities in
T2-weighted images.
Figure 4. Endoscopic retrograde pancreatography
images of stenosis of the main pancreatic duct in the
body of the pancreas. No communication between the
mass and the main pancreatic duct was detected.
Figure 5. Splenic arteriography revealed displacement
by the tumor, but no encasement and tumor stain.
Based on the findings of these examinations, a diagnosis of MCN with hemorrhagic contents was suspected, and a distal pancreatectomy and splenectomy was performed in April 2006. The surgically resected specimen showed a well-demarcated cystic mass measuring 75x55x50 mm in size and located in the body of the pancreas (Figure 6a). On sectioning, the cystic tumor contained brownish mucous and jelly-like material consisting of blood coagulation with fibrin deposition, which was detected by image examinations. Macroscopic findings indicated that the rapid growth within the short period observed in our case was due to internal hemorrhaging, which is sometimes observed in MCNs, but not intraductal papillary mucinous neoplasms (IPMNs). In addition, there was a nodular papillary projection measuring 10 mm in diameter in the cystic wall (Figures 6b and 7a). Microscopically, the cystic wall was lined by columnar pancreas duct epithelium with occasional micropapillary projections and the nodule was characterized by variably complex, arborizing papillary structures lined with plump cells containing abundant eosinophilic cytoplasm (Figure 7bc). Immunohistochemically, the oncocytic tumor cells stained positively with anti-mitochondrial antibody 113-1 used at a dilution of 1:400 (BioGenex, San Ramon, CA, USA) (Figure 7d). An ovarian-type stroma, a hallmark of MCN, was not found. These pathologic findings led to a diagnosis of IOPN. The low mitotic rate having a mindbomb homolog-1 index of less than 1% and the mild degree of cytoarchitectural atypia warranted the classification of adenoma.
Figure 6. An image of the surgically resected
specimen, showing a cystic mass in the body of the
pancreas (a.). Upon sectioning, the cystic tumor and
the monolocular cysts contained blood coagulation
with fibrin deposition, mucous and a nodular papillary
projection measuring 10 mm in diameter (b.).
Figure 7. Microscopically, the cyst wall was lined by
columnar pancreas duct epithelium with papillary
projections (a. x20), and the papillary tumor was
characterized by variably complex, arborizing
structures which were lined by plump cells with
abundant eosinophilic cytoplasm (b. x100, c. x400).
Immunohistochemically, the cytoplasm of the tumor
cells was filled with anti-mitochondrial antibody (d. x100).
The patient had an uneventful postoperative course. At a 9 month follow-up examination, she was well and without symptoms or evidence of tumor recurrence.
DISCUSSION
Pancreatic tumors with oncocytes have been described as oncocytic changes in endocrine tumors [4] or solid and papillary epithelial tumors [5], or as coming from chronic pancreatitis [6], but they are uncommon with intraductal or cystic tumors of the pancreas. In 1996, Adsay et al. [3] reported a new subgroup of IPMNs. They proposed a new disease entity known as IOPN, which was defined by the following pathologic features: Pancreatic duct lesions signifying complex, arborizing, and proliferating papillary structures, tumor cells with a finely granular, eosinophilic cytoplasm, and diffusely present goblet cells. In addition, the cytoplasm of tumor cells stains diffusely with anti-mitochondrial antibodies. Electron microscopy images show abundant tumor cell cytoplasm rich with mitochondria.
The underlying cause for the increased numbers of mitochondria in oncocytoma has been the subject of several reports. Welter et al. [7] measured an increase in mitochondrial deoxyribonucleic acid (DNA) aberrations which were not accompanied by a parallel rise in mitochondrial ribonucleic acid (RNA) transcripts. These findings, which are compatible with the presence of poorly functioning or nonfunctional mitochondria in oncocytic neoplasms, suggest that the excess of mitochondria may be due to a partial block of mitochondrial RNA transcription or decreased RNA stability. Thus, although the biogenesis of mitochondria in oncocytic cells is obviously abnormal, the relationship of this phenotype to the development of tumors remains obscure [2].
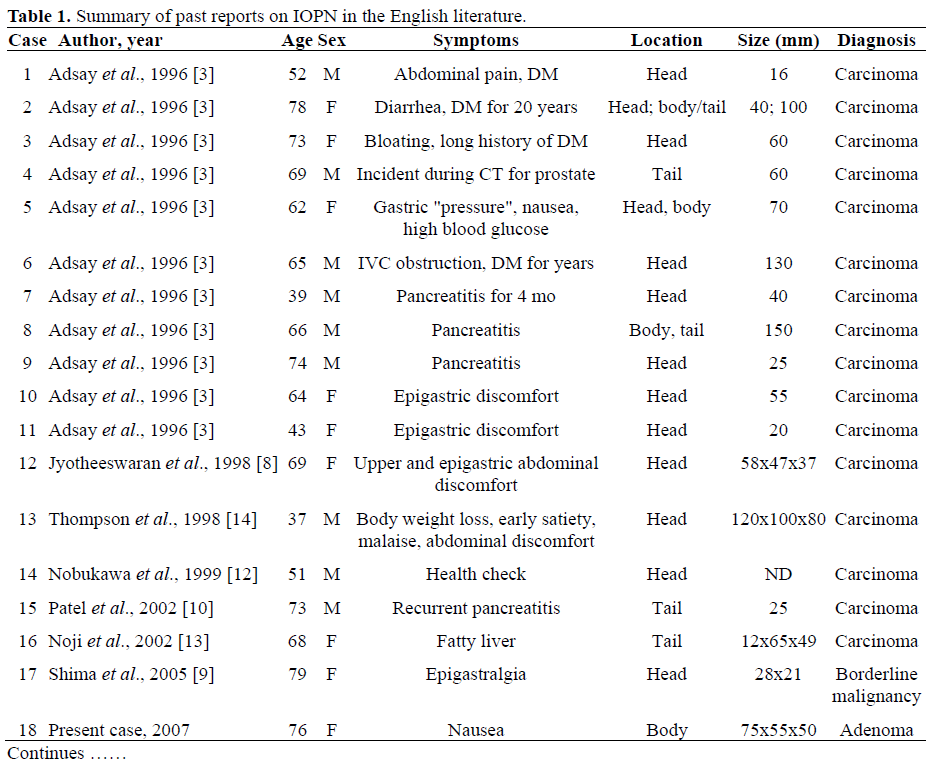
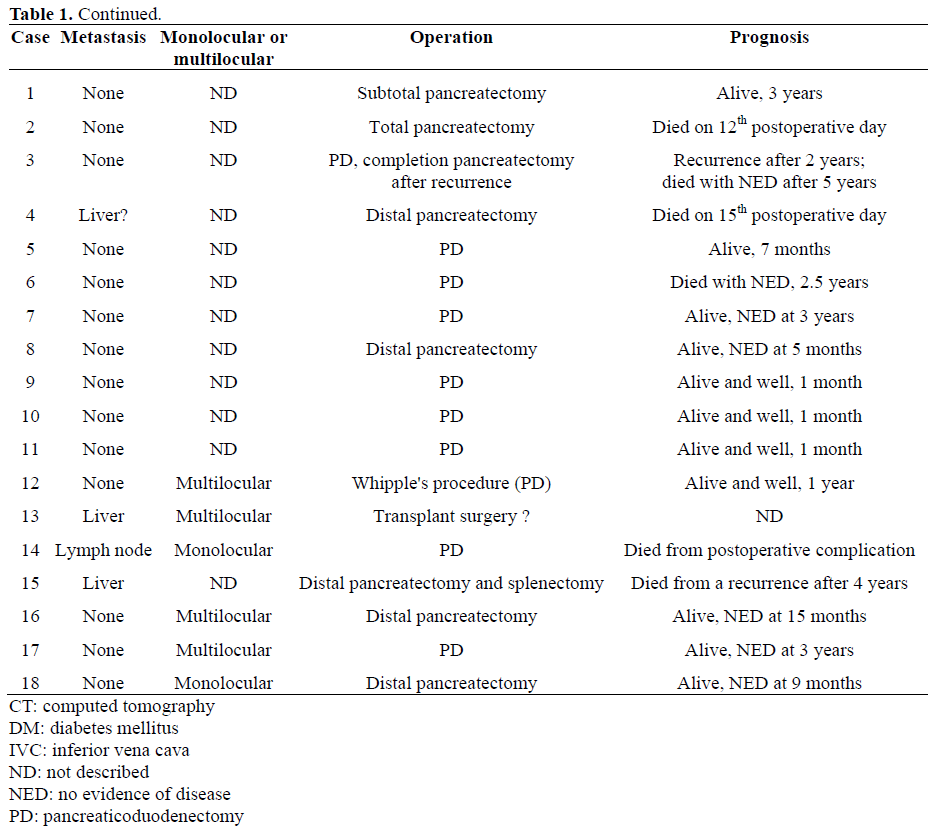
The 17 cases of IOPN which have been reported are summarized in Table 1 [3, 8, 9, 10, 11, 12, 13, 14]. The average age of the patients was 62.5 years, and the male-to-female ratio was 9:8. In cases in which the chief complaint was known, epigastralgia and discomfort were most common while diabetes mellitus and pancreatitis were frequent as coexisting symptoms. As in cases of IPMN, most tumors (72.2%) were located in the pancreatic head while a few were found in the body or tail. Tumor size was relatively large, with an average diameter of 62.5 mm.
Because reports of IOPN are found primarily in pathology journals, detailed analyses of image studies such as ERP and EUS have not been carried out. Only four case reports clearly mention the use of ERP to analyze communication as it relates to the main pancreatic duct [8, 9, 10, 13]. Adsay et al. [3] reported that mucin production in IOPNs was less than in IPMNs. To date, reports of dilatation of the MPD or mucin excretion from the duodenal papilla are limited [8, 9]. In our particular case, no communication between the mass and the MPD was found in ERCP or pathological findings, and neither dilatation of the MPD nor excretion of mucin from the papilla could be detected. In addition, the cystic contents with hemorrhage in the present case are often observed in MCNs but not IPMNs [15, 16]. Therefore, in our case, the IOPN shared clinical characteristics with the MCN as to location, internal hemorrhaging and no communication with the MPD unlike past reports.
Ninety-four percent of cases were diagnosed as carcinoma including reports of invasive tumors or distant metastasis. Therefore, the case presented here is a rare example of a benign IOPN. An adenoma-carcinoma sequence has been proposed for IPMN, and the issue of malignant potential is under intense investigation [17]. In contrast, the degree of malignant potential for IOPNs is still unclear due to the scarce number of reports. As oncocytic tumors tend to be benign in other organs, it is thought that the presence of oncocytes is not the main deciding factor in determining the malignant potential of a tumor [2]. Because all the reported cases of IOPNs were surgical cases, the average size and malignancy in these cases may be biased toward larger size and higher malignancy. Because only one case involved death due to an IOPN, good prognoses can be expected. However, it may be necessary to consider the suitability of follow-up periods which up to now have been short.
In conclusion, the present case had different characteristics from the IOPNs of past reports. The clinical significance of an IOPN is unclear due to the scarce numbers of reports but warrants further examination.
References
- Jaffe RH. Adenolymphoma (oncocytoma) of parotid gland.Am J Cancer 1932; 16:1415-23.
- Tallini G. Oncocytictumours. Virchows Arch 1998; 433:5-12. [PMID 9692819]
- Adsay NV, Adair CF, Heffess CS, Klimstra DS. Intraductaloncocytic papillary neoplasms of the pancreas.Am J SurgPathol 1996; 20:980-94. [PMID 8712298]
- Gotchall J, Traweek ST, Stenzel P. Benign oncocytic endocrine tumor of the pancreas in a patient with polyarteritisnodosa. Hum Pathol 1987; 18:967-9. [PMID 2887505]
- Lee WY, Tzeng CC, Jin YT, Chow NH, Yip CM, Lee JC. Papillary cystic tumor of the pancreas: a case indistinguishable from oncocytic carcinoma. Pancreas 1993; 8:127-32. [PMID 8419900]
- Frexinos J, Ribet A. Oncocytes in human chronicpancreatitis. Digestion 1972; 7:294-301. [PMID 4671520]
- Welter C, Kovacs G, Seitz G, Blin N. Alteration of mitochondrial DNA in human oncocytomas. Genes Chromosomes Cancer 1989; 1:79-82. [PMID 2487148]
- JyotheeswaranS, Zotalis G, Penmetsa P, LeveaCM, SchoenigerLO, Shah AN. A newly recognized entity: intraductal "oncocytic" papillary neoplasm of the pancreas. Am J Gastroenterol 1998; 93:2539-43.[PMID 9860422]
- Shima Y, Yagi T, Inagaki M, Sadamori H, Tanaka N, Horimi T, et al. Intraductaloncocytic papillary neoplasm of the pancreas with celiac artery compression syndrome and a jejunal artery aneurysm: report of a case. Surg Today 2005; 35:86-90. [PMID 15622472]
- Patel SA, Adams R, Goldstein M, Moskaluk CA. Genetic analysis of invasive carcinoma arising in intraductaloncocytic papillary neoplasm of the pancreas. Am J SurgPathol 2002; 26:1071-7. [PMID 12170096]
- Terris B, Dubois S, Buisine MP, Sauvanet A, RuszniewskiP, Aubert JP, et al. Mucin gene expression in intraductal papillary-mucinous pancreatic tumours and related lesions. J Pathol 2002; 197:632-7. [PMID 12210083]
- NobukawaB, Suda K, Suyama M, Ariyama J, Beppu T, Futagawa S. Intraductaloncocytic papillary carcinoma with invasion arising from the accessory pancreatic duct. GastrointestEndosc 1999; 50:864-6.[PMID 10570358]
- Noji T, Kondo S, Hirano S, Ambo Y, Tanaka E, Katoh C, et al. Intraductaloncocytic papillary neoplasm of the pancreas shows strong positivity on FDG-PET. Int J Gastrointest Cancer 2002; 32:43-6. [PMID 12630769]
- Thompson K, Castelli MJ, Gattuso P. Metastatic papillary oncocytic carcinoma of the pancreas to the liver diagnosed by fine-needle aspiration. DiagnCytopathol 1998; 18:291-6. [PMID 9557266]
- Zamboni G, Scarpa A, Bogina G, Iacono C, BassiC, Talamini G, et al. Mucinous cystic tumors of the pancreas: clinicopathological features, prognosis, and relationship to other mucinous cystic tumors. Am J SurgPathol 1999; 23:410-22. [PMID 10199470]
- Thompson LD, Becker RC, Przygodzki RM, Adair CF, Heffess CS. Mucinous cystic neoplasm (mucinous cystadenocarcinoma of low-grade malignant potential) of the pancreas: a clinicopathologic study of 130 cases. Am J SurgPathol 1999; 23:1-16. [PMID 9888699]
- Adsay NV, Merati K, Basturk O, Iacobuzio-Donahue C, Levi E, Cheng JD, et al. Pathologically and biologically distinct types of epithelium inintraductal papillary mucinous neoplasms: delineation of an "intestinal" pathway of carcinogenesis in the pancreas. Am J SurgPathol 2004;28:839-48. [PMID 15223952]








