Keywords
Ampulla of Vater; Biliary Tract Neoplasms; Pancreatectomy; Radiology, Interventional
INTRODUCTION
Pancreatic resections have historically been associated with significant postoperative mortality and morbidity. Over time, postoperative mortality has decreased in most high volume centres, ranging from 2 to 5%, while the incidence of postoperative complications remains high, ranging from 30 to 50% [1-9]. Of these complications, postoperative pancreatic fistula, bile leak and postpancreatectomy haemorrhage represent life-threatening complications because they require a relaparotomy in 4 to 20% of cases, [10] and postoperative mortality following relaparotomy is extremely high, ranging from 13 to 60% [10]. Advances in radiological techniques have increased the use of interventional radiology (IR) in specialist centres for the initial first-line management of these serious postoperative complications, thus reducing the need for reoperation [11- 14]. This study reports our experience with IR procedures after pancreatic resection for pancreatic and periampullary diseases with the purpose of evaluating their usefulness.
METHODS
This was a retrospective study involving a prospective data base regarding all patients who underwent pancreatic resections for pancreatic and periampullary diseases from January 2004 to December 2012. Only patients with postoperative complications were included. Written informed consent was obtained from each patient. All patients with complications were analysed separately regarding the use of IR procedures, including percutaneous drainage of intra-abdominal fluid collections, percutaneous transhepatic cholangiography with percutaneous transhepatic biliary drainage (PTC/PTBD), and angiography with arterial intervention, embolisation or stenting. Patients were selected to perform IR in relation to the clinical course and to the results of an abdominal CT scan. The technical and clinical success of the IR procedures as well as reoperation and repetition of the procedure after IR were reported. Patients with complications in whom IR was performed were compared with patients in whom IR was not performed regarding type of pancreatic resection (pancreaticoduodenectomy, total pancreatectomy, distal pancreatectomy etc.), diagnosis (chronic pancreatitis and pancreatic cancer vs. other periampullary diseases), postoperative mortality and morbidity according to the Clavien-Dindo classification [15], postoperative pancreatic fistula (POPF), postpancreatectomy haemorrhage (PPH), bile leak (BL), reoperation rate and length of hospital stay (LOS). The principal aims of our study were to evaluate the indications, safety and usefulness of IR procedures in the treatment of complications after pancreatic resection for pancreatic and periampullary diseases.
Postoperative mortality was defined as the number of deaths occurring for any reason within 30 days after surgery or before discharge. The postoperative morbidity rate included all complications following surgery up to the day of discharge; they were classified according to the Clavien- Dindo classification [15]. A postoperative pancreatic fistula was defined as the drainage of any measurable volume of fluid with an amylase content greater than 3 times the serum amylase activity on or after postoperative day 3, according to the criteria of the International Study Group on Pancreatic Fistula [8]. Post-pancreatectomy haemorrhage was defined using the International Study Group of Pancreatic Surgery criteria [16]. Bile leak was defined by the International Study Group of Liver Surgery as fluid with an increased bilirubin concentration in the drain or intra-abdominal fluid at least 3 times greater than the serum bilirubin concentration measured at the same time [17].
Immediate technical success was defined as successful aspiration or drain placement at the time of procedure; clinical success was defined as occurring when IR determined the resolution of the complications without other non-radiological treatment or relaparotomy [11]. Periampullary diseases included ampullary, duodenal, cystic and islet cell tumours.
Surgical Techniques and Postoperative Course
The pancreaticoduodenectomies (PDs) and total pancreatectomies (TPs) were performed using the Whipple procedure. In the PDs, the pancreatic remnant was always monitored with a pancreaticojejunostomy without stenting. The biliary tract was treated with a hepaticojejunostomy with stenting if the bile duct was small in diameter in both the PDs and the TPs. Drains were placed in all patients; the first was placed close to the bilio-enteric anastomosis (PD and TP) and the second close to the pancreaticoenteric anastomosis (PD). The left pancreatectomies (LPs) were performed either open or laparoscopically, and the pancreatic remnant was always managed with a stapler. A single drain was placed in all patients close to the pancreatic remnant. The procedures were performed by two experienced surgeons who had each done more than 50 pancreatic resections. Postoperatively, the amylase fluid and quantitative drain output were measured every day from postoperative day 3 to day 10 from the drain placed close to the pancreatic remnant (LP) or the pancreaticojejunostomy (PD). The drain was removed on postoperative day 4 if the amylase value in the drainage fluid was normal. An abdominal CT scan was performed only when an intraabdominal complication was suspected. In all patients who underwent PD, somatostatin analogues were administered postoperatively from postoperative days 1-7, except in the presence of a pancreatic leak in which case they were continued. In both the PDs and the TPs, the drains placed near a hepaticojejunostomy were removed on postoperative day 4 if there was no persistent bilious fluid. A diagnosis of PPH was based on clinical aspects and haemoglobin concentration; if the haemoglobin level dropped to ≥ 3 g/dl, an angio-CT scan or angiography was performed. In the presence of persistent POPF, sentinel bleeding (haemoglobin level dropped to 2 g/dl) was sufficient to indicate an angio-CT scan.
STATISTICS
Means, standard deviation and frequency were used to describe the data. Univariate analyses were carried out using the Fisher’s exact test, the Mann-Whitney-U test and the Pearson chi square linear by linear association. All statistical analyses were carried out by running SPSS for Windows (version 13.0) on a personal computer. Twotailed P values less than 0.05 were considered statistically significant.
RESULTS
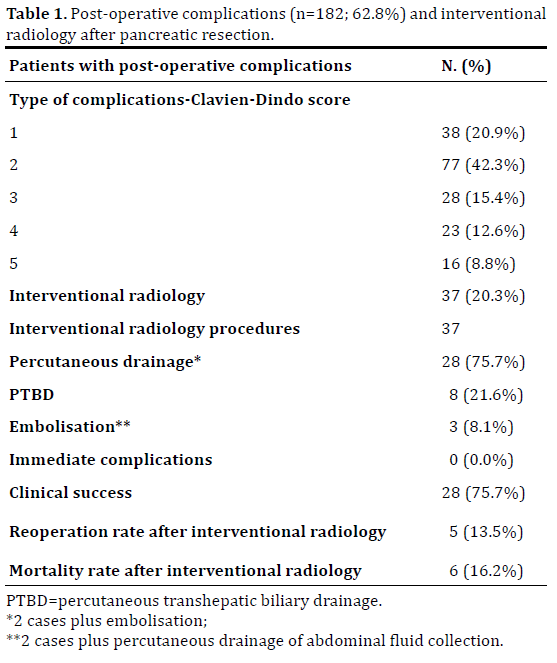
Two hundred and ninety patients underwent pancreatic resections for pancreatic and periampullary diseases from January 2004 to December 2012. Their demographic, surgical, pathologic diagnosis and outcome data are summarised in Table 1. One hundred and eighty-two (62.8%) patients experienced postoperative complications but only 67 (36.8%) had a major complications (grades 3-4- 5). The postoperative mortality rate (grade 5) was 5.5% (16 patients). The overall reoperation rate was 9.0% (26 patients out of 290). The mean length of hospital stay was 18.3 ± 14.4 days. Interventional radiology procedures were performed in 37 out of 290 cases (12.8%). If we consider only the 182 complicated patients, the rate of IR, as part of the treatment, increased from 12.8 to 20.3%. The IR procedure most frequently performed was percutaneous drainage of the intra-abdominal fluid collection (28 cases,75.7%, 2 cases were associated with endoscopic procedures and 2 cases involved percutaneous drainage plus embolisation), followed by percutaneous transhepatic biliary drainage (8 cases,21.6%), and embolisation of the common hepatic artery (3 cases, 8.1%, 2 cases which involved embolisation plus percutaneous drainage of the intra-abdominal fluid collection). Computed tomographyguided percutaneous drainage of the intra-abdominal fluid collection was usually performed (25 cases, 89.3%); ultrasound-guided percutaneous drainage (3 cases, 10.7%) was rarely performed. The IR procedures were performed 14 ± 6.7 days after surgery, and were performed successfully and without immediate complications in all cases. In 13 (35.1%) cases, the procedures were repeated and the number of procedures for each patient ranged from 1 to 3. Clinical success was obtained in 75.7% of cases. The reoperation rate after IR procedures was 13.5% (5 cases); therefore, reoperation was avoided in 32 (86.5%) cases. The mortality rate after IR procedures was 16.2% (6 cases); 4 of these 6 cases (66.7%) involved patients who first underwent IR and then a re-laparotomy (Table 1).
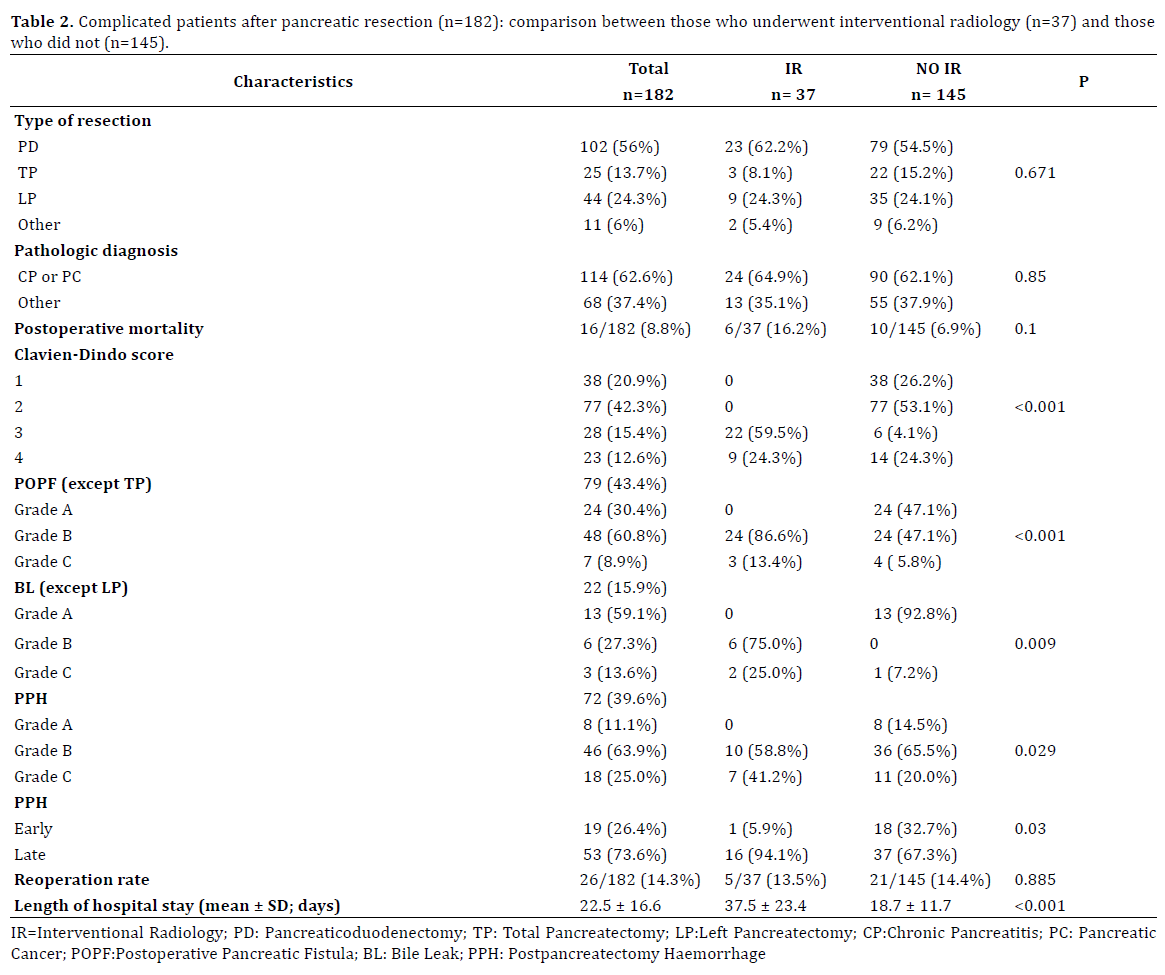
The comparison between the IR group and noninterventional group is summarised in Table 2. There were no statistically significant differences between the IR group and the non-interventional group regarding type of resection (P=0.671), pathologic diagnosis (P=0.850), postoperative mortality (16.2% vs. 6.9%; P=0.100) and reoperation rate (13.5% vs. 14.4%; P=0.885). Patients with clinically relevant POPF and bile leaks (BLs) (grade B and C) were treated significantly more frequently with IR than without it (P<0.001 and P=0.009, respectively). Patients with early PPH were treated more frequently without IR while patients with late PPH were treated with IR (P=0.030) as were patients with PPH grade C (P=0.029). Patients with grades 3, 4 and 5 of the Clavien- Dindo classification who had complications were treated significantly more frequently with interventional radiology procedures (P<0.001). Finally, patients treated with IR procedures had a statistically significant longer length of hospital stay than those in the non-interventional group (37.5 ± 23.4 vs. 18.7 ± 11.7 days; P<0.001).
DISCUSSION
The postoperative mortality rate after pancreatic resection has decreased over time in high volume centres while the postoperative complication rate has remained high [1-9]. The treatment of postoperative complications has changed over time in relation to the more frequent use of minimally invasive techniques. In 2003, Sohn et al. [13] first recognised the importance of IR procedures for the treatment of complications after a pancreaticoduodenectomy and reported the procedures most frequently performed (percutaneous drainage of intra-abdominal fluid collections, percutaneous transhepatic biliary drainage and embolisation) and their indications (pancreatic fistula formation, intra-abdominal abscesses and bile leak). Subsequently, other authors reported the use of IR procedures in the treatment of complications after pancreatic resection ranging from 5.2 to 42.2%, and confirmed the indications and the types of interventional procedures previously reported by Sohn [11-13, 19-21]. Percutaneous drainage of intra-abdominal fluid collections had very high technical and clinical success rates ranging from 93.5 to 100% and from 72 to 83.9%, respectively [11, 13, 18]. Endovascular interventions were also considered safe and feasible, even if they presented a complication rate ranging from 14 to 36% [21-23]. Nevertheless, Limongelli et al [22] reported a significant major complication rate if PPH was treated with surgery as opposed to endovascular procedures (36% vs. 70%; P=0.05) and, in the meta-analysis conducted by Roulin et al. [24] there was a statistically significant difference (47% vs. 22%; P=0.02) in favour of interventional radiology in terms of mortality after PPH. However, it should be pointed out that these studies had small samples as well as some biases, including a selection bias (stabilised patients/ angiography, hemodynamically unstable patients/ laparotomy). The clinical success of the endovascular interventions ranged from 63 to 100% [21-23] and Limongelli et al. [22] reported that complete hemostasis was possible in 73% of all endovascular procedures.
In our experience, interventional radiology procedures were performed in approximately one out of five complicated patients. They were always performed in patients with major complications (grades 3, 4 and 5 of the Clavien-Dindo classification). It was pointed out that IR was performed in more than fifty per cent of patients with major complications (37 out of 67 cases=55.2%). The main indications for IR were intra-abdominal fluid collection due to POPF grades B and C (27 cases out of 37 procedures; 73.0%), followed by bile leak grades B and C (8 cases=21.6%) and, finally, PPH grades B and C (3 cases=8.1%). The most frequently performed IR procedure was percutaneous CT-guided drainage of intra-abdominal fluid collections (27 due to POPF grades B or C, and 1 due to a bile leak). The prompt recognition and treatment of pancreatic leakage and intra-abdominal fluid collection is essential in resolving this most important and frequent complication after pancreatic resection. Moreover, it is useful for preventing and treating life-threatening complications as well as late post-pancreatectomy haemorrhage. For this reason, endovascular surgery for the treatment of late PPH has rarely been performed. In fact, it can be seen that IR procedures were performed in 17 patients with PPH B or C while embolisation was performed in only 3 patients. In our experience, percutaneous drainage of POPF grades B or C was useful in treating both POPF and PPH in 14 patients.
Interventional radiology procedures were always performed with technical success and without early complications, and clinical success was achieved in two out of three patients. Thus, IR after pancreatic resection was feasible and safe.
Finally, to our knowledge, only two papers have compared complicated patients treated with IR and patients in whom IR was not performed. Sohn et al. [13] comparing patients treated with IR and those (complicated and noncomplicated) in whom IR was not performed, showed that patients undergoing IR had a significantly greater incidence of postoperative mortality (6.2% vs. 1.7%: P<0.01), reoperation rate (15% vs. 2.5%; P=<0.01) and a longer median length of stay (15 vs. 10 days). Instead, Baker et al. [12] comparing only complicated patients treated or not with IR, noted that there was no statistical difference in perioperative mortality (P=0304), reoperation rate (P=0.245) and length of hospital stay (P=0.76). The present study represents the second study in which complicated patients treated with IR and complicated patients treated without IR were compared. Similarly to Baker et al. [12] it showed that there was not a significant increase in postoperative mortality and reoperation rate between the two groups, even if IR procedures significantly increased the length of hospital stay. Moreover, our study showed that IR procedures were performed more frequently in those patients with a BL, a high grade of POPF or PPH, and complication grades of 3 or 4 according to the Clavien-Dindo classification. Considering these results, we can hypothesise that IR procedures were very useful in avoiding reoperation.
In conclusion, our results suggested that IR procedures after pancreatic resection for pancreatic and periampullary diseases were feasible, safe and useful, especially for patients with postoperative pancreatic fistulas and bile leaks in whom reoperation was very often avoided.
They consisted, for the most part, of percutaneous CTguided drainage of an intra-abdominal fluid collection due to POPF. They provided less invasive treatment of the complication preventing other life-threatening complications and avoiding reoperation, with the associated morbidity and mortality in an elevated percentages of cases. Therefore, IR procedures were useful in decreasing postoperative mortality after pancreatic resections.
This illustrates the importance of considering an interventional abdominal imaging team in the postoperative management of these patients an integral component of specialist centres for pancreatic surgery.
Conflict of Interest
The authors declare that they have no conflict of interest.
References
- Schmidt CM, Powell ES, Yiannoutsos CT, Howard TJ, Wiebke EA, Wiesenauer CA, Baumgardner JA, et al. Pancreaticoduodenectomy: a 20- year experience in 516 patients. Arch Surg. 2004; 139:718-25. [PMID: 15249403]
- Bassi C, Falconi M, Salvia R, Mascetta G, Molinari E, Pederzoli P. Management of complications after pancreaticoduodenectomy in a high volume centre: results on 150 consecutive patients. Dig Surg. 2001; 18:453-7. [PMID: 11799295]
- Callery MP, Pratt WB, and Vollmer CM. Prevention and management of pancreatic fistula. J Gastrointest Surg. 2009; 13:163–173. [PMID: 18496727]
- Yang YM, Tian XD, Zhuang Y, Wang WM, Wan YL, Huang YT. Risk factors of pancreatic leakage after pancreaticoduodenectomy. World J Gastroenterol. 2005; 11(16):2456-61. [PMID: 15832417]
- Shrikhande SV and D’Souza MA. Pancreatic fistula after pancreatectomy: evolving definitions, preventive strategies and modern management. World J Gastroenterol. 2008; 14:5789–5796. [PMID: 18855976]
- Lai EC, Lau SHY, and Lau WY. Measures to prevent pancreatic fistula after pancreatoduodenectomy: a comprehensive review. Arch Surg. 2009; 144:1074–1080. [PMID: 19917946]
- Cameron JL, Riall TS, Coleman J, Belcher KA. One thousand consecutive pancreaticoduodenectomies. Ann Surg. 2006; 244:10-5. [PMID: 16794383]
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, Neoptolemos J, et al. Post-operative pancreatic fistula: an international study group (ISGPF) definition. Surgery. 2005; 138:8-13. [PMID: 16003309]
- Gooiker GA, van Gijn W, Wouters MW, Post PN, van de Velde CJ, Tollenaar RA. Systematic review and meta-analysis of the volumeoutcome relationship in pancreatic surgery. Br J Surg. 2011; 98:485-494. [PMID: 21500187]
- Standop J, Glowka T, Schmitz V, Schäfer N, Overhaus M, Hirner A, Kalff JC. Operative re-intervention following pancreatic head resection: indications and outcome. J Gastrointest Surg. 2009; 13:1503-1509. [PMID: 19421823]
- Zink SI, Soloff EV, White RR, Clary BM, Tyler DS, Pappas TN, Paulson EK. Pancreaticoduodenectomy: frequency and outcome of post-operative imaging-guided percutaneous drainage. Abdom Imaging. 2009; 34:767- 771. [PMID: 18758847]
- Baker TA, Aaron JM, Borge M, Pierce K, Shoup M, Aranha GV. Role of interventional radiology in the management of complications after pancreaticoduodenectomy. Am J Surg. 2008; 195:386-390. [PMID: 18308043]
- Sohn TA, Yeo CJ, Cameron JL, Geschwind JF, Mitchell SE, Venbrux AC, Lillemoe KD. Pancreaticoduodenectomy: Role of Interventional Radiologists in Managing Patients and Complications. J Gastrointest Surg. 2003; 7:209-219. [PMID: 12600445]
- Sanjay P, Kellner M and Tait IS. The role of interventional radiology in the management of surgical complications after pancreatoduodenectomy. HPB. 2012; 14:812-817. [PMID: 23134182]
- Dindo D, Demartines N, Clavien PA. Classification of surgical complications. A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004; 240:205-213. [PMID: 15273542]
- Wente MN, Veit JA, Bassi C, Dervenis C, Fingerhut A, Gouma DJ, et al. Postpancreatectomy haemorrhage (PPH)-An International Study Group of Pancreatic Surgery (ISGPS) definition. Surgery. 2007; 142:20-25. [PMID: 17629996]
- Koch M, Garden OJ, Padbury R, Rahbari NN, Adam R, Capussotti L, et al. Bile leakage after hepatobiliary and pancreatic surgery: A definition and grading of severity by the International Study Group of Liver Surgery. Surgery. 2011; 149:680-688. [PMID: 21316725]
- Pedrazzoli S, Liessi G, Pasquali C, Ragazzi R, Berselli M, Sperti C. Postoperative pancreatic fistulas. Preventing severe complications and reducing reoperation and mortality rate. Ann Surg. 2009; 249:97-104. [PMID: 19106683]
- Correa-Gallego C, Brennan MF, D'angelica M, Fong Y, Dematteo RP, Kingham TP, Jarnagin WR, et al. Operative drainage following pancreatic resection. Analysis of 1122 patients resected over 5 years at a single institution. Ann Surg. 2013; 258:1051-1058. [PMID: 23360918]
- Azeem N, Baron TH, Topazian MD, Zhong N, Fleming CJ, Kendrick ML. Outcomes of endoscopic and percutaneous drainage of pancreatic fluid collections arising after pancreatic tail resection. J Am Coll Surg. 2012; 215:177-185. [PMID: 22634120]
- Asai K, Watanabe M, Kusachi S, Matsukiyo H, Saito T, Kodama H, Enomoto T, et al. Successful treatment of a common hepatic artery pseudoaneurysm using a coronary covered stent following pancreatoduodenectomy: report of a case. Surg Today. 2014; 44:160-165. [PMID: 22932840]
- Limongelli P, Khorsandi SE, Pai M, Jackson JE, Tait P, Tierris J, Habib NA, et al. Management of delayed postoperative haemorrhage after pancreaticoduodenectomy. Arch Surg. 2008; 143:1001-1007. [PMID: 18936380]
- Roulin D, Cerantola Y, Demartines N, Schäfer M. Systematic review of delayed Postoperative haemorrhage after pancreatic resection. J Gastrointest Surg. 2011; 15:1055-1062. [PMID: 21267670]

