Yoshihiro Hamada1*, Kensei Maeshiro2 and Yoshifuku Nakayama3
1Department of Pathology, School of Medicine, Fukuoka University, Fukuoka, Japan
2Department of Surgery, St. Maria Hospital, Kurume, Fukuoka, Japan
3Laboratory Medicine, Kyushu Medical Center, Fukuoka, Japan
- *Corresponding Author:
- Yoshihiro Hamada
Department of Pathology
School of Medicine, Fukuoka University
7-45-1, Nanakuma, Jonan-ku
Fukuoka, Japan
Tel +81-92-801-1011
Fax +81-92-863-8383
E-mail yhamada@fukuoka-u.ac.jp
Received June 10th, 2014 – Accepted September 04th, 2014
Keywords
Carcinoma, Pancreatic Ductal; pancreatic cancer-associated antigen MUSE11; Pancreatic Carcinoma; Pancreatic Neoplasms
INTRODUCTION
Surviving for 5 years is a milestone in cancer therapy, including in patients with pancreatic ductal adenocarcinoma (PDAC). Patients with PDAC have a poor prognosis because of local spread or metastatic disease at presentation and the associated low-rate of resectability [1, 2]. Three-dimensional analysis has shown an association between poor patient prognosis and the presence of microscopic residual cancer following resection (R1) [3, 4]. However, the impact of resection on outcome is unclear, with some reports finding that R1 resection has independent prognostic significance [3, 5-9], whereas other reports found that R1 resection was not prognostic [10-12]. Moreover, several patients who have undergone R1 resection have achieved long-term survival [13-16]. To clarify the prognostic significance of R1 resection of PDAC, we followed patients who underwent R1 resection for as long as possible and evaluated their cause of death. Thus, this study was designed to clarify the prognostic influence of R1 and R0 resection of PDAC on ≥5-year survival.
METHODS
A total of two seventy one patients underwent pancreatic resection in our hospital during a 26-year period. Of these, 33 survived ≥5 years; causes of death were known for those who died after 5 years. Patients with intraductal papillary mucinous neoplasms were excluded. Clinical data were obtained from patients’ charts, and pathological factors were assessed according to the first English edition of the classification of pancreatic cancer by the Japan Pancreas Society [17].
Surgical specimens were fixed in 10% buffered formalin for 24–48 hours and cut axially into slices 3–4 mm thick. All slices were evaluated macroscopically and microscopically. The degree of residual cancer in each sample was reassessed according to the criteria of the Royal College of Pathologists . R0 resection was defined as the complete absence of tumor tissue from the resection margins, and R1 resection was defined as the presence of tumor tissue ≤1 mm from a circumferential margin surface, including the pancreatic cut edges, the dissected peripancreatic margin including the dorsal area of the pancreas and SMV groove, and the ventral surface. In addition, the correlation between the number of cancer-positive slices at initial R1 resection and the time of tumor recurrence (<5 years vs. ≥5 years) was analyzed in 30 patients who underwent R1 resection and died due to peritonitis carcinomatosis following local recurrence.
Patients were followed-up for 61 to 288 months. Followup included outpatient reviews, physical examination, laboratory studies, and imaging methods, including abdominal ultrasonography and CT whenever symptoms and/or laboratory data were suggestive of local recurrence or metastatic disease. Causes of death were assessed by CT scans, with an autopsy performed on one patient.
Categorical variables were compared using the χ2 test and Spearman rank correlation. The principal outcome measure was length of survival, measured from the time of the original surgery and analyzed using the Kaplan– Meier method. Patients alive at the time of follow-up were censored. Variables significant (P<0.05) on univariate analysis were included in multivariate analysis in a backwards stepwise fashion. All statistical analyses were performed using StatView.
RESULTS
Of the thirty three patients who survived ≥5 years, 19 had undergone R0 resection and 14 had undergone R1 resection (Table 1). The percentage of male patients was significantly higher in the R1 than in the R0 group. All tumors were classified as invasive ductal adenocarcinomas, with no between-group differences in tumor grade, lymphovascular permeation, or MIB-1 labeling index. However, final tumor stage was significantly earlier in the R0 than in the R1 group.
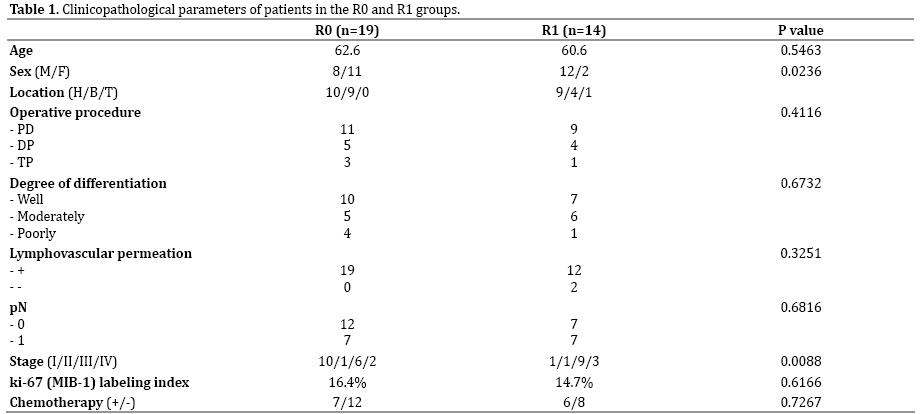
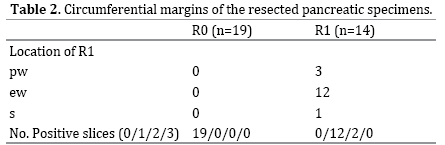
Three positive circumferential margins were observed in the resected specimens (Table 2): the pancreatic cut edge (pw), the dissected peripancreatic margin including the dorsal area of the pancreas and SMV groove (ew), and the ventral surface (s). The most common positive margin in the R1 group was ew. Of the 14 patients in this group, 12 had one involved margin and two had two involved margins.
The cumulative survival rates of the R0 and R1 groups after 5 years differed significantly (Figure 1). Median survival was 85 months in the R1 group and 96 months in the R0 group. Of the 14 patients who had undergone R1 resection, 12 died of peritoneal carcinomatosis following local recurrence. In contrast, only three patients died in the R0 group, two of senility and one of ischemic heart disease, but none died of PDAC recurrence. Interestingly, the time from surgery to death due to peritonitis carcinomatosis of R1 patients was inversely proportional to the number of cancer-positive slices (Figure 2, p<0.0032).
Figure 1. Kaplan–Meier survival curves of patients with PDAC who
underwent R0 or R1 resection and survived more than 5 years.
Figure 2. Correlation of number of positive slices and time to recurrence
in patients who underwent R1 resection and died within 5 years or
survived more than 5 years. The X-axis shows time (months) from surgical
resection of primary PDAC to death due to peritonitis carcinomatosis
following local recurrence. The Y-axis shows the number of positive
slices on detailed pathological examination of patients who underwent
R1 resection.
Multivariate analysis showed that R status was independently associated with long-term survival (Table 3).

DISCUSSION
The presence of positive surgical margins after resection of a solid tumor is a factor associated with poor patient prognosis. However, the impact of microscopically positive resection margins (R1) on outcome in patients with PDAC has been found to vary, with several studies reporting that it has independent prognostic significance [3, 5-9], while others have not [10-12]. Moreover, several patients who underwent R1 resection for PDAC survived for 5 years, confounding the impact of resection margin on patient prognosis [13-16]. Our results showed that R1 resection had an impact on the prognosis of patients who survived more than 5 years, and that these patients died because of peritoneal carcinomatosis following local tumor recurrence.
Several studies have described patient prognosis 5 years after surgery for PDAC. For example, five of 12 patients died of recurrent or metastatic pancreatic cancer more than 5 years after surgery [18], and 10 of 62 patients (16%) died of pancreatic cancer after 5 years [15]. One of 11 long-term survivors was found to experience a local recurrence 55 months after surgery and died 79 months postoperatively [19]. However, the mechanism underlying long-term recurrence is unclear. The pace of tumor progression may vary and may be determined by tumor biology rather than pathology, including by the number of tumor-initiating cells [20] and mesenchymal features [20-22]. We considered that late recurrence may also be associated with remnant tumor volume. About 90% of our patients who underwent R1 resection had only one positive slice. Moreover, we found that the time from surgery to recurrence was inversely proportional to the number of cancer-positive slices. Thus, remnant cancer volume might affect the time to recurrence. Detailed pathological examination may also help predict the time from surgery to recurrence.
Genomic study of pancreatic cancer cells taken from autopsies indicated that the time interval between the occurrence of the initiating mutation and the first parental, non-metastatic founder cell was 10 years, with at least 5 more years required for the acquisition of metastatic ability [23]. Our patients presented with tumor invasion or lymph node metastasis at surgical resection. However, the decreased tumor volume after surgical resection lengthened the time of tumor cell dissemination to >5 years. That is, metastasis required not only gene mutations, but also tumor volume or environment.
Although a detailed 3-dimensional analysis of pancreatic specimens can be performed [3, 4], our pathological assessments were performed using serial tissue slices 3–5 mm thick in a plane perpendicular to the duodenal axis. Despite the current lack of guidelines on the minimum number of blocks, the need for extensive sampling has been recognized [3, 24], with the number of circumferential resection margin blocks significantly correlating with R1 rate [3]. Because we sometimes detected small metastatic deposits in regional lymph nodes and in the soft tissues, we examined all slices. Moreover, because pathological diagnosis may have changed, so may have the final tumor stage. In addition, other lesions may have been present, such as endocrine microadenomas.
The significant difference in gender distribution in the R0 and R1 groups may have been due to gender-associated differences in visceral adipose tissue in Japanese individuals, with males generally having substantially more visceral adipose tissue than females [25]. This increase in adipose tissue volume in males may have increased the difficulty of dissection, especially on the dorsal side of the pancreas. Consequently, cancer cells may have been more likely to remain in the dissected area in males. Further investigations of additional patients should include assessments of differences in weight or amounts of visceral fat on imaging modalities.
In conclusion, there is a potential for tumor recurrence in the resected area of patients who undergo R1 resection of PDAC and survive for more than 5 years. Although the numbers of 5- and 10- year survivors with PDAC has increased, these patients should be followed-up as long as possible for the early diagnosis and treatment of recurrence.
Acknowledgments
The authors thank Ms. M. Yuhki for her excellent technical assistance.
Conflict of Interest
Authors declare to have no conflict of interest.
References
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, Thun MJ. Cancer statistics, 2008. CA Cancer J Clin. 2008; 58: 71-96. [PMID: 18287387]
- Sener SF, Fremgen A, Menck HR, Winchester DP. Pancreatic cancer: a report of treatment and survival trends for 100,313 patients diagnosed from 1985-1995, using the National Cancer Database. J Am Coll Surg. 1999; 189: 1-7. [PMID: 10401733]
- Verbeke CS, Leitch D, Menon KV, McMahon MJ, Guillou PJ, Anthoney A. Redefining the R1 resection in pancreatic cancer. 2006; Br J Surg 93: 1232-1237. [PMID: 16804874]
- Esposito I, Kleeff J, Bergmann F, Reiser C, Herpel E, Friess H, Schirmacher P, Büchler MW. Most pancreatic cancer resections are R1 resections. Ann Surg Oncol. 2008; 15: 1651-1660. [PMID: 18351300]
- Yeo CJ, Cameron JL, Lillemoe KD, Sitzmann JV, Hruban RH, Goodman SN, Dooley WC, Coleman J, et al. Pancreaticoduodenectomy for cancer of the head of the pancreas. 201 patients. Ann Surg. 1995; 221: 721-731. [PMID: 7794076]
- Sohn TA, Yeo CJ, Cameron JL, Koniaris L, Kaushal S, Abrams RA, Sauter PK, et al. Resected adenocarcinoma of the pancreas-616 patients: results, outcomes, and prognostic indicators. J Gastrointest Surg. 2000; 4: 567-579. [PMID: 11307091]
- Neoptolemos JP1, Stocken DD, Dunn JA, Almond J, Beger HG, Pederzoli P, Bassi C, et al. Influence of resection margins on survival for patients with pancreatic cancer treated by adjuvant chemoradiation and/ or chemotherapy in the ESPAC-1 randomized controlled trial. Ann Surg. 2001; 234: 758-768. [PNID: 11729382]
- Jarufe NP, Coldham C, Mayer AD, Mirza DF, Buckels JA, Bramhall SR. Favourable prognostic factors in a large UK experience of adenocarcinoma of the head of the pancreas and periampullary region. Dig Surg. 2004; 21: 202-209.
- Winter JM, Cameron JL, Campbell KA, Arnold MA, Chang DC, Coleman J, Hodgin MB, et al. 1423 pancreaticoduodenectomies for pancreatic cancer: A single-institution experience. J Gastrointest Surg. 2006; 10: 1199-1210. [PMID: 17114007]
- Bouvet M, Gamagami RA, Gilpin EA, Romeo O, Sasson A, Easter DW, Moossa AR. Factors influencing survival after resection for periampullary neoplasms. Am J Surg. 2000; 180: 13-17. [PMID: 11036132]
- Schmidt CM1, Powell ES, Yiannoutsos CT, Howard TJ, Wiebke EA, Wiesenauer CA, Baumgardner JA, et al. Pancreaticoduodenectomy: a 20- year experience in 516 patients. Arch Surg. 2004; 139: 718-725. [PMID: 15249403]
- Raut CP, Tseng JF, Sun CC, Wang H, Wolff RA, Crane CH, Hwang R, et al. Impact of resection status on pattern of failure and survival after pancreaticoduodenectomy for pancreatic adenocarcinoma. Ann Surg. 2007; 246: 52-60.[PMID: 17592291]
- Ferrone CR, Pieretti-Vanmarcke R, Bloom JP, Zheng H, Szymonifka J, Wargo JA, Thayer SP, et al. Pancreatic ductal adenocarcinoma: long-term survival does not equal cure. Surgery. 2012; 152: S43-49. [PMID: 22763261]
- Schnelldorfer T1, Ware AL, Sarr MG, Smyrk TC, Zhang L, Qin R, Gullerud RE, et al. Long-term survival after pancreatoduodenectomy for pancreatic adenocarcinoma: is cure possible? Ann Surg. 2008; 247: 456- 462. [PMID: 18376190]
- Riall TS, Cameron JL, Lillemoe KD, Winter JM, Campbell KA, Hruban RH, Chang D, Yeo CJ. Resected periampullary adenocarcinoma: 5-year survivors and their 6- to 10-year follow-up. Surgery. 2006; 140: 764-772. [PMID: 17084719]
- Cleary SP1, Gryfe R, Guindi M, Greig P, Smith L, Mackenzie R, Strasberg S, et al. Prognostic factors in resected pancreatic adenocarcinoma: analysis of actual 5-year survivors. J Am Coll Surg. 2004; 198: 722-731. [PMID: 15110805]
- Classification of Pancreatic carcinoma. Japan Pancreas Society Kanehara& Co. Ltd., Tokyo. 1996.
- Conlon KC, Klimstra DS, Brennan MF (1996) Long-term survival after curative resection for pancreatic ductal adenocarcinoma. Clinicopathologic analysis of 5-year survivors. Ann Surg 223: 273-279. [PMID: 8604907]
- Han SS, Jang JY, Kim SW, Kim WH, Lee KU, Park YH. Analysis of long-term survivors after surgical resection for pancreatic cancer. Pancreas. 2006; 32: 271-275. [PMID: 16628082]
- Rasheed ZA1, Yang J, Wang Q, Kowalski J, Freed I, Murter C, Hong SM, et al. Prognostic significance of tumorigenic cells with mesenchymal features in pancreatic adenocarcinoma. J Natl Cancer Inst. 2010; 102: 340-351. [PMID: 20164446]
- Javle MM, Gibbs JF, Iwata KK, Pak Y, Rutledge P, Yu J, Black JD, Tan D, Khoury T. Epithelial-mesenchymal transition (EMT) and activated extracellular signal-regulated kinase (p-Erk) in surgically resected pancreatic cancer. Ann Surg Oncolo. 2007; 14: 3527-3533. [PMID: 17879119]
- Krantz SB1, Shields MA, Dangi-Garimella S, Munshi HG, Bentrem DJ. Contribution of epithelial-to-mesenchymal transition and cancer stem cells to pancreatic cancer progression. J Surg Res. 2012; 173: 105-112. [PMID: 22099597]
- Yachida S1, Jones S, Bozic I, Antal T, Leary R, Fu B, Kamiyama M, et al. Distant metastasis occurs late during the genetic evolution of pancreatic cancer. Nature. 2010; 467: 1114-1117. [PMID: 20981102]
- Chatelain D1, Fléjou JF. [Pancreatectomy for adenocarcinoma: prognostic factors, recommendations for pathological reports]. Ann Pathol. 2002; 22: 422-431. [PMID: 12483163]
- Ishizuka J. Clinical significance of measurement of visceral fat area (in Japanese). Nippon RinshoNaikaikaishi 2006; 21: 420-425.



