Keywords
Meta-Analysis as Topic; Mortality; Multiple Organ Failure; Organ Dysfunction Scores; Pancreatitis, Acute Necrotizing /complications
Abbreviations
IPD: individual patient data; SOFA: Sepsisrelated Organ Failure Assessment
INTRODUCTION
Organ failure is a major determinant of mortality [1, 2, 3, 4, 5] in patients with acute pancreatitis and this has been highlighted in the new international multidisciplinary classification of acute pancreatitis severity as the “systemic” determinant [1, 2]. Patients who develop organ failure usually require admission to high dependency unit or intensive care unit (ICU). These patients are among the most resource demanding in health care systems [6, 7]. ICUs currently represent the largest clinical cost department in hospitals, with expenses estimated to be up to 20% of a hospital’s budget [8, 9], and costs per day is three to five-fold greater than in general wards [10, 11, 12].
Several aspects of organ failure have been studied, although many questions remain.
1) Dynamics of Organ Failure
It is widely accepted that local pancreatic inflammation is the initiating stimulus for a systemic inflammatory response. This, in turn, may result in the development of organ failure and contribute to death in patients with acute pancreatitis. The importance of the duration and reversibility of organ failure has been well recognized in the last decade. It has been shown that patients with worsening organ failure as well as those with persistent organ failure have a significantly higher mortality rate [13, 14, 15, 16, 17]. A study from the United Kingdom [14] enrolled 290 patients across 18 centers and found that resolution of organ failure within 48 hours was associated with a better prognosis compared to patients with organ failure for more than 48 hours. This was irrespective of whether the organ failure was present on admission or developed later. Another study conducted in Scotland [13] on 121 patients found that patients with worsening organ failure and poor response to treatment have a higher mortality rate. A study from New Zealand also demonstrated that the initial physiological response to intensive care treatment was a better predictor of outcome and mortality in patients with acute pancreatitis [17]. These studies underscore the dynamic nature of organ failure and the importance of monitoring the response to treatment.
2) Number of Failed Organs
The concept of multiple organ failure was first described in the 1970s [18], since then, a large number of definitions and acronyms have been proposed [19]. A modern definition for multiple organ failure in patients with acute pancreatitis refers to the failure of two or more organ systems [20]. Multiple organ failure has been shown to be the leading cause of death in a variety of clinical settings [21, 22]. Mortality rate in acute pancreatitis patients with multiple organ failure has been reported to be up to 100% [20, 23, 24, 25, 26] and there is a significant correlation between the number of organ failures and mortality [27]. A large population based retrospective cohort study on all deaths due to acute pancreatitis in Scotland included data from 1,024 patients and found that 63% of fatalities had failure of at least two organ systems [28].
3) Which Organs Fail
The Atlanta classification for severity of acute pancreatitis advocated four organ systems (cardiovascular, pulmonary, renal and gastrointestinal bleeding) to classify the severity of acute pancreatitis [22]. The European Society of Intensive Care Medicine since advocated a scoring system that includes six major organ systems to describe as quantitatively and objectively as possible the degree of organ dysfunction over time in critically ill patients [29]. This scoring system, termed the Sepsis-related Organ Failure Assessment (SOFA) score, has been widely used in a variety of disease settings [30, 31, 32]. The organ systems used in the SOFA score are respiratory, cardiovascular, coagulation, hepatic, renal and central nervous systems. The number of organ systems that have been included in studies have varied from three [4], four [27, 33], six [34, 35] to eight [27]. Based on the 2011 global survey of pancreatologists [36], the consensus is that three organ systems (respiratory, cardiovascular and renal) fail most frequently in patients with acute pancreatitis and is of much more prognostic importance than failure of other systems [4, 35, 37, 38]. Presence/absence of organ failure in each of these three systems is used in the new international multidisciplinary classification of acute pancreatitis severity [1].
4) Combination and Sequence of Organ Failures
A prospective multicenter inception cohort analysis [39] of 17,440 ICU admissions (all cases and not confined to patients with acute pancreatitis) treated from 1988 to 1990 and 5,677 ICU admissions treated from 1979 to 1982 found that combinations of organ systems and the organ system that failed had an impact on outcome. They found that the profile of physiologic abnormalities substantially influences mortality. For example, mortality rate for patients with two organ system failures varied from 20% (combination of hematologic and cardiovascular failure) to 76% (combination of cardiovascular and neurologic failures).
In patients with acute pancreatitis, a retrospective study by Halonen et al. [35] demonstrated that different combinations of two organ system failures have different mortality rates with the highest mortality rate (91%) associated with the combination of hepatic and renal failures. They also showed that hepatic failure, renal failure, previous cardiovascular medication and cardiovascular failure were independent factors that are associated with hospital mortality. Some limitations of this study include the retrospective design, the relatively small cohort of patients (n=113) and a selection bias because not all patients with organ failure were included.
Another study looked at sequential system failure in patients with acute renal failure after rupture of abdominal aortic aneurysms [40]. The authors showed that there was a similar progression of organ system failures in all patients. This sequence unfolded more slowly in patients that survived longer and developed more quickly in those surviving for shorter periods. This “predictability” of sequence failure in organ failure, if confirmed, may have important implications in the allocation of resource and targeted treatments directed towards slowing disease progression and reducing mortality.
Limitations of Current Knowledge About Organ Failure
First, most studies have been single center cohort studies [15, 16, 41, 42, 43, 44] without sufficient statistical power to investigate all aspects of organ failure and their effect on mortality. This is likely because of relatively low incidence of acute pancreatitis patients with organ failure. The annual incidence rate in the United States is 2-4 cases of complicated acute pancreatitis per year per 100,000 adults, and only a fraction of them develop organ failure [45].
Second, there are some studies in which the cohorts from larger multi-center studies are part of interventional studies [14, 46] which makes any inference about disease course and outcomes in general, and organ failure in particular, inherently biased. This is because any studied intervention is designed to alter the natural course of the disease. Other larger studies are limited by selection bias, such as using preselected cohorts of patients with other determinants of outcome (e.g., pancreatic necrosis) or only selected patients who had a contrast enhanced CT scan [33, 47, 48, 49]. This selection bias does not allow a valid inference about the course and outcomes of organ failure.
Third, there is a relatively limited body of evidence in the literature about the relative importance of different characteristics of organ failure such as number, timing, duration, sequence, and combination [1]. Moreover, there is limited evidence to validate the definitions of these characteristics. Valid outcome definitions are essential for quality research, allowing comparability of results among centers and the ability to monitor changes in between different centers over time [50].
Unanswered Questions About Organ Failure
Limitations and bias in the existing literature highlights the need for purportedly designed noninterventional studies to answer a number of key questions relating to the characteristics of organ failure in acute pancreatitis [51] and how they are linked to mortality (Figure 1). These include, but are not limited to the following questions:
1) What is the relative incidence of each organ failure?
2) What is the relationship between number of organ failures and mortality?
3) What is the most common sequence in failing systems?
4) What is the timing of onset for each organ failure and its effect on mortality?
5) How is mortality affected by the duration of each system failure?
6) What is the relative incidence of the specific sequences of organ failure and its effect on mortality?
7) What is the relative incidence of each combination of two system failures and its effect on mortality?
Figure 1. Current knowledge and unanswered questions
regarding patients with acute pancreatitis that develop organ
failure.s
Answering the Questions by Conducting an Individual Patient Data Meta-Analysis
Pooled analysis of prospective data from individual patients in all the available studies has been regarded as the gold standard in evidence synthesis generation [52, 53] and has provided the best approach to answer questions pertinent to the natural course of disease [54]. The methods and advantages of individual patient data (IPD) metaanalysis have been well described [55, 56]. IPD meta-analysis provides the least biased and most reliable means of addressing questions not satisfactorily answered by individual clinical studies [57]. This is because it does not rely on published information alone and includes all available study data, thus allowing for detailed checks of the integrity and completeness of data and also reducing selection and publication bias. By including data from multiple centers, it provides a stronger endorsement of results, better clarification and provision of updated follow up information, as well as a collaboration for further research [58]. In addition to this, it allows for more powerful and flexible analysis of subgroups and testing, adjusting for confounders.
OBJECTIVE
The aim of the proposed study is to perform an IPD meta-analysis to determine the relative incidence of each organ failure, and the impact that the number, timing, duration, sequence, and combination of different individual organ failures on mortality in patients with acute pancreatitis.
METHODS AND DESIGN
Study Design
The study design will be an individual patient data meta-analysis [55, 56, 57, 58].
Identification of Studies
All participants of the recently conducted first global survey of pancreatologists, who are active in clinical research, will be invited to contribute individual patient data to this study [36]. Table 1 presents the geographic distribution of participants in the global survey. Pancreatologists are also encouraged to contact the corresponding author of this article if they are interested in contributing to this project.

Eligibility Criteria
To be included, studies will have to meet the following criteria:
• Design: prospective cohort;
• Population: patients with acute pancreatitis who presented with or developed organ failure during first week of hospital admission;
• Exposure: respiratory, renal, and/or cardiovascular organ failure;
• Outcome: in-hospital mortality;
• Study period: conducted from the year 2000 onwards.
Studies/individual data will be excluded if:
• Participants were enrolled into an interventional study;
• Data do not contain the essential information required (see below).
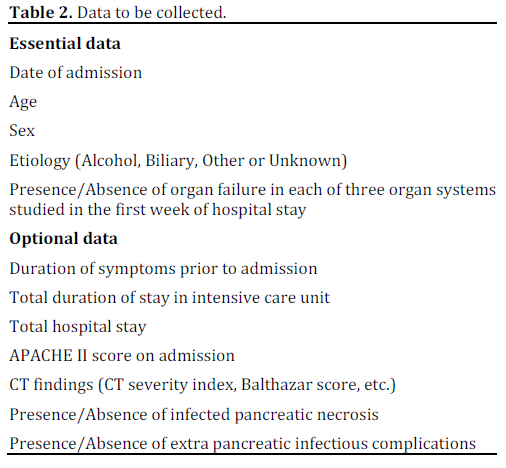
Collection of Data and Management
Essential and optional data to be collected are shown in Table 2. All the contributors will be asked to provide de-identified data by uploading them into a standardized data collection form or in any convenient format by encrypted, electronic transfer where possible or by other means as required, depending on site issues. The original data collection files sent by the authors will be kept in their original version and will be saved on a password-protected server at the University of Auckland, and behind the firewall to ensure security. Only the investigators of PANCREA II study will have direct access to individual data prior to publication of the final report.
Transfer of Data
The data will be transferred to a secure passwordprotected web server at University of Auckland or by privacy encrypted e-mail. This permits a secure and identifiable connection and minimizes the possibility of data loss.
Data Checking
Study investigators will perform data validation using a copy. The data will be checked independently with respect to range, internal consistency, missing or extreme values, errors and consistency with published reports. Study details, such as selection methods and outcome details will be crossed-checked against published reports, study protocols and data collection spread sheets. Apparent inconsistencies, implausibilities, or omissions will be clarified with collaborators and, where appropriate, rectified. Summary tables and listing of the variables used in planned analyses will be supplied to collaborators for checking. Any discrepancies will be resolved by discussion. Collaborators will be asked to verify all recorded data before any analysis and the data will not be used for any other purposes without permission from all the collaborators.
Core Data Set and Variables
All verified data will be entered into a master Excel spread sheet. A unique identification number will be allocated to each patient entered into the core data set. This number will easily correspond to patients from verified data from individual studies. The essential and optional data will be manually entered into master spread sheet, and checked.
Definitions
Acute pancreatitis will be diagnosed by the presence two of the following three features:
• abdominal pain characteristic of acute pancreatitis;
• serum amylase and/or lipase 3 times the upper limit of normal; and
• characteristic findings of acute pancreatitis on tomography (CT) scan.
Organ failure will be defined as the presence of worsened organ function in an acutely ill acute pancreatitis patient using one of the following criteria:
• “breaching of thresholds” as described by Bradley et al. [22] with shock defined as a systolic blood pressure less than 90 mmHg, pulmonary insufficiency defined as PaO2 of 60 mmHg or less, renal failure defined as a creatinine level greater than 177 μmol/L (2 mg/dL) after rehydration;
• a SOFA score of 2 or more for each individual system [29];
• a Marshall score of 2 or more for each individual system [59].
The organ systems that will be reported on include respiratory, cardiovascular and renal systems. The definitions used in relation to the timing, duration, sequence and combination of organ failures are given in Figure 2.
Figure 2. Outcome definitions for the studied characteristics of
organ failure.
Total hospital stay will be defined as the number of consecutive days the patient was in hospital.
Duration of symptoms will be defined as the number of consecutive full days (24 hours) the patient had symptoms before the day of admission, excluding the day of admission.
Planned Statistical Analysis
Due to the complexity of the statistical analyses, the following section represents the planned principal analyses; some modifications and secondary analyses are likely to emerge during the project. However, a detailed statistical analysis plan will be produced before the analysis. Any analysis conducted will be based on the checked and updated IPD from all available studies.
Primary Analysis
A “one-stage” approach will be used because of its increased power and ability to test for nonlinear relationships for continuous variables and ability to control for aggregation bias [53, 58, 60, 61, 62]. The model used will be based on a logistic regression model [52] adjusted for confounding variables including age, sex, etiology, etc. The dependent variable will be mortality and independent variables will initially include the characteristics of organ failure (timing, duration, sequence, and combination of organ failures). The R 2.15.2 framework (R Foundation for Statistical Computing, Vienna, Austria) will be used for statistical analysis [63].
Summary statistics with corresponding 95% confidence intervals (CIs) will be calculated. This will include the pooled incidence of each system failure. Patients will be grouped according to total number of organ failures at any point and pooled incidence for one, two, three organ failures will be calculated with corresponding mortality rates.
Patients will also be grouped according to timing of first (any) organ failure and mortality rates and relative risks will be calculated according to organ failure occurring at any particular day during the first week. Further analysis will be performed based on duration of organ failure. Relative risks of death will be calculated for patients with organ failure for one day only compared to organ failure for more than one day. The same analysis will be done for organ failure for two days compared to organ failure for more than two days and so on (three and four days).
Patients with two or three organ failures with different sequences of organ failures will be grouped together and the pooled incidence of each sequence of organ failure will be calculated.
Lastly, patients will be grouped according to different combinations of two organ failure and relative risks of death will be calculated. These combinations will include cardiovascular and respiratory, cardiovascular and renal, respiratory and renal systems.
Subgroup Analysis
The cohorts will be grouped according to the provision of optional data. These will be listed firstly in a summary table with the following headings: study title, number of patients, data available (yes/no) for covariates: durations of symptoms, APACHE II score on admission, extent of necrosis on CT, CT severity index, infectious pancreatic complications during hospitalization, other infectious complications during hospitalization, as well as data available for secondary outcomes: duration of ICU stay and total hospital stay. If sufficient patient numbers are available, analysis will then be conducted for each covariate in separate subgroups. The same model used in the primary analysis will also be applied for secondary outcomes if sufficient data are available.
Secondary Analysis
Further analyses may include possible confounding factors for the entire patient population identified from our subgroups analysis. Subsequent analysis from the primary analysis will adjust for any additional confounders using multivariate regression to give estimates that are more relevant to individual patients.
Data Presentation
Baseline characteristics of patients will be presented for individual cohorts as well as overall summary statistics. Continuous variables will be presented as mean and standard deviation (or median and range if not normally distributed). Binary and categorical outcomes will be presented as frequency and percentages. We will also report mortality rates both before and after adjustments for confounders.
For all primary and secondary analyses, adjusted risk ratios and corresponding 95% CIs will be presented, along with the corresponding P values. P values less than 0.05 will be regarded as statistically significant. The final meta-analysis will be reported based on relevant guidelines [64, 65].
Publication Policy
The main results of this project will be published and presented under the auspices of the Pancreatitis Across Nations Clinical Research and Education Alliance (PANCREA). Up to two researchers from each contributing centre and the PANCREA Steering Committee will be invited to author the manuscript. Results from further papers using the same data set will not be published without approval from all collaborators and will acknowledge the PANCREA collaboration as the source of the data. The PANCREA collaboration will disseminate the findings of its research widely at academic conferences and in journal publications.
DISCUSSION
Organ failure is one of main causes of death in patients with acute pancreatitis but, to date, there has been a lack of quality data on its natural course and characteristics that influence patients’ outcomes. Part of the drive to improve patients’ outcomes will require a better understanding of the different characteristics of organ failure. The best way to advance this is to aggregate existing prospective data from non-interventional studies under the auspice of an international collaboration. This approach allows for more powerful and flexible analysis of subgroups and testing, adjusting for confounders and minimizes publication and reporting bias [66] and has been described as the “gold standard” of evidence synthesis [55, 56, 57].
The PANCREA collaboration has already been established and its first study was to develop a new classification for the severity of acute pancreatitis [1]. This involved several stages. The first stage was an evidence review to recognize a need for a new classification for the severity of acute pancreatitis and to highlight the limitations of previous classifications. The second stage was conducting a world-wide survey of pancreatologists. The third stage was to further discuss the proposed classification and seek accord on definitions at an international symposium during the 2011 Meeting of the International Association of Pancreatology (Kochi, India). The final document was published as a feature article in the world’s premier surgical journal and was accompanied by a supportive editorial by the author of the Atlanta classification [67]. The new classification has also become available in several languages other than English [68, 69, 70, 71].
The study described in this protocol will be the second multicentre study of the PANCREA collaborative (PANCREA II study). It will attempt to answer important questions regarding the effect of timing, duration, sequence and combination of individual organ system failures on mortality. Information derived from this study will be used to optimize routine clinical management and improve clinical care strategies. These will then help in the direction of health resources and improve cost effectiveness. It can also help validate outcome definitions, allow comparability of results and form a more accurate basis for patient allocation in further clinical studies.
Conflict of interest
The authors have no potential conflict of interest
References
- Dellinger EP, Forsmark CE, Layer P, Lévy P, Maraví-Poma E, Petrov MS, et al. Determinant-based classification of acute pancreatitis severity: An international multidisciplinary consultation. Ann Surg 2012; 256:875-80. [PMID 22735715]
- Petrov MS, Windsor JA, Lévy P, Pancreatitis Across Nations Clinical Research and Education Alliance (PANCREA). New international classification of acute pancreatitis: more than just 4 categories of severity. Pancreas 2013; 42:389-91. [PMID 23486363]
- Stevenson K, Carter CR. Acute pancreatitis. Surgery 2013; 31:295-303.
- Thandassery RB, Yadav TD, Dutta U, Appasani S, Singh K, Kochhar R. Prospective validation of 4-category classification of acute pancreatitis severity. Pancreas 2013; 42:392-6. [PMID 23429498]
- Petrov MS, Windsor JA. Conceptual framework for classifying the severity of acute pancreatitis. Clin Res Hepatol Gastroenterol 2012; 36:341-4. [PMID 22551642]
- Sigurdsson GH. Intensive care management of acute pancreatitis. Dig Surg 1994; 11:231-41.
- Maraví Poma E, Zubia Olascoaga F, Petrov MS, Navarro Soto S, Laplaza Santos C, Morales Alava F, et al. SEMICYUC 2012. Recommendations for intensive care management of acute pancreatitis. Med Intensiva 2013; 37:163-79. [PMID 23541063]
- Halpern NA, Bettes L, Greenstein R. Federal and nationwide intensive care units and healthcare costs: 1986-1992. Crit Care Med 1994; 22:2001-7. [PMID 7988140]
- Chalfin DB. Cost-effectiveness analysis in health care. Hosp Cost Manag Account 1995; 7:1-8. [PMID 10143321]
- Oostenbrink JB, Buijs-Van der Woude T, van Agthoven M, Koopmanschap MA, Rutten FF. Unit costs of inpatient hospital days. Pharmacoeconomics 2003; 21:263-71. [PMID 12600221]
- van Dijk FE, van der Werken C. What are the costs of an intensive care patient? The direct costs of a surgical patient per ICU-admission and per inpatient day. Medisch Contact 1998; 53:1154-6.
- Carter D. Acute pancreatitis: the value of life. Br J Surg 1993; 80:1499-500. [PMID 8298910]
- Buter A, Imrie CW, Carter CR, Evans S, McKay CJ. Dynamic nature of early organ dysfunction determines outcome in acute pancreatitis. Br J Surg 2002; 89:298-302. [PMID 11872053]
- Johnson C, Abu-Hilal M. Persistent organ failure during the first week as a marker of fatal outcome in acute pancreatitis. Gut 2004; 53:1340-4. [PMID 15306596]
- Lytras D, Manes K, Triantopoulou C, Paraskeva C, Delis S, Avgerinos C, Dervenis C. Persistent early organ failure: defining the high-risk group of patients with severe acute pancreatitis? Pancreas 2008; 36:249-54. [PMID 18362837]
- Le Mée J, Paye F, Sauvanet A, O'Toole D, Hammel P, Marty J, et al. Incidence and reversibility of organ failure in the course of sterile or infected necrotizing pancreatitis. Arch Surg 2001; 136:1386-90. [PMID 11735865]
- Flint R, Windsor JA. Early physiological response to intensive care as a clinically relevant approach to predicting the outcome in severe acute pancreatitis. Arch Surg 2004; 139:438-43. [PMID 15078714]
- Eiseman B, Beart R, Norton L. Multiple organ failure. Surg Gynecol Obstet 1977; 144:323-6. [PMID 841449]
- Baue AE. MOF, MODS, and SIRS: what is in a name or an acronym? Shock 2006; 26:438-49. [PMID 17047513]
- Visconti M, Rabitti PG, Uomo G, Giannattasio F, Varriale M, Russo C. The multiple-organ failure syndrome in acute pancreatitis. Its pathogenesis and treatment. Recenti Prog Med 1995; 86:81-5. [PMID 7754179]
- Kallinen O, Maisniemi K, Böhling T, Tukiainen E, Koljonen V. Multiple organ failure as a cause of death in patients with severe burns. J Burn Care Res 2012; 33:206-11. [PMID 21979843]
- Bradley EL III. A clinically based classification system for acute pancreatitis. Summary of the International Symposium on Acute Pancreatitis, Atlanta, Ga, September 11 through 13, 1992. Arch Surg 1992; 128:586-90. [PMID 8489394]
- Tran DD, Cuesta MA, Schneider AJ, Wesdorp RI. Prevalence and prediction of multiple organ system failure and mortality in acute pancreatitis. J Crit Care 1993; 8:145-53. [PMID 8275159]
- Petrov MS, Shanbhag S, Chakraborty M, Phillips AR, Windsor JA. Organ failure and infection of pancreatic necrosis as determinants of mortality in patients with acute pancreatitis. Gastroenterology 2010; 139:813-20. [PMID 20540942]
- Wilson C, McArdle CS, Carter DC, Imrie CW. Surgical treatment of acute necrotizing pancreatitis. Br J Surg 1988; 75:1119-23. [PMID 3208048]
- Mounzer R, Langmead CJ, Wu BU, Evans AC, Bishehsari F, Muddana V, et al. Comparison of existing clinical scoring systems to predict persistent organ failure in patients with acute pancreatitis. Gastroenterology 2012; 142:1476-82. [PMID 22425589]
- Mofidi R, Duff MD, Wigmore SJ, Madhavan KK, Garden OJ, Parks RW. Association between early systemic inflammatory response, severity of multiorgan dysfunction and death in acute pancreatitis. Br J Surg 2006; 93:738-44. [PMID 16671062]
- Mole DJ, Olabi B, Robinson V, Garden OJ, Parks RW. Incidence of individual organ dysfunction in fatal acute pancreatitis: analysis of 1024 death records. HPB 2009; 11:166-70. [PMID 19590643]
- Vincent JL, Moreno R, Takala J, Willatts S, De Mendonça A, Bruining H, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. Intensive Care Med 1996; 22:707-10. [PMID 8844239]
- Vincent JL, De Mendonca A, Cantraine F et al. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study. Crit Care Med 1998; 26:1793-800. [PMID 9824069]
- Ferreira FL, Bota DP, Bross A, Mélot C, Vincent JL. Serial evaluation of the SOFA score to predict outcome in critically ill patients. JAMA 2001; 286:1754-8. [PMID 11594901]
- Moreno R, Vincent JL, Matos R, Mendonça A, Cantraine F, Thijs L, et al. The use of maximum SOFA score to quantify organ dysfunction/failure in intensive care. Results of a prospective, multicentre study. Intensive Care Med 1999; 25:686-96. [PMID 10470572]
- Tenner S, Sica G, Hughes M, Noordhoek E, Feng S, Zinner M, Banks PA. Relationship of necrosis to organ failure in severe acute pancreatitis. Gastroenterology 1997; 113:899-903. [PMID 9287982]
- Yang XN, Guo J, Lin ZQ, Huang L, Jin T, Wu W, et al. The study on causes of death in fulminant pancreatitis at early stage and late stage. Sichuan Da Xue Xue Bao Yi Xue Ban 2011; 42:686-90. [PMID 22007499]
- Halonen KI, Pettilä V, Leppäniemi AK, Kemppainen EA, Puolakkainen PA, Haapiainen RK. Multiple organ dysfunction associated with severe acute pancreatitis. Crit Care Med 2002; 30:1274-9. [PMID 12072681]
- Petrov MS, Vege SS, Windsor JA. Global survey of controversies in classifying the severity of acute pancreatitis. Eur J Gastroenterol Hepatol 2012; 24:715-21. [PMID 22382706]
- Zhu AJ, Shi JS, Sun XJ. Organ failure associated with severe acute pancreatitis. World J Gastroenterol 200; 9:2570-3. [PMID 14606099]
- Mole DJ, McClymont KL, Lau S, et al.Mole DJ, McClymont KL, Lau S, Mills R, Stamp-Vincent C, Garden OJ, Parks RW. Discrepancy between the extent of pancreatic necrosis and multiple organ failure score in severe acute pancreatitis. World J Surg 2009; 33:2427-32. [PMID 19641951]
- Zimmerman JE, Knaus WA, Wagner DP, Sun X, Hakim RB, Nystrom PO. A comparison of risks and outcomes for patients with organ system failure: 1982-1990. Crit Care Med 1996; 24:1633-41. [PMID 8874298]
- Tilney NL, Bailey GL, Morgan AP. Sequential system failure after rupture of AAA: An unsolved problem in postoperative care. Ann Surg 1973; 178:117-22. [PMID 4723419]
- Büchler MW, Gloor B, Müller CA, Friess H, Seiler CA, Uhl W. Acute necrotizing pancreatitis: treatment strategy according to the status of infection. Ann Surg 2000; 232:619-26. [PMID 11066131]
- Lutfarakhmanov II, Mironov P, Timerbulatov M. Prognostic value of the pattern of multiple organ dysfunctions in severe acute pancreatitis. Anesteziol Reanimatol 2007; 2:44-7. [PMID 17564000]
- Rocha FG, Benoit E, Zinner MJ, Whang EE, Banks PA, Ashley SW, Mortele KJ. Impact of radiologic intervention on mortality in necrotizing pancreatitis: the role of organ failure. Arch Surg 2009; 144:261-5. [PMID 19289666]
- Lankisch PG, Pflichthofer D, Lehnick D. Acute pancreatitis: which patient is most at risk? Pancreas 1999; 19:321-4. [PMID 10547190]
- Petrov MS. Predicting the severity of acute pancreatitis: Choose the right horse before hitching the cart. Dig Dis Sci 2011; 56:3402-4. [PMID 21971951]
- Van Santvoort HC, Bakker OJ, Bollen TL et al. A conservative and minimally invasive approach to necrotizing pancreatitis improves outcome. Gastroenterology 2011; 141:1254-63. [PMID 21741922]
- Isenmann R, Rau B, Beger HG. Early severe acute pancreatitis: characteristics of a new subgroup. Pancreas 2001; 22:274-8. [PMID 11291929]
- Remes-Troche JM, Uscanga LF, Peláez-Luna M, Duarte-Rojo A, González-Balboa P, Teliz MA, et al. When should we be concerned about pancreatic necrosis? Analysis from a single institution in Mexico City. World J Surg 2006; 30:2227-33. [PMID 17103098]
- Lankisch PG, Pflichthofer D, Lehnick D. No strict correlation between necrosis and organ failure in acute pancreatitis. Pancreas 2000; 20:319-22. [PMID 10766460]
- Maraví Poma E, Laplaza Santos C, Gorraiz López B, Albeniz Arbizu E, Zubia Olascoaga F, Petrov MS, et al. Clinical pathways in acute pancreatitis: recommendations for early multidisciplinary management. Med Intensiva 2012; 36:351-7. [PMID 22564789]
- Petrov MS, Windsor JA. Severity of acute pancreatitis: impact of local and systemic complications. Gastroenterology 2012; 142:e20-1. [PMID 22542833]
- Stewart GB, Altman DG, Askie LM, Duley L, Simmonds MC, Stewart LA. Statistical analysis of individual participant data meta-analyses: a comparison of methods and recommendations for practice. PloS One 2012; 7:e46042. [PMID 23056232]
- Chalmers I. The Cochrane collaboration: preparing, maintaining, and disseminating systematic reviews of the effects of health care. Ann N Y Acad Sci 1993; 703:156-65. [PMID 8192293]
- Petrov MS. Abdominal fat: a key player in metabolic acute pancreatitis. Am J Gastroenterol 2013; 108:140-2. [PMID 23287945]
- Simmonds MC, Higgins JP. Covariate heterogeneity in meta-analysis: criteria for deciding between meta-regression and individual patient data. Stat Med 2007; 26:2982-99. [PMID 17195960]
- Stewart LA, Clarke MJ. Practical methodology of meta-analyses (overviews) using updated individual patient data. Stat Med 1995; 14:2057-79. [PMID 8552887]
- Stewart L, Parmar M. Meta-analysis of the literature or of individual patient data: is there a difference? Lancet 1993; 341:418-22. [PMID 8094183]
- Simmonds MC, Higgins JP, Stewart LA, Tierney JF, Clarke MJ, Thompson SG. Meta-analysis of individual patient data from randomized trials: a review of methods used in practice. Clin Trials 2005; 2:209-17. [PMID 16279144]
- Marshall JC, Cook DJ, Christou NV, Bernard GR, Sprung CL, Sibbald WJ. Multiple organ dysfunction score: a reliable descriptor of a complex clinical outcome. Crit Care Med 1995; 23:1638-52. [PMID 7587228]
- Fisher DJ, Copas AJ, Tierney JF, Parmar MK. A critical review of methods for the assessment of participant level interactions in individual participant data meta-analysis of randomised trials and guidance for practitioners. J Clin Epid 2011; 64:949-67. [PMID 21411280]
- Tudor SC, Williamson PR, Marson AG. Investigating heterogeneity in an individual participant data meta-analysis of time to event outcomes. Stat Med 2005; 24:1307-19. [PMID 15685717]
- Simmonds MC, Bowden J, Tierney JF, Copas A, Higging JPT. Individual participant data meta-analysis of time-to-event outcomes: one-stage versus two-stage approaches for estimating the hazard ratio under a random effect model. Research Synthesis Methods 2011; 2:150-62.
- R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing: Vienna, Austria: 2012. [ISBN 3-900051-07-0]
- Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. JAMA 2000; 283:2008- [PMID 10789670]
- Riley RD, Lambert PC, Abo-Zaid G. Meta-analysis of individual participant data: rationale, conduct, and reporting. BMJ 2010; 340:521-5. [PMID 20139215]
- Stewart LA, Tierney JF, Burdett S. Do systematic reviews based on individual participant data offer a means of circumventing biases associated with trial publications? In: Rothstein H, Sutton A, Borenstein M. Publication Bias in Meta-Analysis: Prevention, Assessment and Adjustments: John Wiley & Sons, 1005:261-86. [ISBN 978-0-470-87014-3]
- Bradley EL III. Atlanta redux: revisiting the severity stratification system for acute pancreatitis. Ann Surg 2012; 256:881-2. [PMID 23108124]
- De Campos T, Parreira JG, Assef JC, Rizoli S, Nascimento B, Fraga GP. Classification of of severity of acute pancreatitis. Rev Col Bras Cir 2013; 40:164-8.
- Uomo G, Dellinger EP, Forsmark CE, Layer P, Lévy P, Maraví-Poma E, et al. Pancreatitis Across Nations Clinical Research and Education Alliance (PANCREA). International multidisciplinary classification of acute pancreatitis severity: The 2013 Italian edition. Minerva Medica 2013 (in print).
- Maraví-Poma E, Dellinger EP, Forsmark CE, Layer P, Lévy P, Shimosegawa T, et al. International multidisciplinary classification of acute pancreatitis severity: The 2013 Spanish edition. Med Intensiva 2013. [PMID 23747189]
- Layer P, Dellinger EP, Forsmark CE, Lévy P, Maraví-Poma E, Shimosegawa T, et al. International multidisciplinary classification of acute pancreatitis severity: The 2013 German edition. Z Gastroenterol 2013; 51:544-50. [PMID 23740353]



