Abstract
Pancreatic cancer ranks among many of the death causes linked to cancer. The average diagnostic scale of pancreatic cancer is around
31 mm & hasn't substantially changed in the past thirty years. The late-presenting indications were associated with poor early tumour
diagnosis. Commonly used imaging techniques used in the pancreatic cancer diagnosis is Magnetic Resonance Imaging, Endoscopic
Ultrasound, and Computer Topography. In the Pancreatic Ductal Adenocarcinoma treatment, vascular resection remains a topic of debate.
Vascular resection should only be conducted on carefully selected subjects that have an proof for the occurrence of resectable tumours or
borderline resectability tumours from the pre-operative imaging investigations. Resection at an early stage of pancreatic cancers is the
best chance of cure. Venous resection and reconstruction have become a standard technique to achieve negative margins, and in complex
venous resections/reconstructions, it is highly advisable to seek the help of experienced vascular surgeons.
Keywords
Pancreatic cancer; Portal Vein; Pancreaticoduodenectomy
Abbreviations
EU Endoscopic Ultrasound; CT Computer Topography;
MRI Magnetic Resonance Imaging; PDAC Pancreatic Ductal
Adenocarcinoma; PV Portal Vein; SMV Superior Mesenteric Vein;
SMA Superior Mesenteric Artery; NCCN National Comprehensive
Cancer Network; MDT Multidisciplinary Team; EUS Endoscopic
Ultrasonography; ISGPS International Study Group for Pancreatic
Surgery ; PD Pancreaticoduodenectomy
INTRODUCTION
Pancreatic cancer is ranked as the fourteenth
commonest cancer in the world as well as the 7th highest
cause for cancer related mortality. Epidemiology
estimations reported 4.58.918 diagnoses & deaths of
4.32.242 patients from pancreatic cancer worldwide in
2018 [1]. In Europe, there were more than 78,000 new case
subjects in 2012 [2]. Each year in the US, approximately
43,000 people die of pancreatic cancer making it the
4th commonest cancer linked death cause [3]. Despite
investigation and improvements in the treatment of this
ailment, it’s prone to become the 2nd chief cancer-linked
death cause within the next decade [4]. Approximately
55,440 (26,240 women & 29,200 men) were estimated
to be confirmed with pancreatic cancer in the year 2018,
and approximately 44,330 (21,310 women & 23,020 men)
might have died from pancreatic cancer [5]. 1-5% of average
long-term rates of survival are linked to pancreatic cancer
PDAC (pancreatic ductal adenocarcinoma), demonstrating poor predicted survival [6]. A number of factors led
to an increased pancreatic cancer risk. Such factors of
risk range from; usage of tobacco, obesity, overweight,
occupational exposure to certain chemicals (benzene,
dyes, petrochemicals & pesticides), family history,
ethnicity, gender, age, hereditary inherited syndromes,
chronic pancreatitis, diabetes, stomach problems, liver
cirrhosis, diets, physical inactivity, alcohol and coffee [7].
Pancreatic cancer signs & indications differ depending on
the location & tumour stage. The tumours at the pancreas
head cause obstructive jaundice & loss of weight resulting
in diarrhoea & steatorrhea. Tumours of the tail & body
usually lead to pain in the abdomen & loss of weight. Pain
is also commonly linked to pancreatic cancer. The pain
typically acts as a dull, deep pain, originating from the
upper abdomen, radiating to the back [8].
PDAC is one of the few poorly predicted cancers, with
less than five percent of subjects surviving five years after
diagnosis. Surgical resection in these cases is the only hope
of curative treatment. Though, only 10 to 20 percent of
subjects are fit for resection as nearly fifty percent present
with metastatic & thirty five percent with locally advanced
surgically un-resectable disease. PDAC's poor prognosis
is primarily related to late diagnosis [9, 10] These Days,
radical surgical intervention for pancreatic cancer patients
is the only possibly therapeutic option. Radical surgical
resection accompanied by adjuvant chemotherapy can be
carried out in around twenty percent of all PDAC subjects
during the diagnosis period & is quite often the only hope
for subjects' long-term survival, with an estimated five-year
survival of 20 to 25% [9, 11]. During diagnosis, higher then
eighty percent of them are un-resectable owing to invasion
of retroperitoneal tissue, PV (Portal Vein)/SMV (Superior Mesenteric Vein), hepatic or peritoneal metastases
development, invasion of the mesenteric artery, or failure
to withstand significant surgical resection. Extended
procedures, comprising vascular resections, have become
more common in specialist centers as a consequence of
advanced technologies & surgical procedures [12]. This
has resulted in a substantial improvement in pancreatic
surgery & has broadened the resectability boundary &
increased the chance of obtaining a curative surgical
strategy in pancreatic cancer patients associated with
neoadjuvant & adjuvant treatment approaches. Highlevel
of biological activity & early retroperitoneal tissue
involvement, lymph nodes, & peri-pancreatic blood
vessels are the characteristics of pancreatic carcinoma.
Most of the pancreatic cancers are detected at an advanced
phase. About thirty to thirty five percent are graded as unresectable
due to the isolated participation of the portal
vein/superior mesenteric [13]. For the first time, Fortner
systematically presented the resection idea of the PV for
complete tumour removal [14]. At high volume pancreatic
centers, resection of portomesenteric vein is currently
considered as a standard protocol. For a modern pancreatic
surgeon, vascular operating experience is essential.
Only resections of artery are still a contentious topic
nowadays. Nonetheless, instances of resection comprising
reconstruction of major arteries like hepatic artery, SMA
(Superior Mesenteric Artery) & the coeliac axis have been
recorded, even though in small series of case [15]. With
this context here, the techniques, indications & major
consequences of vascular resection & reconstruction for
extensive pancreatic cancer surgery were reviewed by us.
Classification of PDAC
The pancreatic tumours were traditionally been
considered either un-resectable or resectable. NCCN
(National Comprehensive Cancer Network) was the first
to propose definition for borderline resectable PDAC, that
applies to tumours affecting surrounding structures as not
to be explicitly un-resectable nor explicitly resectable [16].
Aggressive treatment of this community of neoadjuvant
chemotherapy patients has enabled surgery to be
practicable & advanced PDAC surgical methods, including
vascular & multivisceral resections, have been performed
widely [16, 17]. However, vascular resection remains a
topic of discussion in the PDAC management, and hence this
assessment elasticities and overview of the management &
abreast knowledge on vascular resection like indications,
techniques, major outcomes in PDAC surgery.
For localized PDAC, three resectability grades
are described; these are “resectable”, “borderline
resectable”, & “unresectable”, summarized in (Table 1)
[18]. If the celiac trunk & SMA, the SMV & PV are patent,
& if there are no distant metastases then pancreatic
ductal adenocarcinoma is well-defined as resectable.
However, more subjects have been encompassed in a
growing borderline resectable disease category with the
advancement of more comprehensive tools of imaging &
surgical procedures [18, 19]. Patient’s with focal tumour
abutment of superior mesenteric artery (<180°), gastroduodenal
artery encasement up to the hepatic artery, or
SMV/PV involvement that can be resected & reconstructed.
Patients with tumour encasement (more than half of
the vessel circumference) or an occlusion/thrombus
of superior mesenteric artery, an un-re-constructable
superior mesenteric vein or SMV-PV confluence occlusion,
or a direct involvement of the aorta, inferior vena cava,
or celiac axis are not fit for surgery [18]. In combination
with vascular resection, the basis of pancreatectomy is to
upsurge the likelihood to attain a curative R0 resection.
Neoadjuvant method is not advised in venous borderline
resectability, but upfront surgery must be carried out
instead, & if the intraoperative outcome matches the
situation of presumed borderline as described above
completed as an en bloc tumour removal with venous
replacement [18, 19]. Subjects classified as borderline
resectable based on features of arterial involvement
observed at imaging ought to go through surgical
examination to attain further confirmation of any
arterial infiltration, and if there is confirmation of an
arterial borderline resectability intra-operatively as a
true arterial involvement, palliative treatment ought to
be considered as the standard of care [18, 19].

Indications for Vascular Resection
Extended surgical methods, such as multivisceral & vascular
resections, are been performed commonly in Pancreatic ductal
adenocarcinoma owing to improved surgical procedure &
intensive care, including exact management of complications
[17]. Combined PV resection with pancreatectomy ought to
be addressed with a view to attain clear margins of resection
based on pre-operative imaging in suspectable cases of
portal vein invasion instead of deciding purely on the basis
of operational findings. All subjects ought to go through CT
(contrast-enhanced tomography) as regular pre-operative
work up. The development of computed axial tomography
with multislice multi-detector allows imaging of entire
pancreas in the peak contrast intensification. Also, it is also possible to process the information from the
contrast-enhanced tomography to obtain 3D images &
visualizing different view planes. Spiral computed axial
tomography with IV contrast & thin-section technique may
precisely evaluate the relationships of low-density tumor
formation to the celiac trunk, SMA & superior mesentericportal
vein confluence. Based on the discussion of MDT
(Multidisciplinary Team), MRI, EUS & laparoscopy must be
carried out on an individual subject basis. MRI is generally
prescribed when liver metastasis is suspected to be
present. As per Ishikawa et al [20] & Nakao et al [21], the
indications are confined to unilateral (≤ 180°) segmental
vascular involvement. Particular attention was given to
the omission of the deep retroperitoneal invasion cases,
characterized by the intact connective tissue’s absence
between the right lateral side of SMA & the tumor. As an
absolute contraindication, the involvement of isolated
artery isn’t accepted. At this stage, EUS (Endoscopic
Ultrasonography) is more effective in detecting invasion
in the porto-mesenteric system & in the specialized
medical centers it is a standard procedure. Tumors with
simultaneous numerous blood vessels involvement at
the same time or with a massive retroperitoneal invasion
are treated as resectable only in the case of neoadjuvant
chemotherapy sensitivity.
As per these suggestions, pre-operative resectability
assessment ought to be done on the basis of CT scan
with a protocol that is pancreas-specific, such as a
“hydropancreas” CT. For localized Pancreatic ductal
adenocarcinoma, 3 resectability grades are defined, these
are “resectable,” “borderline resectable,” & “unresectable”
[18].
When there is no presence of vascular attachment i.e.
no distortion of the venous structures & clearly preserved
fat planes toward the arteries, then a tumour is classified
as resectable. When occlusion/narrowing/distortion of
the mesentericoportal veins is diagnosed with a technical
reconstruction possibility on the veins’ distal & proximal
margin or an attachment at the hepatic artery without the
celiac axis or a semi circumferential abutment (≤ 180°) of
the SMA then the resectability is classified as borderline.
Tumours with celiac trunk and/or superior mesenteric
artery infiltration or as tumours that involves the SMV,
PV, or their confluence then these locally advanced
tumour is classified as surgically unresectable tumours.
The “encasement” term means that the tumour cannot be
distinguished from the blood vessel for more than 180° of
the latter’s circumferences. A tumour is well-defined as
unresectable when it has distant presence of metastases,
having superior mesenteric artery encasement >180°, any
celiac abutment, unreconstructible superior mesenteric
vein/PV, invasion or encasement of aortic/IVC, or lymph
nodes metastases beyond the resection field.
Given the advancement of pancreatic imaging, it might
be difficult to distinguish between the resectable disease
(stage I & II) & locally advanced disease (stage III) & such
cases are classified as “borderline resectability”. Vascular resections are typically needed in cases often defined
as having “borderline resectable” findings. Borderline
resectable carcinoma is defined as per 2009, exert
consensus statement [22] & encompasses involvement
of short superior mesenteric vein/portal vein with free
proximal & distal venous segments, allowing secure
reconstruction & superior mesenteric artery less than
180° or involvement of short hepatic artery with intact
truncus coeliacus. The discrepancy from the classification
of M.D. Anderson Group is taken into consideration the
tumours, abutting or encasing (relying on the tumourvessel
interface degree) the superior mesenteric vein/
portal vein borderline but is not resectable [23].
The Cao et al TVI-classification takes into account the
circumferential interface of radiographic tumour vein & its
importance as a prognostic tool for concomitant resection
of vessel [24].
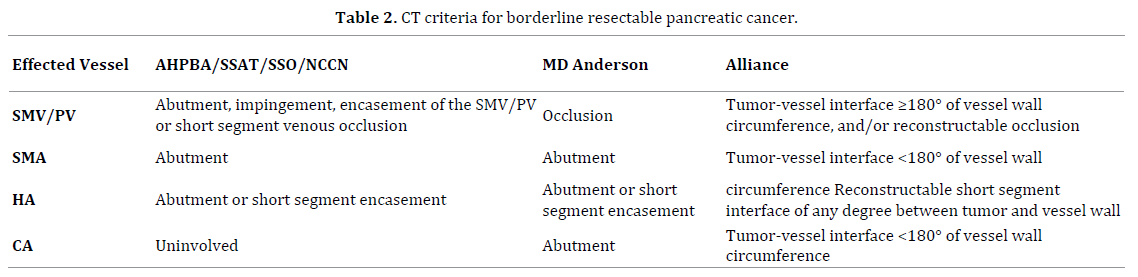
A consensus statement standardizing the definition
of the “borderline resectability” term in compliance with
the NCCN (National Comprehensive Cancer Network)
guidelines and also the concept of extended resections
issued by the ISGPS (International Study Group for
Pancreatic Surgery) (Table 2) [18, 22, 23].
The methodology ought to be distinct when diagnosing
the borderline findings in the involvement of arterial &
venous vessel. In venous borderline resectability, the
neoadjuvant therapy is not advised. Upfront surgery
ought to be carried out &, if the intra-operative finding
matches the situation of presumed borderline as per above
demarcation, completed as an en bloc tumour removal
with venous replacement [18]. In comparison, palliative
treatment must be considered the standard of care when
the arterial borderline resectability which was suspected is
confirmed intra-operatively as a true arterial involvement.
The neoadjuvant therapy may be used to stratify & identify
the subjects with borderline findings that don’t profit from
extended resections. Subjects under neoadjuvant therapy
with a clear progression of tumour must be omitted from
secondary exploration. Vascular resection should be
carried out in subjects who are cautiously chosen with data
for the resectable tumours’ presence or with borderline
resectability tumours from pre-operative computed axial
tomography.
For Vascular Resection and Reconstruction
The NCCN (National Comprehensive Cancer Network)
guidelines definition is based on the tumor relation with
the involved major vessels (Table 3) [25].

Depending on the extent of the invasion of the PV &
SMV, different techniques for resection & reconstruction
are used. In minimal invasion cases, a partial resection
& reconstruction with an autologous patch may be
performed. A peritoneal patch has been described as
feasible [26]. In cases of broader invasion, segmental
resection and reconstruction should be performed. When
an end-to-end anastomosis isn’t possible, autologous,
homologues, or prosthetic (ring) grafts are the options [27]. The classification proposed by the International Study
Group of Pancreatic Surgery divided the venous resection
in 4 types depending on the performed reconstruction:
venorrhaphy, patch, primary anastomosis, & interposition
conduit [28]. However, with large-scale mobilization of the
root of the mesentery, an end to end anastomosis is almost
always likely. Technically, an extensive Kocher Maneuver
together with a Cattell-Braasch maneuver is a safe technic
to perform pancreatic and venous resection. 45 subjects,
who went through pancreatectomy with portomesenteric
resection in a retrospective study, none had a thrombosis
after a median follow-up of 22 months [29].
In a retrospective examination of a prospectively
gathered database of two hundred forty one subjects who
went through pancreatectomy with venous resection, no
differences in mortality, morbidity & long-term survival
were noticed related to patients who underwent a standard
resection [30, 31]. In a large multicenter retrospective
review from the United Kingdom that included 1588
subjects with borderline resectable tumors, venous
resection in pancreatic cancer surgery was also reported
as safe & feasible [32]. Median survival (eighteen months
for the standard procedure &18.2 months for patients
undergoing venous resection, P=0.0001) and in hospital
mortality were similar in both groups [33]. Thus, if a
resection with a tumor negative-margin seems possible,
venous resection should be performed if necessary. Such
an approach is now internationally well accepted.
Venous Resections
Involvement of major vessel in PDAC subjects has been a
contraindication to resection, historically. Fortner, in 1973
outlined a surgical method of regional pancreatectomy
which involves en bloc peripancreatic soft tissue resection,
regional lymph nodes with portal vein (type I) resection,
or major artery resection & reconstruction (type II).
While these extended resections attained improved
rates of resectability, high mortality (twenty three
percent) & high morbidity (sixty seven percent) linked to low rates of survival (three-years survival rate three
percent) inhibited generalized adoption of resection &
reconstruction of major vessel [14]. Nevertheless, major
improvements in surgical & radiological procedures could
be accomplished, which would result in enhanced preoperative
staging, better selection of subjects as well as
reduction of surgical mortality & morbidity [34]. Contrary
to involvement of artery, the superior mesenteric vein
or portal vein invasion isn’t in itself an unresectability
criterion. [35, 36]. Unlike arterial resection, widespread
acceptability of Pancreaticoduodenectomy (PD) with PV
approaches has been achieved in many centers around the
world & can be safely performed with no peri-operative
mortality or morbidity increase in comparison to standard
PD [35, 36, 37, 38]. When there is involvement of Portal
vein or superior mesenteric vein, attempting a resection
is legitimate & venous excision is either performed by a
tangential resection or by a segmental resection [39, 40].
Venous Resection and Reconstruction - Technical
Outcomes
Depending in the type of reconstruction that is
performed, different venous patency and patient outcomes
have been reported. Direct vein reconstruction without
patch or interposition graft has a lower rate of thrombosis
[41]. The length of the reconstruction has also an important
role in patient outcomes. In a Japanese retrospective
analysis of 810 subjects, 9% subjects suffered severe
anastomotic stenosis within the first post-operative year.
A significant part of these subjects was symptomatic with
gastrointestinal bleeding or hepatic encephalopathy.
Operation time over 520 minutes and resection length
over 31mm were predictors of anastomotic stenosis [42].
Snyder et al reported long-term venous patency
rates after reconstruction of seventy two percent at a
median follow up of 7 months. [25]. Patients with portal
vein thrombosis suffered 24.3 months of worse overall
survival. Median overall survival of the subjects without
portal vein thrombosis was 35.0 months [43]. Prosthetic grafts were associated with a 4 times increased risk of
early portal vein thrombosis. The role of anticoagulation
for these patients is still not clear [44]. In a retrospective
review of 128 subjects who went through portal vein
resection and reconstruction during pancreatectomy,
survival of subject was 66% at one year. The use of a
prosthetic graft was associated with a worse survival [45].
Alternatives to prosthetic grafts could be the use of bovine
pericardium and cold-stored cadaveric venous allograft.
PV reconstruction with the extern iliac vein or peritoneum
has also been reported [27, 46]. In a retrospective review
from Norway, no changes in post-operative morbidity and
mortality were seen when comparing reconstructions
with cold-stored cadaveric venous interposition allografts
or primary end-to-end anastomosis after segmental vein
resections. In addition, 18.6 months was the assessed
median overall survival in subjects who obtained venous
allografts & 20.5 months in the other group [47, 48, 49].
In a recent paper from Germany, the histopathological
infiltration of the portal vein was analyzed as an
outcome factor. Considerably higher metachronous liver
metastasis incidence was seen in subjects with true vein
invasion. 11.9 months was the median overall survival
for these subjects & for those patients without true
venous invasion it was 16.1 months [50]. Subjects with
poorly differentiated tumours after venous resection
had a shorter life span in comparison to those with well
& moderately differentiated pancreatic cancer who had
longer life span (12.5 months median survival vs. 24.5
months, P=0.023) [51]. Thus, pancreatic surgery with vein
resection alone cannot change the tumour biology. Thus,
perioperative treatment and intensified chemotherapy
regimens, including individualized therapy targeting the
metabolic reprogramming in cancer cells, will be more and
more important [52].
Arterial Resection
Ever since fortner first proposed the idea as part of
regional pancreatectomy, since then arterial resection
for PDAC has become a subject of controversy. Venous
resection & reconstruction are quite common nowadays
when the pancreatic tumour can't be isolated from
the adjacent portal vein or superior mesenteric vein.
Nevertheless, due to the high rates of mortality &
morbidity related to arterial resection & reconstruction,
several researchers consider the invasion of hepatic
artery, the celiac axis of the superior mesenteric artery, as
a contraindication to surgery [53, 54]. Lately, with the rise
of effective systemic treatments, emphasis is been focused
on the possible advantage of primary tumour resection,
even in the complex arterial abutment or encasement
setting, particularly when it is the only site of measurable
disease, after neoadjuvant treatment [55]. Even though in
some subjects arterial invasion is classified as borderline
resectable as per the ISGPS consensus statement, an
upfront resection is recommended rarely, even though
it can be conducted technically [18]. In addition, arterial
invasion typically predicts considerable mesenteric
neural plexus involvement with the incapability to attain a negative margin of retroperitoneal resection even with
radical extended surgery. In short, arterial resection can
be safely performed by skilled hands, but so far up to now
it is not represented as standard method of treatment.
Summary
In comparison to no resection, PD with venous
resection particularly with R0 resection increases
survival. When compared to PD with no vascular resection,
morbidity & mortality rates are greater in PD with venous
resection. With respect to PD with venous resection after
neoadjuvant therapy, poorer oncological outcome is
seen in PD with upfront venous resection (increased R1
resection risk, poorer rate of survival). PD with arterial
resection is linked to higher rates of mortality & morbidity
(than venous resection PD) and hasn't really proven to
be of any benefit. A distal splenopancreatectomy with
celiac axis resection is related to higher rates of mortality
& morbidity & the oncological advantage of this method
hasn't been demonstrated clearly. Today, literature offers
further encouragement for neoadjuvant treatment in
pancreatic cancer management. The objective ought to
be to wait for outcomes of RCTs which includes clearly
resectable tumours, neoadjuvant treatment as well as a
complete R0 resection in all subjects needing planned
vascular resection with (or with no) reconstruction. Such
subjects ought to be handled during pancreatic resection
by a skilled team in both pre-operative/neoadjuvant
treatment & vascular resection. Not every center has such
skills/experience hence creating another strong issue
for regionalizing complex cancer care involving multiple
remedies.
Key Recommendations
For operative planning, CT with intravenous
augmentation is the proper imaging modality, but for
searching liver metastasis, MRI is considered better.
To reduce the time of liver ischemia, venous resection
ought to be performed at the end of resection.
The most utilized suture material is Prolene 5/0
Direct anastomosis is the preferential approach for
reconstruction in segmental resection cases.
Left renal vein is the ideal graft
Regular heparin use is controversial- with subcutaneous
40 mg enoxaparin application twice daily, this could be
changed.
CONCLUSION
Pancreatic cancer has had a poor prognosis history
due to its late detection. A family history of pancreatic
cancer carefully monitored with a genetic screening has
the ability for predicting the early detection, expected
incidence & potential pancreatic cancer management.
In addition, further screening modalities & examination
with imaging techniques & interventional radiology use
have helped enhance early detection and pancreatic
cancer management. Resection at an early disease stage of pancreatic cancer is the best chance of cure. Venous
resection and reconstruction have become a standard
technique to achieve negative margins. In complex venous
resections/reconstructions it is highly advisable to seek
the help of experienced vascular surgeons.
Conflicts of Interest
All named authors hereby declare that they have no
conflicts of interest to disclose.
References
- International Agency for Research on Cancer. Global cancer observatory. World Health Organization. http://gco. iarc. fr. Accessed. 2018 Nov; 8.
- Ferlay J, Steliarova-Foucher E, Lortet-Tieulent J, Rosso S, Coebergh JWW, Comber H, et al. Cancer incidence and mortality patterns in Europe: estimates for 40 countries in 2012. Eur J Cancer 2013; 49:1374-1403. [PMID: 23485231]
- Siegel RL, Miller KD Jemal A. CA Cancer J Clin 2017; 67:7-30. [PMID: 28055103]
- Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res 2014; 74:2913-2921. [PMID: 24840647]
- American Cancer Society. Cancer Facts and Figures 2017. 1-71. Genes Dev 2017;21(20):2525-38.
- Siegel R, DeSantis C, Jemal A. Colorectal cancer statistics, 2014. CA Cancer J Clin 2014; 64:104-117. [PMID: 24639052]
- Hariharan D, Saied A, Kocher HM. Analysis of mortality rates for pancreatic cancer across the world. HPB (Oxford) 2008; 10:58-62. [PMID: 18695761]
- Dragovich T, Espat JN, Erickson RA. Pancreatic Cancer Clinical Presentation: History, Physical Examination. Medscape. 2017.
- Hartwig W, Hackert T, Hinz U, Gluth A, Bergmann F, Strobel O, et al. Pancreatic cancer surgery in the new millennium: better prediction of outcome. Ann Surg 2011; 254:311-319. [PMID: 21606835]
- Hackert T, Büchler MW. Pancreatic cancer: advances in treatment, results and limitations. Dig Dis 2013; 31:51-56. [PMID: 23797123]
- Schnelldorfer T, Ware AL, Sarr MG, Smyrk TC, Zhang L, Qin R, et al. Long-term survival after pancreatoduodenectomy for pancreatic adenocarcinoma: is cure possible? Ann Surg 2008; 247:456-462. [PMID: 18376190]
- Hartwig W, Werner J, Jäger D, Debus J, Büchler MW. Improvement of surgical results for pancreatic cancer. Lancet Oncol 2013; 14:e476-485. [PMID: 24079875]
- Heinemann V, Haas M, Boeck S. Neoadjuvant treatment of borderline resectable and non-resectable pancreatic cancer. Ann Oncol 2013; 24:2484-2492. [PMID: 23852311]
- Fortner JG. Regional resection of cancer of the pancreas: a new surgical approach. Surg 1973; 73:307-320. [PMID: 4265314]
- Mollberg N, Rahbari NN, Koch M, Hartwig W, Hoeger Y, Büchler MW, et al. Arterial resectionduring pancreatectomy for pancreatic cancer: a systematic review and meta-analysis. Annals of surgery 2011; 254:882-893. [PMID: 22064622]
- National Comprehensive Cancer Network. Clinical practice guidelines in oncology: pancreatic adenocarcinoma. Version 1.2008 and 1.2014.
- Hackert T, Tjaden C, Büchler MW. Developments in pancreatic surgery during the past ten years. Zentralbl Chir 2014; 139:292-300. [PMID: 23824618]
- Bockhorn M, Uzunoglu FG, Adham M, Imrie C, Milicevic M, Sandberg AA, et al. Borderline resectable pancreatic cancer: a consensus statement by the International Study Group of Pancreatic Surgery (ISGPS). Surgery 2014; 155:977-988. [PMID: 24856119]
- Hartwig W, Vollmer CM, Fingerhut A, Yeo CJ, Neoptolemos JP, Adham M, et al. Extended pancreatectomy in pancreatic ductal adenocarcinoma: definition and consensus of the International Study Group for Pancreatic Surgery (ISGPS). Surgery 2014; 156:1-14. [PMID: 24856668]
- Ishikawa O, Ohigashi H, Imaoka S, Furukawa H, Sasaki Y, Fujita M, et al. Preoperative indications for extended pancreatectomy for locally advanced pancreas cancer involving the portal vein. Ann Surg 1992; 215:231. [PMID: 1543394]
- Kaneko T, Nakao A, Inoue S, Harada A, Nonami T, Itoh S, et al. Intraportal endovascular ultrasonography in the diagnosis of portal vein invasion by pancreatobiliary carcinoma. Ann Surg 1995; 222:711. [PMID: 8526577]
- Callery MP, Chang KJ, Fishman EK, Talamonti MS, Traverso LW, Linehan DC. Pre-treatment assessment of resectable and borderline resectable pancreatic cancer: expert consensus statement. Ann Surg Oncol 2009; 16:1727-1733. [PMID: 19396496]
- Varadhachary GR, Tamm EP, Abbruzzese JL, Xiong HQ, Crane CH, Wang H, et al. Borderline resectable pancreatic cancer: definitions, management, and role of preoperative therapy. Ann Surg Oncol 2006; 13:1035-1046. [PMID: 16865597]
- Cao HST, Balachandran A, Wang H, Nogueras-González GM, Bailey CE, Lee JE, et al. Radiographic tumor-vein interface as a predictor of intraoperative, pathologic, and oncologic outcomes in resectable and borderline resectable pancreatic cancer. J Gastrointest Surg 2014; 18:269-278. [PMID: 24129826]
- Bond-Smith G, Banga N, Hammond TM, Imber CJ. Pancreatic adenocarcinoma. BMJ 2012; 344:e2476. [PMID: 22592847]
- Dokmak S, Aussilhou B, Sauvanet A, Nagarajan G, Farges O, Belghiti J. Parietal peritoneum as an autologous substitute for venous reconstruction in hepatopancreatobiliary surgery. Ann Surg 2015; 262:366-371. [PMID: 25243564]
- Yoshioka M, Uchinami H, Watanabe G, Iida M, Nakagawa Y, Miyazawa H, et al. Domino reconstruction of the portal vein using the external iliac vein and an ePTFE graft in pancreatic surgery. Journal of Gastrointestinal Surgery. 2017; 21:1278-1286. [PMID: 28378316]
- Dunne DFJ, Kleeff J, Yip VS, Halloran C, Ghaneh P, Neoptolemos JP. Arterial resection in pancreatic cancer. In Pancreatic Cancer. Springer New York 2017; 1-16.
- Chiaro MD, Segersvärd R, Rangelova E, Coppola A, Scandavini CM, Ansorge C, et al. Cattell-Braasch maneuver combined with artery-first approach for superior mesenteric-portal vein resection during pancreatectomy. J Gastrointest Surg 2015; 19:2264-2268. [PMID: 26423804]
- Beltrame V, Gruppo M, Pedrazzoli S, Merigliano S, Pastorelli D, Sperti C. Mesenteric-portal vein resection during pancreatectomy for pancreatic cancer. Gastroenterol Res Pract 2015; 2015:659730. [PMID: 26609307]
- Ramacciato G, Nigri G, Petrucciani N, Pinna AD, Ravaioli M, Jovine E, et al. Pancreatectomy with mesenteric and portal vein resection for borderline resectable pancreatic cancer: multicenter study of 406 patients. Ann Surg Oncol 2016; 23:2028-2037. [PMID: 26893222]
- Allema JH, Reinders ME, Van Gulik TM, Van Leeuwen DJ, De Wit LT, Verbeek PC, et al. Portal vein resection in patients undergoing pancreatoduodenectomy for carcinoma of the pancreatic head. Br J Surg 1994; 81:1642-1646. [PMID: 7827892]
- Ravikumar R, Sabin C, Hilal MA, Bramhall S, White S, Wigmore S, et al. Portal vein resection in borderline resectable pancreatic cancer: a United Kingdom multicenter study. J Am Coll Surg 2014; 218:401-411. [PMID: 24484730]
- Bang S, Chung HW, Park SW, Chung JB, Yun M, Lee JD, et al. The clinical usefulness of 18-fluorodeoxyglucose positron emission tomography in the differential diagnosis, staging, and response evaluation after concurrent chemoradiotherapy for pancreatic cancer J Gastrointest Surg 2006; 40:923-939. [PMID: 11992799]
- Müller SA, Hartel M, Mehrabi A, Welsch T, Martin DJ, Hinz U, et al. Vascular resection in pancreatic cancer surgery: survival determinants. J Gastrointest Surg 2009; 13:784.
- Kim PTW, Wei AC, Atenafu EG, Cavallucci D, Cleary SP, Moulton CA, et al. Planned versus unplanned portal vein resections during pancreaticoduodenectomy for adenocarcinoma. Br J Surg 2013; 100:1349-1356. [PMID: 23939847]
- Riediger H, Makowiec F, Fischer E, Adam U, Hopt UT. Postoperative morbidity and long-term survival after pancreaticoduodenectomy with superior mesenterico-portal vein resection. J Gastrointest Surg 2006; 10:1106-1115. [PMID: 16966029]
- Hartel M, Niedergethmann M, Farag-Soliman M, Sturm JW, Richter A, Trede M, et al. Benefit of venous resection for ductal adenocarcinoma of the pancreatic head. Eur J Surg 2002; 168:707-712. [PMID: 15362580]
- Sasson AR, Hoffman JP, Ross EA, Kagan SA, Pingpank JF, Eisenberg BL. En bloc resection for locally advanced cancer of the pancreas: is it worthwhile? J Gastrointest Surg 2002; 6:147-158. [PMID: 11992799]
- Siriwardana HP, Siriwardena AK. Systematic review of outcome of synchronous portal-superior mesenteric vein resection during pancreatectomy for cancer. Br J Surg 2006; 93:662-673. [PMID: 16703621]
- Dua MM, Tran TB, Klausner J, Hwa KJ, Poultsides GA, Norton JA, et al. Pancreatectomy with vein reconstruction: technique matters. HPB 2015; 17:824-831. [PMID: 26223388]
- Fujii T, Nakao A, Yamada S, Suenaga M, Hattori M, Takami H, et al. Vein resections >3 cm during pancreatectomy are associated with poor 1-year patency rates. Surgery 2015; 157:708-715. [PMID: 25704426]
- Snyder RA, Prakash LR, Nogueras-Gonzalez GM, Kim MP, Aloia TA, Vauthey JN, et al. Vein resection during pancreaticoduodenectomy for pancreatic adenocarcinoma: patency rates and outcomes associated with thrombosis. J Surg Oncol 2018; 117:1648-1654. [PMID: 29723419]
- Chandrasegaram MD, Eslick GD, Lee W, Brooke-Smith ME, Padbury R, Worthley CS, et al. Anticoagulation policy after venous resection with a pancreatectomy: a systematic review. HPB. 2014; 16:691-698. [PMID: 24344986]
- Glebova NO, Hicks CW, Piazza KM, Abularrage CJ, Cameron AM, Schulick RD, et al. Technical risk factors for portal vein reconstruction thrombosis in pancreatic resection. J Vasc Surg 2015; 62:424-433. [PMID: 25953018]
- Strobel O, Büchler MW. Peritoneal patch as autologous venous substitute in pancreatic and hepatobiliary surgery. Chirurg 2015; 86:1068. [PMID: 26464344]
- Jara M, Malinowski M, Bahra M, Stockmannn M, Schulz A, Pratschke J, et al. Bovine pericardium for portal vein reconstruction in abdominal surgery: a surgical guide and first experiences in a single center. Dig Surg 2015; 32:135-141. [PMID: 25791515]
- Kleive D, Berstad AE, Sahakyan MA, Verbeke CS, Naper C, Haugvik SP, et al. Portal vein reconstruction using primary anastomosis or venous interposition allograft in pancreatic surgery. J Vasc Surg Venous Lymphat Disord 2018; 6:66-74. [PMID: 29128301]
- Zhang XM, Zhang J, Fan H, He Q, Lang R. Feasibility of portal or superior mesenteric vein resection and reconstruction by allogeneic vein for pancreatic head cancer—a case-control study. BMC Gastroenterol 2018; 18:49. [PMID: 29661201]
- Mierke F, Hempel S, Distler M, Aust DE, Saeger HD, Weitz J, et al. Impact of portal vein involvement from pancreatic cancer on metastatic pattern after surgical resection. Ann Surg Oncol 2016; 23:730-736. [PMID: 27554501]
- Michalski CW, Kong B, Jäger C, Kloe S, Beier B, Braren R, et al. Outcomes of resections for pancreatic adenocarcinoma with suspected venous involvement: a single center experience. BMC Surg 2015; 15:100.[PMID: 26296752]
- Sunami Y, Rebelo A, Kleeff J. Lipid metabolism and lipid droplets in pancreatic cancer and stellate cells. Cancers 2018; 10:3.
- Fuhrman GM, Leach SD, Staley CA, Cusack JC, Charnsangavej C, Cleary KR, et al. Rationale for en bloc vein resection in the treatment of pancreatic adenocarcinoma adherent to the superior mesenteric-portal vein confluence. Pancreatic Tumor Study Group. Ann Surg 1996; 223:154. [PMID: 8597509]
- Harrison LE, Klimstra DS, Brennan MF. Isolated portal vein involvement in pancreatic adenocarcinoma. A contraindication for resection? Ann Surg 1996; 224:342. [PMID: 8813262]
- Strobel O, Berens V, Hinz U, Hartwig W, Hackert T, Bergmann F, et al. Resection after neoadjuvant therapy for locally advanced, “unresectable” pancreatic cancer. Surgery 2012; 152:S33-S42. [PMID: 22770956]

