Keywords
academic training, education, evidencebased practice, general practice, medical faculty
How this fits in with quality in primary care
What do we know?
Even in countries where academic training is part of the specialty training programme, there are barriers to closing the gap between general practice clinical and academic work. Strategies to improve general practice research bear the potential of creating a gap between the academic and clinical communities.
What does this paper add?
The general level of academic capacity can rise by using participatory action research in developing the faculty for mandatory research training of general practitioners. To succeed fully an inherent barrier of academia itself must, however, be challenged.
Background
Since the beginning of this century, there has been an international campaign to revitalise academic medicine. [1–3]A number of recommendations and initiatives to support primary care research have led to research competencies at senior or elite levels.[4] However, by distinguishing between ‘users of research’, ‘participants in research’ and ‘leaders in research’,[5] there is a risk of a gap between academic and clinical general practitioners (GPs).[6] Networks and workshops to train in research skills for those interested have been established to stimulate the growth of research in general practice.[5,7] Limiting the definition of academic capacity to the elite production of research knowledge, however, is not helpful if the aim is a general increase in GP academic capacity. The World Organisation of Family Doctors has suggested that progress could be achieved through a link to the educational agenda.[8]
In some countries, training critical appraisal is integrated into clinical supervision during GP training. [9] However, previous studies have found various obstacles to building academic capacity in the form of research skills and critical appraisal competencies: trainers lack self-confidence in teaching critical appraisal and research skills;[10] the quality of critical appraisal training in GP training varies greatly;[11] GP trainees perceive the limited training time and a lack of research studies with a primary care focus a hindrance; [10,11] trainers are often aware of the importance of the need to build academic capacity, but fail to prioritise time spent on this in training;[12] and, when trained, the skills learned in the training period are not transferable for use in clinical work after GP training. [10,11]
In 2001, the Danish national regulatory body for doctors introduced ‘research training’ as a mandatory part of all medical specialist training. The aim was to strengthen the skills of future doctors to find and analyse the scientific literature, and to use this knowledge for the critical assessment of established clinical practice.
Denmark’s three regional postgraduate medical educational boards interpreted the national guidelines and defined generic learning outcomes for training. Hospitals and universities were expected to deliver the training.
The Danish Government funded the training. The budget was the equivalent of approximately £3000 per participant, to cover all expenses including salaries, process evaluation, faculty development, meetings, overheads, administration and programme planning. Salaries in Denmark are among some of the highest in Europe, so it is difficult to translate this directly to the UK or other circumstances.
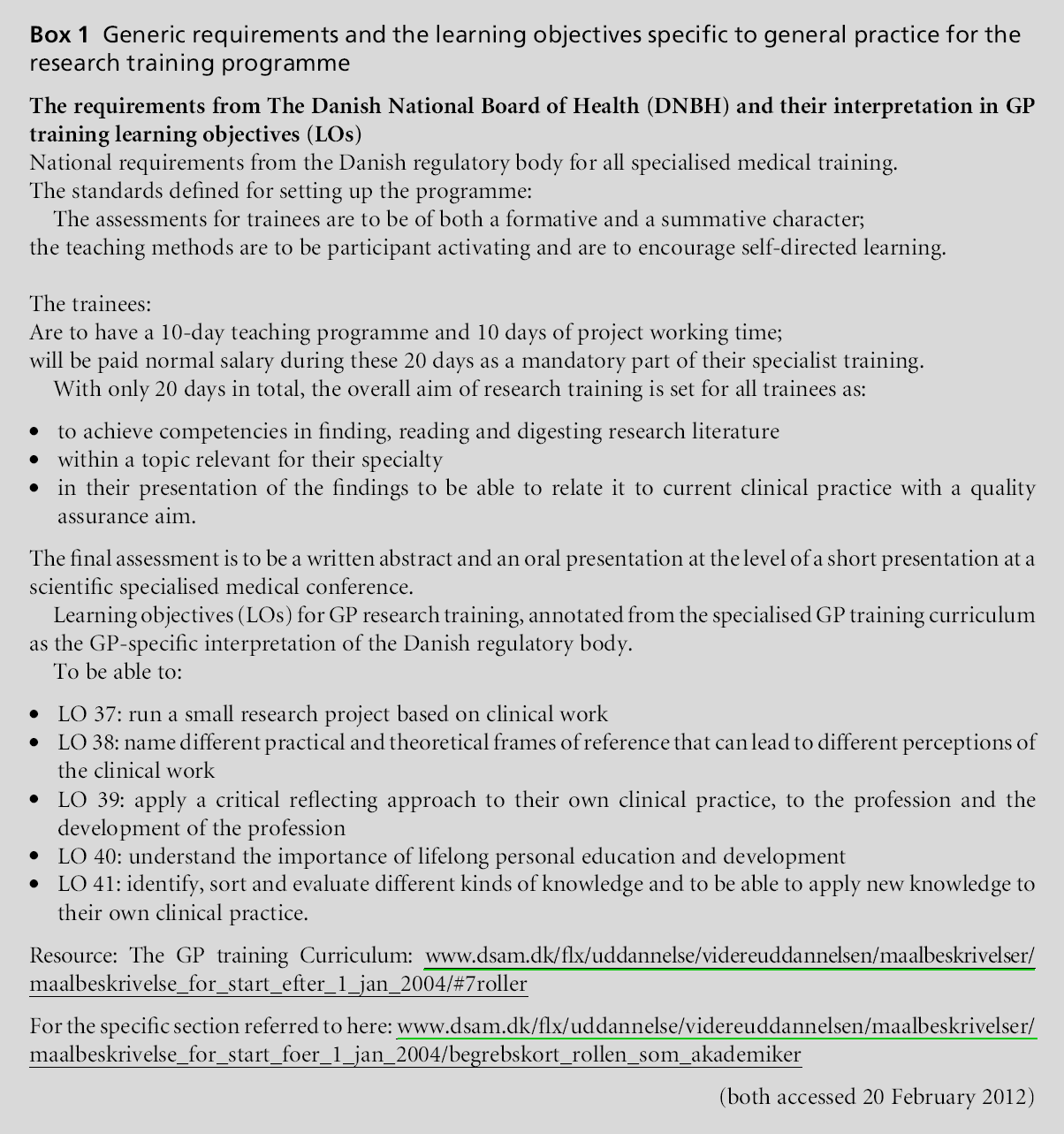
All medical specialties adapted the generic learning outcomes for the research training to reflect their specific clinical context and theoretical basis. For general practice, this meant that research training should function as a learning strategy for five of the 119 major learning objectives in the national GP Curriculum (Box 1).
The Research Unit for General Practice in Copenhagen (RGP) is responsible for the planning and delivery of research training for approximately half of all Danish GP trainees.
In Denmark, GP research activities are mainly done by a group of university academics. The RGP saw the new educational reform as an opportunity to develop the research training programme as a means of raising the academic level, not only among GP trainees, but also, in general, among established GPs.
This paper describes the development of GP research training in the eastern part of Denmark from the beginning of the reform in August 2006 to August 2009. The paper describes the rationale, basic principles and learning points from our experiences with setting up the programme. Collection of evaluation data stopped in 2009, but developments afterwards are also outlined.
Aims and strategies
The national regulatory body outlined the educational agenda: educating doctors through the research training programme so they could learn the skills to critically assess scientific knowledge.
This aim could have been achieved by setting up a training programme with teachers from the university. The RGP, however, also wanted the process to gradually empower the GP community to achieve academic capacity. We therefore decided to deliver the training programme using the existing cohort of GP researchers, GP educators and GP clinicians. The aims were therefore also to:
• create a link between GP researchers and the GP training community
• create an awareness of critical appraisal in surgeries training GPs, allowing GP trainers to experience the relevance of critical appraisal for their own clinical practice.
Methods, design and material
Methods and design to set up the research training programme
The national guideline prescribed assessment of the trainees in the form of a comprehensive project, including communication of the results, with the quality expected of a short paper presentation at conferences or scientific associations (Box 1).
The RGP had previously delivered other research training programmes as part of continuing professional development, and the best evaluated elements were incorporated into the new programme.[13–15] The educational strategy of the programme was inspired by theories of how to support reflective practice,[16] self-directed and problem-based learning,[17,18] supporting the integration of many forms of knowledge, including experience based.[19] The formative evaluation approach[20] was used in the assessment of the individual GP trainee’s work during the programme, and, in the process, evaluation of the development of the research training programme content.
Methods and design to set up the faculty
The educational strategy was first to establish a shared understanding between GP academics, GP educators and GP clinicians. First, using a bottom-up design, we allowed GP educators to develop their research skills and GP researchers to develop their educational skills. Second, we aimed to support the region’s GP educators and academics in learning through their preparation to become teachers, and in learning fromtheir teaching of GP trainees. Building on the GPs’ academic and educational skills, we asked them to interpret the curriculum for the programme.[21,22] In this way, the strategy aimed to ensure that the programme was authentic to general practice. The hope was also that by using local GPs, the teaching and learning activity within the local area would create awareness and skills that would affect their own as well as their colleagues’ clinical work.
Methods and design of the evaluation of the programme
Programme development was based on amulti-method process evaluation in an action research design (participatory evaluation).[17,23–25] The development process continuously involved the teachers and learners, and continuously introduced improvements to the training during the delivery of the research training of the trainees, the teachers, and the steering group (authors CT, ABSN, LJH, CH).
Evaluation material
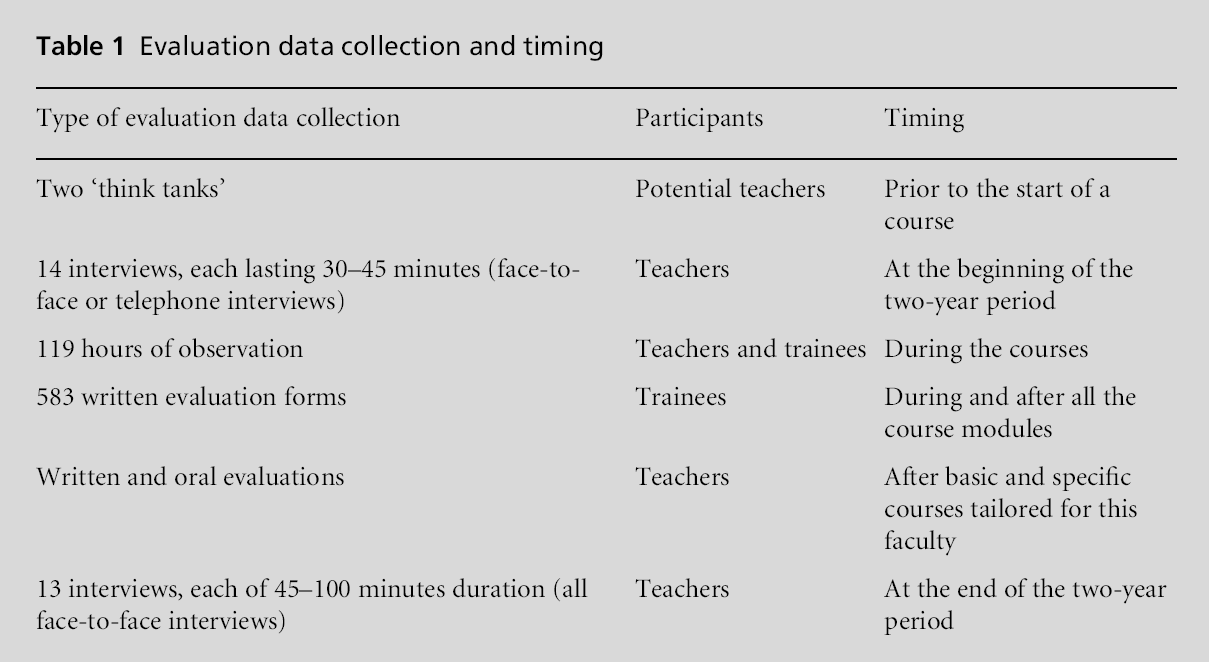
The development and evaluation of the programme therefore overlap. The data were collected in different settings during the development and delivery of the programme. The methods used can be seen in Table 1.[23,26,27]
All interview data were analysed continuously during the development and delivery of the programme using a phenomenological approach with a thematic analysis inspired by Giorgi as described by Malterud.[28]
Weused content analysis for the written evaluations with open-ended questions. Researcher triangulation involved authors LV,RDand CT. All data were used in the development of the programme.
Results
The teaching faculty was developed from 0 to 25 engaged teachers, and the content of the research training programme was developed simultaneously with delivery of the programme.
By August 2009, nine courses had been completed. The continuous evaluation led to multiple adjustments in the programme content and faculty development.
A steering group led the work through several parallel work streams:
• establishment of the teaching faculty
• development of the content of the training programme
• delivering the training to all GP trainees in the region
• creating awareness, understanding and links between academic GPs, GP educators and GP clinicians.
Establishment of the teaching faculty
Research training had not been an element of GP training, so the steering group had to establish a faculty of teachers. The training had to be tailored to general practice usage, so we decided to create a faculty mainly consisting of clinical and academic GPs, with the aim of creating awareness, understanding and links between academic and clinical general practice. Researchers from other disciplines with relevant academic training were also trained to become part of the teaching faculty.
The learning objectives for the research training programme were used by the steering group to define the teaching tasks. To determine the faculty needed for these tasks we set up two ‘think tanks’, run as facilitated reflective forums, to discuss what the participating GPs needed to learn in order to become confident future teachers in the programme.
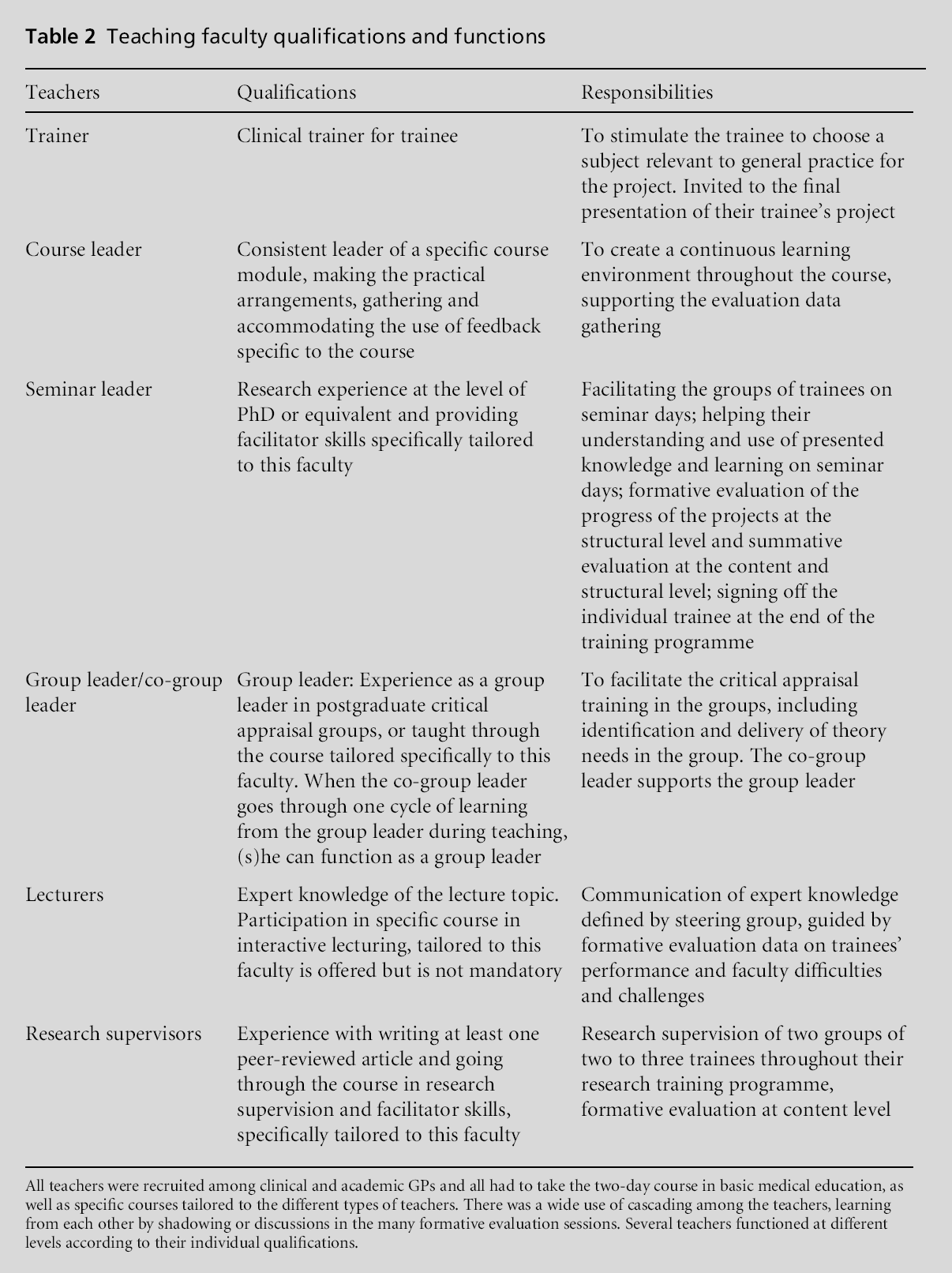
Itwas decided that six types of teacherswere needed to deliver the programme, with different types of skills and levels of responsibility (Table 2).
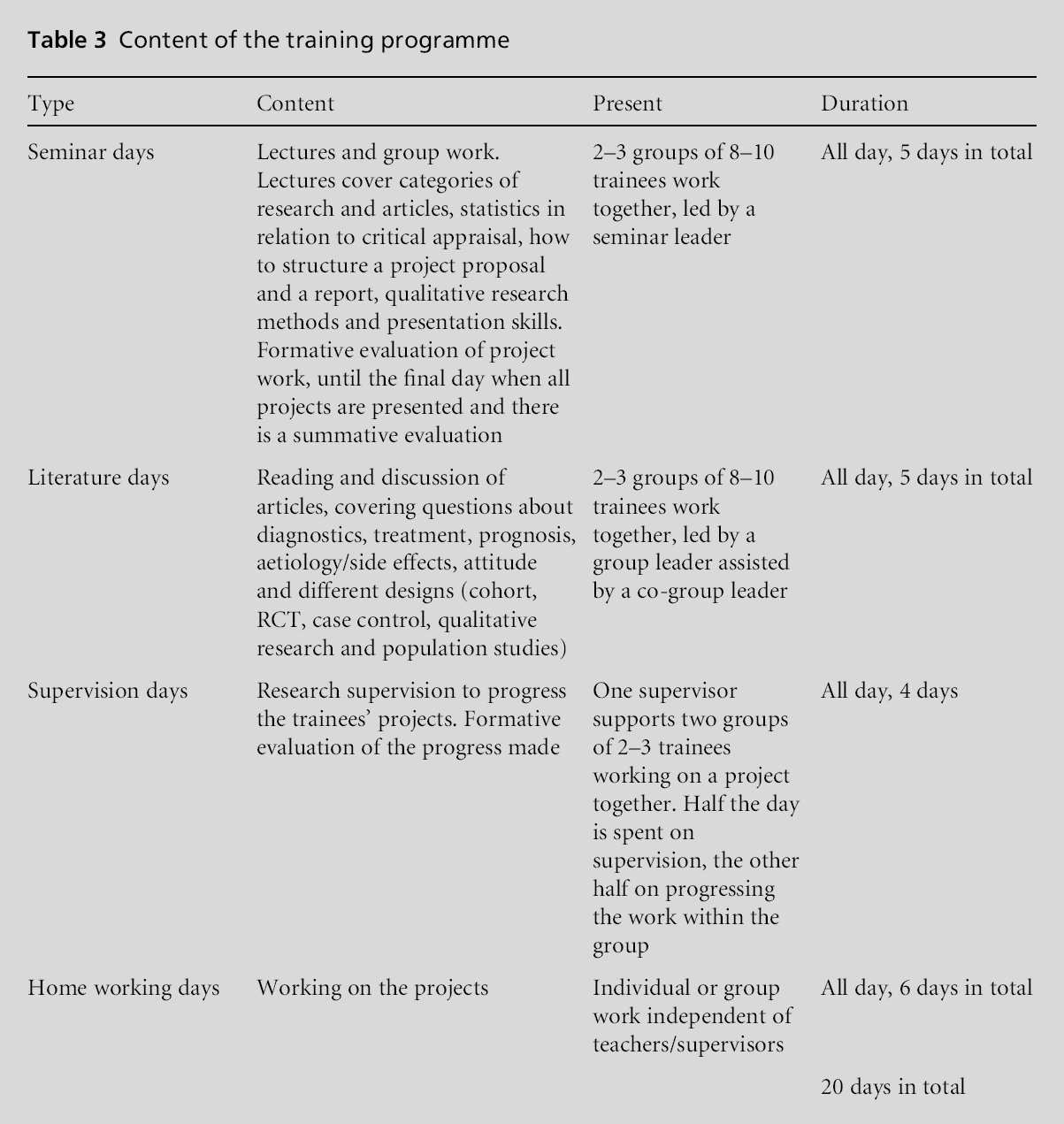
At all levels, the (future) teachers expressed a need for courses in which they could train skills in basic medical education as well as courses specifically aimed at their different tasks and roles. Based on feedback from the future teachers we provided tailored courses (Table 3).
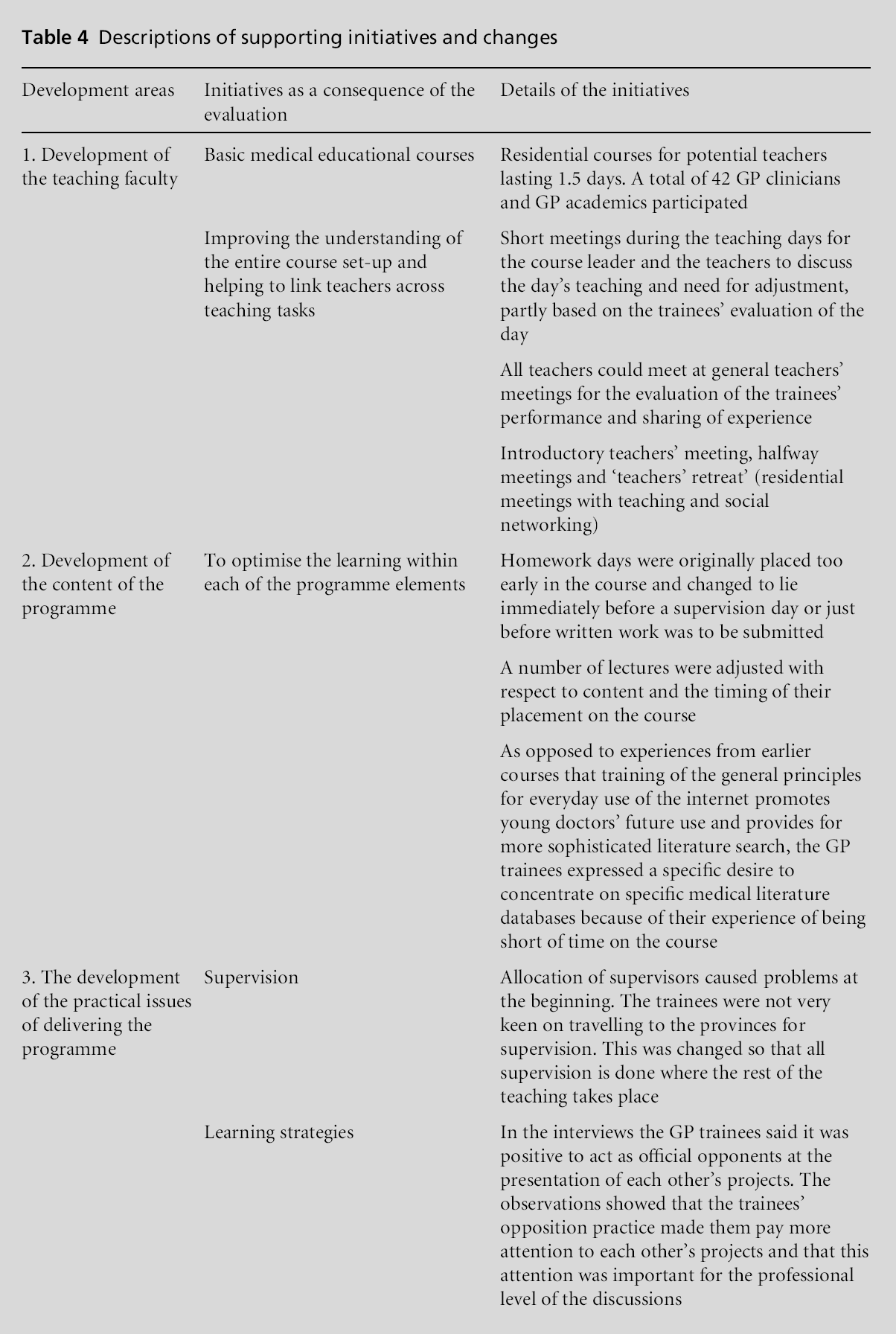
In August 2009, the teaching faculty consisted of 25 trained teachers, each undertaking at least one of the teaching roles. During development, the teachers increasingly articulated their joint ownership of the performance of, and adjustments to, the content and delivery of the training programme. For example, the teachers wished to start meetings for those teaching the same group of trainees; mentor–mentee relations among teachers; forming a group that would take over some of the steering group’s task of adjustment of the programme content. The faculty changes and the support initiatives are described in Table 4.
Development of the content of the training programme
The training programme was in accordance with the national regulatory body’s guidelines (Table 3). Two elements seemed to be of special importance for the success of the programme: the formative assessment and an emphasis on teaching trainees to assess their own and others’ work through constructive feedback, and the trainees acting as official opponents to their peers’ oral presentations.
In the written evaluations, most of the GP trainees stated that the trainingwas useful for their future work as GPs and they had achieved skills to answer daily clinical questions. Group work was very important in the programme, training the trainees in teamwork. Changes in the programme content are described in Table 4.
Delivering the research training to all GP trainees in the region
The RGP offered the programme to all GP trainees entitled to research training in the region. Fewer trainees than expected attended the courses (n = 95, as of August 2009) mainly because of maternity leave or sick leave.
The participant observations of the teaching sessions and the trainee interviews showed that trainees who were initially reluctant to participate became involved and acquired a positive attitude to research training. All data showed that the GP trainees took responsibility for their own learning early in the programme. This was also described in reports from GP trainees in the GP members’ magazine.[29]
Creating awareness, understanding and links between academic GPs, GP educators and GP clinicians
By August 2009, six trainees had returned to the RGP asking to do further research, one of them starting a PhD project.
As a result of the faculty development, the RGP now houses a large group of GPs and GP academics with a basic understanding of medical education achieved by participation in the educational courses for the teachers. In addition, at the summative assessment day, GP trainers attended to support their trainees in their presentations.
While the GP trainers fromoutside the RGP started to engage with the programme, interviews with the faculty showed that GP academics began to perceive the research training as competing with research production. The appreciation of the possible benefits of this programme changed into dissatisfaction, especially among those RGP academics who were not or only slightly involved.
Because of financial restraints in 2009, the process evaluation was replaced by a more conventional assessment aimed at monitoring general satisfaction. It is therefore not based on the same variety of evaluation sources, but to give perspective to the resultswe can add a few extra learning points based on the continuing delivery of the programme. Another 12 courses have been held and the teaching faculty now has 36 teachers. The number of different types of teachers involved created a demand for extensive coordination. Seminar leaders now also have the role of research supervisors, resulting in less demand for coordination. The faculty now comprises more experienced GP researchers than GP educators. Trainees still work on individual projects in groups, but not necessarily within the same theme, and there are now only two rather than three formative evaluations during the programme, reducing the resources needed for coordination.
Discussion
In this article, we describe the development of a GP research training programme, developing academic capacity in the community of GPs through a participatory action research process, developing a faculty and the programme content.
Our work was based on Stenhouse’s[22] classic description of the curriculum as a process rather than a static document; those who deliver the training must be involved in the continuous interpretation, and thus development of the training, in order to ensure the relevance for clinical GPs. Teaching is not just a pile of teaching materials and a long list of learning objectives; it is the translation of the idea underlying the training into a hypothesis that can be tested in practice. This invites critical testing and results in the teachers becoming researchers into their own processes and teaching. In this way, the teachers are supported in their professional development as teachers so that the complexity of learning and teaching is recognised. In order to do this, the teaching situation must accommodate individual learning needs. A high degree of self-monitoring among the teachers and learners is needed, together with room for a dialogue regarding the learning processes. If the teachers are to develop in this way, continuous work with their understanding and insight into the teaching situations is necessary. Organisation of the teaching should be done not only prior to the teaching and for the teachers, but also in the actual situations and in collaboration with the teachers.[17]
To pursue this educational ethos the research training had to be developed within the premises of action research; delivery of the programme could not be separated from the next step in the programme development, and those who created the learning situation – teachers and trainees – had to be involved in the development. The action research design was chosen not just to support the educational framework for teachers and students, but also because the foundation for learning of this nature implies continuous integration of experience.
After nine training courses, the teaching faculty was ready for participatory evaluation and development in its true form. According to these results, the project was a success. It is, however, important to note several points: the effect of the research training programme was mainly based on self reports and took place in a period when the research training was still new. A follow-up assessment on changed clinical behaviour was planned, but resources did not allow for this. The support needed for an action research project is always quite extensive, and we cannot judge the long-term effect of the initial three years of support, with a more conventional project following this period.
Educationally, practically and financially, we chose a solution that required a prioritised effort. One could call into question our continued focus on the development of the teaching faculty. Our basic idea for the strategy was to be able to professionally pass on something as basic as the management of knowledge within the profession. There is an acknowledgement of the inadequacy of what GPs master by virtue of their profession as clinicians[30] and what GP academics master by virtue of their research experience.[31] To deliver the training, the academics needed teaching skills and the GP trainers needed research skills.
With the project work, we achieved a development of awareness, understanding and linkage between the academic agenda and the clinical and training community outside the RGP. However, although the GP trainers from outside the RGP engaged with the programme, the GP academics working within the RGP saw this development as competing for their scarce time for research production.
In all research institutions there is always a demand for increased efficiency and an ever more specific research profile. As we see it, there is one challenge in particular that is significant for generic academic capacity building: the regulation of academia itself. Academic institutions are not measured on the longterm building of academic environments and capacity, but on their annual production of publications. A well-argued educational, theoretical set-up for general academic capacity building will always conflict with the academic agenda of knowledge production within a specific research profile. We tried to conform with this agenda by applying the action research design, but to succeed in this strategy, educational research has to play a prominent part in the research profile of the organisation delivering the programme.
In just three years, we showed that it was possible to overcome several of the previously reported obstacles in critical appraisal training of GP trainees, and the programme has now been implemented in the southern part of Sweden with a few adaptations to the local context. However, the study is also an important illustration of an inbuilt obstacle to any attempt to build bridges between the clinical world and academia.
We were fortunate to be allowed to run this process for almost three years.
With restrictions in budgets it is often difficult to maintain a long-term perspective. The changes to this programme after 2009 have directed the focus to research, and deviated from the original focus on educational support for the trainees, to set learning needs and to train team working skills to meet and resolve a collaborative challenge. Although not documented with evaluation data, there now seems to be a tendency for this programme to use the more traditional set up of research teachers for research training. This could be interpreted in at least two ways; (1) the strategy worked and there are now enough GP researchers to cover the teaching needs; or (2) the longer perspective with general academic capacity building for GP educators and clinicians needed too much support to continue with the resources available.
The addition of research impact and environment as part of the assessment of UK higher education institutions offers hope for the future perception of the need to develop academic capacity among clinicians and educators as we have described in this article (www.hefce.ac.uk/research/ref/ accessed 20 February 2012).
References
- Wilkinson D. Education and debate: ICRAM (The International Campaign to Revitalise Academic Medicine): agenda setting. BMJ 2004;329:787–9.
- Lionis C, Carelli F and Soler JK. Developing academic careers in family medicine within the Mediterranean setting. Family Practice 2004;21:477–8.
- del Mar C. Editorial. Is primary care research a lost cause? BMJ 2009;339:b4810 (and replies to this article).
- Holtedahl K. Research and practice combined – ideas for a life in general practice. Family Practice 2008;25:132–6.
- Del Mar C and Askew D. Building family/general practice research capacity. Annals of Family Medicine 2004 May;2(Suppl 2):35–40.
- Kohn R. Research in General Practice: bringing innovation into patient care. Workshop Report. The Academy of Medical Sciences, October 2009. www.acmedsci.ac.uk/ download.php?file=/images/publication/ 12569153801.pdf (accessed 2 July 2011).
- Laurence CO, Beilby JJ, Marley JE, Newbury J, WilkinsonDand Symon B. Establishing a practice based primary care research network. The University Family Practice Network in South Australia. Austrailan Family Physician. 2001;30(5):508–12.
- Dobbs F, Soler JK, Sandholzer H et al. The development of research capacity in Europe through research workshops – the EGPRN perspective. Family Practice 2009;1–4.
- The Royal College of General Practitioners. The RCGP Curriculum. London: RCGP. www.rcgp-curriculum. org.uk/extras/curriculum/index.aspx (accessed 2 July 2011).
- Siriwardena AN, Sandars J and Scott K. Attitudes of general practice trainers to teaching evidence-based medicine. Education for Primary Care 2004;15:611–17.
- Galloway R, Urquhart C and Evans R. Appraising evidence: the GP registrar perspective. Education for Primary Care 2004;15:64–72.
- Lehy N, Sheps J, Tracy CS, Nie JX, Moineddin R and Upshur REG. Family physicians’ attitudes toward education in research skills during residency. Canadian Family Physician 2008;54:413–14e.
- Bitsch-Christensen M. Flot international bedømmelse af forskningsenheden for almen medicin. Forskningen er relevant og formidlingen er i top. [Impressive international evaluation of the research unit for general practice. The research is relevant and the communication of it the best.] Ugeskr Læger 2003;165(18):1909.
- Ha?kansson A, Bengtsson K, Jørgensen AF and Hollnagel H. Forskningstræning for alle læger – ogsa? uden for universitetssygehusene. Evaluering af kursus i grundlæggende forskningsmetodologi. [Research training for all doctors – also outside university hospitals. Evaluation of course in basic research methodology.]Ugeskr Læger 2003;165(36):3423.
- Waldorff FB and Hermann C. Rationelle beslutninger for den travle praktiserende læge: effekt af kursus i internetbaserede søgninger. [Rational decisions for the busy GP: effect of a course in internet based literature searches.] Ugeskr Læger 2004;166(21):2054.
- Brockband A and McGill I. Facilitating Reflective Learning in Higher Education. Philadelphia: Society for Research into Higher Education & Open University Press, 1998.
- Elliot J. Reflecting Where the Action Is. London: Routledge, 2007.
- Jarvis P. Practised-based and problem-based learning. In: Jarvis P (ed) The Theory of Practice of Teaching. London: Kogan Page, 2002, pp. 123–31.
- Jarvis P. Towards a Comprehensive Theory of Human Learning, Lifelong Learning and the Learning Society, Vol 1. London: Routledge, 2006.
- Gipps CV. Beyond Testing, Towards a Theory of Educational Assessment. London: Falmer Press, 1994.
- Stenhouse L. Culture and Education. London: Nelson, 1967.
- Stenhouse L. An Introduction to Curriculum Research and Development (Open University set book). London: Heineman, 1975.
- Greene J. Evaluation, democracy, and social change. In: Shaw IF,Grene J and MarkMM(eds) The SAGEHandbook of Evaluation. London: SAGE, 2006, pp. 118–40.
- Cresswell JW. Educational Research (2e). Upper Saddle River, NJ: Pearson Education, 2005.
- Koshy V. Action Research for Improving Practice. A practical guide. London: Paul Chapman, 2005.
- Davies P, Necomer K and Soydan H. Government as structural context for evaluation. In: Shaw IF, Grene J and MarkMM(eds) The SAGE Handbook of Evaluation. London: SAGE, 2006, pp. 163–83.
- Brookfield SD. Understanding and Facilitating Adult Learning. Milton Keynes: Open University Press, 1986.
- Malterud K. Kvalitative metoder i medisinsk forskning: En innføring. Oslo: Universitetsforlaget, 2008.
- Hammerhøj L. Forskningstræning: Lærerigt udbytte i Region Øst [Research training: instructive outcome in Region East]. Practicus 2008;191(32):113.
- The General Medical Council. Good Medical Practice: teaching and training, appraising and assessing. www. gmc-uk.org/guidance/good_medical_practice/teaching_ training.asp (accessed 20 February 2012). The report can be downloaded at www.gmc-uk.org/publications/ standards_guidance_for_doctors.asp#gmp (accessed 20 February 2012).
- Dearing R. The National Committee of Inquiry into Higher Education, 1997. The report is available at www.leeds.ac.uk/educol/ncihe (accessed 2 July 2011).
Funding
The study was funded by The Danish Government, administered by the East Regional PostgraduateMedical Educational Board in Denmark and The Research Unit for General Practice in Copenhagen, University of Copenhagen, Denmark.
Peer Review
Not commissioned; externally peer reviewed.

