Keywords
complications; Pancreatitis, Chronic; Pancreatic Fistula
Abbreviations
CBD common bile duct; CT TAP CT toraco-abdominopelvic;
CXR chest x-ray; IPN infected pancreatic necrosis; PCF
pancreatico-colonic fistula; PD pancreatic duct; OTSC over the scope
clips; WON walled off necrosis
INTRODUCTION
Pancreatitis is an acute inflammatory process of
the pancreas with variable grades of severity [1]. It can
be severe and associated with local and/ or systemic
complications. Colonic complications are well known and
present in 1-3.3% of all patients with acute pancreatitis,
increasing to 15% in severe cases [2, 3], particularly in those
with necrotising pancreatitis or walled off necrosis (WON).
It is thought to occur as a consequence of pancreatic or
peripancreatic inflammation and infection and can also be
secondary to percutaneous drainage or surgical debridement
of pancreatic necrosis [4]. Typical clinical manifestations are
diarrhoea, hematochezia, and fever.
We present a case of an incidental diagnosis of a
pancreatico-colonic fistula (PCF) in a patient without
documented episodes of acute pancreatitis. The literature
on the topic was reviewed assessing presentation, diagnosis
and management. The aim of the study was to identify this
rare but potentially dreadful entity and if conservative
management can be possible in specific situations.
MATERIAL AND METHODS
A literature search was undertaken using PUBMED as
search engine including all papers published in English
until January 2019 and the references were cross-checked
for additional studies. The MESH headings used were
pancreatic fistula, colonic fistula, acute pancreatitis, colonic
complications. The target of the search was to identify
articles providing data on patients with acute, chronic or
acute on chronic pancreatitis who suffered as complication
PCF defined as clear communication from pancreatic duct
(PD) to colon visualised in computed tomography (CT),
CT with soluble contrast enema, ERCP or colonoscopy and
that reported type of management performed. Exclusion
criteria were defined as fistula aetiology unrelated with
pancreatitis, lack of appropriate imaging capable to clearly
define communication from PD to colon, fistula from colon to pancreatic abscess, infected pancreatic necrosis (IPN),
WON or pseudocyst, not specifically communicating with
pancreatic duct and articles in a different language than
English.
The PubMed search with the Mesh headings previously
stated provided 32 records and another 59 were obtained
by cross reference. No duplicate records were identified.
Articles were reviewed following the PRISMA guidelines.
91 records were screened by title and 29 were excluded
because were unrelated to the topic, not in English,
reporting fistula communicating pancreas to skin or
peritoneum, related to splenic artery pseudoaneurysm
or due to ingestion of corrosive. 62 full-text articles
were assessed for eligibility. 55 were excluded due to
no reported defined fistula from PD to colon (13 records
described fistula to pancreatic abscess/IPN/ WON, 10
records described fistula to pancreatic pseudocyst and in
32 records diagnostic image consisted only in plain film
abdominal X ray or the CT/ERCP/colonoscopy could not
clearly define communication from PD to colon). Finally,
7 papers were identified for full examination and analysis.
All of those were single case reports (Figure 1).
Figure 1: PRISMA flow diagram.
RESULTS
Case Report
We present a sixty-seven-year-old man with no known
previous medical history but a 60 pack year smoking
history and excess alcohol intake that presented to our
hospital with significant weight loss, non-productive cough,
short of breath and worsening of his basal status over the
last few weeks. There was no history of abdominal pain,
pancreatitis, diarrhoea or previous surgical interventions.
On admission, his chest x-ray (CXR) showed a suspicious
left upper lobe lesion with a left basal pleural effusion. A
computed tomography scan of the Chest, abdomen and
pelvis (CT TAP) showed a 4.2 cm enhancing mass in the left
upper lobe consistent with a primary lung neoplasm. There
was also extensive pancreatic parenchymal calcification
predominantly in the pancreatic head with ductal calculi
and pancreatic duct dilatation.
Three weeks after presentation he complained of right
sided abdominal pain. A clinical diagnosis of possible
biliary colic was made and a biliary ultrasound was
performed. This demonstrated a contracted thick walled
gallbladder. In addition, the pancreatic duct was again
noted to be dilated with a suggestion of an obstructing
pancreatic head mass (Figure 2a). To clarify those
findings a CT pancreatic protocol was performed which
showed extensive pancreatic parenchymal calcification
predominantly in the pancreatic head, with ductal calculi
and a pancreatic duct which was dilated measuring 1
cm maximal diameter. A focal pancreatic mass was not
identified. In the body and tail of the pancreas, there
was gas evident within the pancreatic duct itself and
also adjacent to the pancreatic duct in the tail. The gas
adjacent to the pancreatic tail tracked back towards the
distal transverse colon and there appeared to be a fistula to the lumen of the colon. In addition, there was a rimenhancing
fluid collection adjacent to the spleen which
measured 3.2 × 6.1 cm in maximal transverse diameter.
There was associated moderate left pleural effusion with
left lower lobe collapse and a small right pleural effusion.
Neither focal liver lesions nor biliary ductal dilatation was
seen. Gallstones were noted in the contracted gallbladder
(Figure 2b). A gastrografin enema was performed where
the pancreatic duct was seen to fill with contrast as the
contrast filled retrogradely through the transverse colon.
The fistula appeared to arise at approximately the level
of the splenic flexure (Figure 2c). Finally, a colonoscopy
ruled out any possible colonic neoplasm but failed to
identify the fistula orifice.
Figure 2: (a). US Pancreatic duct dilatation. (b). CT pancreas. The gas adjacent to the pancreatic tail tracks back towards the distal transverse colon and there appears to be a fistula to the lumen of the colon. (c). Gastrografin enema. The pancreatic duct was seen to fill with contrast as the contrast-filled retrogradely through the transverse colon. The fistula appears to arise at approximately the level of the splenic flexure.
No active cause for the PCF was demonstrated. There
was a long standing history of alcohol excess but no prior
hospital admissions with abdominal pain or pancreatitis.
Review of the Literature
Out of 91 records identified only 7 cases reported a
true PCF. Patients were predominantly male (7/8), with
a mean age of 60.4 years (range 42-78 years). A prior
history of alcohol abuse was present in all but one patient.
No comorbidities were stated. Presentation was chronic
pancreatitis in 3/8 cases, bowel obstruction in one case
and abdominal pain in 2 cases. Two of eight cases were
found incidentally on CT findings and one following a ERCP.
Two patients were diagnosed following a laparotomy for
pancreatitis. Our case was the only one that presented
without a prior history of pancreatitis, or prior surgery.
Aetiology was given as alcohol-induced pancreatitis in
seven cases and gallstone disease in one. In all cases, the
transverse or left colon was the area affected. Computed
tomography was the initial diagnostic test in 6/8 patients
and in 3/8 patients findings were confirmed with watersoluble
contrast enema. ERCP was the diagnostic tool in
more than half of the cases (5/8) and colonoscopy was
used as the main diagnostic or confirming test in 2/8 cases
(Table 1).
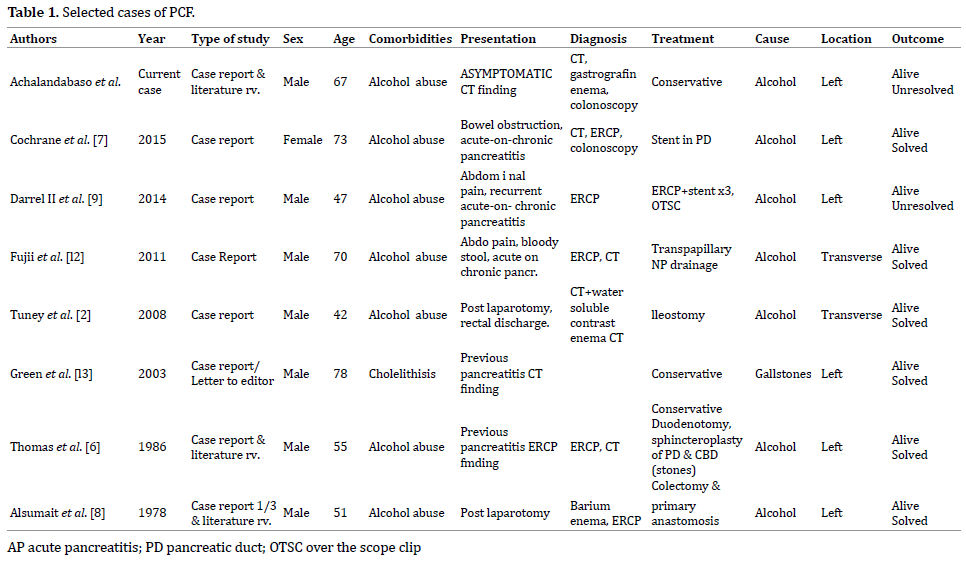
Patient details are as shown in Table 1. Treatment was
varied and heterogenous. Observation was adopted in 3/8
cases, endoscopic management (pancreatic duct stent,
over the scope clips-OTSC-, transpapillary nasopancreatic
drainage, hemoclippings and glue injection) in 3/8
and surgical resection in 2/8 cases. Duodenotomy,
sphincteroplasty of the pancreatic duct (PD) and common
bile duct (CBD) was performed in one case with gallstone
aetiology but no invasive treatment was directed to the
fistula, which healed with conservative management. Two
cases were diagnosed post-laparotomy. The first patients
presented with severe alcoholic pancreatitis, underwent
laparotomy for refractory sepsis, were a necrosectomy
was performed and colonic involvement at the descending
portion of the colon was discovered. Drainage and
ileostomy were carried out. Following the surgery
presence of persistent pancreatic juice discharge through
the anus led to suspect a PCF, that was confirmed by CT
with contrast enema, same technique after six months showed spontaneous closure, therefore, the ileostomy was
closed. The second patient presented after 2 years of the first
episode of severe acute pancreatitis with colonic resection
and primary anastomosis, with abdominal pain, fever and
diarrhoea and a barium enema revealed extravasation from
the colon to the stomach and an ERCP confirmed fistulous
tract beyond the pancreas that communicated with both the
stomach and the colon. Underwent relaparotomy with colonic
resection, primary anastomosis and pancreaticojejunostomy
and choledochojejunostomy.
Patients were successfully treated with resolving
fistula in follow up imaging in 6/8 cases, all patients being
alive at the time of the respective publications. In our case,
only observation was performed and although the fistula
is not resolved, the patient is still asymptomatic from the
abdominal point of view at 14 months of follow up.
DISCUSSION
Colonic complications associated with acute pancreatitis
are rare but carry an increased risk of mortality when delayed diagnosis and treatment. Incidence varies between
3.3% to 15% depending on the severity of pancreatitis as
described in Mohamed et al. [5]. PCF is most commonly
associated with walled-off pancreatic necrosis or abscess
formation and rarely forms spontaneously, it can also be
associated with pancreatic duct disruption. Percutaneous
interventional drainage of infected peri-pancreatic
collections as well as surgical procedures is associated
with an increased incidence.
Classic clinical manifestations for pancreatic colonic
fistula include diarrhoea, hematochezia, and fever. The
rapid disappearance of a previously noted abdominal mass,
especially if associated with gastrointestinal bleeding,
is very suggestive of the development of pancreatic duct
to colon fistula [6]. Hematochezia is the most common
clinical manifestation found in 60% of patients and is
associated with a mortality rate of 50-77% [4, 7]. Clinical
detection of colonic complications occurs relatively late in
the disease course as demonstrated in our series where
3 patients presented with acute on chronic pancreatitis
and 2 patients post laparotomy after former episodes of
pancreatitis.
Regarding diagnosis, there is variability among
modalities utilised. Computed tomography seems to be
the standard initial technique, it can show air fluid levels
in the pancreatic duct or directly visualize a fistula to
the colon with or without a classical cut-off sign that
has also been described in plain films [6]. A contrast
enema is an important study when consideration of
a colon abnormality arises in patients with known or
suspected pancreatitis. Some studies claim ERCP as the
gold standard to be done once PCF is suspected [2, 7]. The pancreatogram usually demonstrates tortuosity of the
pancreatic duct with extravasation of contrast from the
tail of the pancreas into the colon confirming a pancreatic
duct-colonic fistula. ERCP can also be therapeutic
when used to place a stent in the pancreatic duct or for
nasopancreatic drainage. Nevertheless, it is an invasive
technique that could be avoided with a water-soluble
enema, which can also be sensible and specific, being
less aggressive [2, 8]. Colonoscopy should be performed
to rule out underlying malignancies since both clinical
scenarios can have common symptoms. Despite all the
possible imaging techniques in some cases will only be
diagnosed intraoperatively. It is apparent that diagnosis
of this particular complication can be difficult, therefore,
a high index of suspicion must be maintained in patients
with severe acute pancreatitis with ongoing disease, in
particular, individuals with persistent sepsis, significant
diarrhoea or gastrointestinal haemorrhage.
Treatment in the acute/emergency situation has
traditionally been surgical or more lately interventional
radiology since patients may be haemodynamically
unstable [9]. In a retrospective study by Kochhar et al.
[10], the investigators found that all patients admitted to
their unit over a 4-year period with acute pancreatitis and
fistulisation to the colon underwent surgery. However,
this review suggests that in fact haemorrhage is an
infrequent presentation and surgery was seldom required.
Similar data has been reported by Ito et al. [3] where
conservative treatment has been shown to be successful
in selected patients. Successful non-surgical management
options have emerged in the last 20 years, with greater
utilization of percutaneous and endoscopic techniques.
Endoscopic options for PCF include ERCP with pancreatic sphincterotomy and pancreatic duct stenting, fibrin glue,
clips, nasopancreatic drainage or dual modality drainage
(percutaneous and endoscopic drainage simultaneously or
combined endoscopic and video-assisted retroperitoneal
pancreatic debridement). The treatment of large fistulas
may require the use of several different endoscopic tools
together.
The incidence of GI fistula is much higher in patients that
had a surgical intervention prior to being transferred to the
referral centre [11]. To an extent the site of fistula dictates
the management approach with small bowel fistulas
closing spontaneously whereas many colonic fistulas may
require active intervention such as percutaneous drainage,
endoscopic therapy or surgery (resection with or without
diversion). Although it has been shown that colonic fistulas
which became apparent after percutaneous pancreatic
drainage might close spontaneously [11]. The mortality
has been reported to be similar in patients with and
without GI fistula [4] although Jiang et al. reported higher
mortality in the subgroup of colonic fistula [11].
Our patient developed a PCF without the classical
history of prior pancreatitis. He was essentially
asymptomatic, required no intervention and remains
well on follow-up. Close surveillance is required as these
patients are at increased risk of developing exocrine and
endocrine insufficiency in the long term.
The authors recognise the limitations of this review.
This literature review identified a heterogeneous series
of retrospective case reports; the time frame between the
first and the last article is more than fifty years, with all the
developments and experience gained in the different fields
namely endoscopy, interventional radiology, surgery and
intensive care management occurring during that timeperiod.
Even though the cases reported were a small number
we feel that there is sufficient encouraging experience
with endoscopic and interventional radiology to consider
conservative management and avoid surgery in selected
patients as well as choosing a watch and wait approach, as
it may provide a survival benefit for patients that present
with a stable condition. Multidisciplinary decision and
treatment in high volume centres is mandatory.
CONCLUSION
PCF fistula can be a common observation in patients
with complicated acute pancreatitis being a rare
incidental finding in our patient since no episodes of
abdominal pain were reported and no infected pancreatic
collections or other complications were identified in the
imaging performed. Treatment can vary from a watch
and wait approach in asymptomatic cases, different
endoscopic techniques or surgical resection with or without anastomosis, mainly in symptomatic patients
with colonic haemorrhage. To our knowledge, this is the
first asymptomatic case of PCF described in the literature,
although other cases might have been misdiagnosed
in asymptomatic patients. It is infrequent since PCF’s
are generally symptomatic and associated with severe
necrotising pancreatitis.
Conflict of Interest
All authors are in agreement with the content of the
manuscript. There is no conflict of interest.
References
- Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, et al. Classification of acute pancreatitis - 2012: Revision of the Atlanta classification and definitions by international consensus. Gut 2013; 62:102–11. [PMID: 23100216]
- Tüney D, Altun E, Barlas A, Yegen C. Pancreatico-colonic fistula after acute necrotizing pancreatitis. Diagnosis with spiral CT using rectal water soluble contrast media. J Pancreas. 2008; 9:26–9. [PMID: 18182739]
- Ito K, Igarashi Y, Mimura T, Kishimoto Y, Kamata I, Kobayashi S, et al. Severe acute pancreatitis with complicating colonic fistula successfully closed using the over-the-scope clip system. Case Rep Gastroenterol 2013; 7:314–21. [PMID: 23904844]
- Tsiotos GG. Incidence and Management of Pancreatic and Enteric Fistulas after Surgical Management of Severe Necrotizing Pancreatitis. Arch Surg 1995; 130:48. [PMID: 7802576]
- Mohamed SR, Siriwardena AK. Understanding the colonic complications of pancreatitis. Pancreatology 2008; 8:153–8. [PMID: 18382101]
- Thomas CT, Hinton PJ, Thomas E. Spontaneus pancreatic duct colon fistula. J Clin Gastroenterol 1986; 8:69–73. [PMID: 3517133]
- Cochrane J, Schlepp G. Acute on chronic pancreatitis causing a highway to the colon with subsequent road closure: pancreatic colonic fistula presenting as a large bowel obstruction treated with pancreatic duct stenting. Case Rep Gastrointest Med 2015; 2015:794282. [PMID: 25893120]
- Alsumait AR, Jabbari M, Goresky CA. Pancreaticocolonic fistula: a complication of pancreatitis. Can Med Assoc J 1978; 119:715–9. [PMID: 709471]
- Gray DM 2nd, Mullady DK. Attempted Endoscopic Closure of a Pancreaticocolonic Fistula with an Over-The-Scope Clip. JOP J Pancreas 2014; 13:712–4. [PMID: 23183409]
- Kochhar R, Jain K, Gupta V, Singhal M. Fistulization in the GI tract in acute pancreatitis. Gastrointest 2012; 75:436–40. [PMID: 22154413]
- Jiang W, Tong Z, Yang D, Ke L, Shen X, Zhou J, et al. Gastrointestinal Fistulas in Acute Pancreatitis with Infected Pancreatic or Peripancreatic Necrosis. Medicine (Baltimore) 2016; 95:1–4. [PMID: 27057908]
- Fujii K, Suzuki K, Goto A, Nakahata K, Matsunaga Y, Wakasugi H, et al. Pancreatic-colonic fistula successfully treated with endoscopic transpapillary nasopancreatic drainage. Endoscopy 2011; 43(Suppl. 2):154–5. [PMID: 21563059]
- Green BT, Mitchell RM, Branch MS. Spontaneous Resolution of a Pancreatic – Colonic Fistula after Acute Pancreatitis. Am J Gastroenterol 2003; 98:2809–10. [PMID: 14687844]



