Keywords
Cholangiopancreatography, Magnetic Resonance; Cysts; Liver Transplantation; Pancreatic Cyst
Abbreviations IPMN: intraductal papillary mucinous neoplasia; MDCT: multi-detector-row computed tomography; OLT: orthotopic liver transplantation
INTRODUCTION
Improvement in technology and the ever-increasing application of diagnostic cross-sectional imaging have facilitated the detection of incidental pancreatic cysts in patients without symptoms referable to the pancreas [1]. Therefore, the prevalence of pancreatic cysts, traditionally considered to be low, ranges from 0.47 up to 36.7% in recent studies [2, 3, 4]. Because of the wide spectrum of underlying anatomic and pathologic features, as well as uncertainty concerning their biologic behavior, incidentally detected cysts are challenging to manage, and both surveillance and surgery have been proposed as alternative strategies in the general population [1, 4].Among imaging tools, magnetic resonance cholangiopancreatography (MRCP) is the most sensitive in assessing pancreatic fluid-filled structures, including the ductal system and/or cysts [5]. Nevertheless, to our knowledge, no studies using this technique have investigated the prevalence of incidental pancreatic cysts in post-solid transplantation patients who are at higher risk of developing malignancies as compared to general population, due to long-term immunosuppression [6]. Patients’ management after pancreatic cyst detection may be particularly challenging if the cysts are intraductal papillary mucinous neoplasias (IPMNs) [6]. This study was aimed at assessing the frequency of v
METHODS
Patient Population
By performing a computerized search, we identified all patients who underwent abdominal MRI at our institution over a 2-year period (July 2006 - July 2008). Of these patients, liver-transplanted patients whose examination included MRCP were enrolled. All cases had undergone MRCP for suspected biliary complications. The following exclusion criteria were established to assure that any cysts discovered were actually incidental findings: known and/or clinically suspected pancreatic disease of any nature, previous imaging demonstration of pancreatic cysts or abnormalities of any nature (including pancreatic calcifications at pre-orthotopic liver transplantation (OLT) routine computed-tomography), previous pancreatic surgery, pancreas transplantation, and known or suspected polycystic diseases involving the pancreas. We excluded patients with a history of preand/ or post-OLT acute pancreatitis or pre- and/or post- OLT symptoms of exocrine and/or endocrine impaired function referable to chronic pancreatitis, according to the current diagnostic standards, as previously stated [3], and as previously assessed by the transplantation selection-committee. Moreover, patients with MRCP abnormalities suggesting chronic pancreatitis and/or previous acute pancreatitis were excluded. Two patients were excluded due to the presence of pancreatic parenchymal atrophy in one and a single dilated secondary duct at the head in the other. Five patients were excluded from image analysis because of incomplete representation of the main pancreatic duct and/or low image quality due to motion or ascitesrelated artifacts. The final population included 47 subjects (38 male, 9 female; age range 39-70 years, mean age 59.3 years) who underwent OLT based on the following indications: HCV-related cirrhosis (n=16, with HIV coinfection in 1 case); HBV-related cirrhosis (n=2); alcoholic cirrhosis (n=13); hepatocellular carcinoma (n=13, associated with HCV infection in 6 cases, HBV infection in 2 cases, alcoholic cirrhosis in 4 cases, and cryptogenetic cirrhosis in 1 case); primitive sclerosing cholangitis (n=1); acute liver failure (n=1); and metastasis from intestinal carcinoid (n=1). The types of biliary anastomosis were choledochocholedochostomy in 40 subjects and Roux-en-Y choledochojejunostomy in 7 subjects. The time interval between OLT and MRCP ranged from 9 days to 125 months (mean 24.7 months). Fifteen patients underwent 1-3 additional MRCPs to monitor biliary findings over a 1-31 month follow-up period (median: 16.6 months). A total of 72 examinations were performed.
MR Imaging Technique
All examinations were performed using a 1.5 Tesla system (Siemens Avanto, Erlangen, Germany) equipped with a 6-element phased-array torso-coil. The pancreaticobiliary tract was imaged with the multislice technique, using two respiratory-triggered turbo spin echo (TSE) sequences with the following parameters: TR 1,700 ms, TE 654 ms, matrix 241x256, FOV 250x250, slices 60-80, thickness 1.5 mm, means 1, gap 0, nominal acquisition time 3 min 51 s, planes of acquisition coronal, and eventually axial (older sequence, used before 2007); TR 2,500 ms, TE 682 ms, matrix 357x384, FOV 380x380, slices 72-90, thickness 1 mm, thickness in z direction 1.1 mm, means 1, gap 0, parallel imaging acceleration factor 3, nominal acquisition time 3 min 51 s, plane of acquisition coronal (nearly isotropic sequence, used after 2007).
Image Analysis
Original data were loaded onto a dedicated workstation (Vitrea, Vital Images Inc., Minnetonka, MN, U.S.A.). MRCP source thin slices, multiplanar reformations and maximum intensity projection reconstructions, along with abdominal MR images were analyzed in consensus by two experienced abdominal radiologists (R.G., G.C.).
Simple pancreatic cysts were defined as cysts having a round or oval shape, sharp demarcation from the surrounding parenchyma, smooth thin walls, absence of lobules or septa and a homogeneous signal of simple fluid. An additional criterion for simple cysts was a diameter equal to or smaller than 20 mm. Bilobated cysts equal to or smaller than 20 mm were also considered as simple pancreatic cysts. All cysts not having the above criteria were defined as “complex”. A hyper-intense spot on MRCP images had to be at least 3 mm or more in each diameter, and be visible on both source and reformatted/maximum intensity projection reconstruction images to be defined as a cyst. On these bases, the following data were recorded for all cysts: number, dimensions (mm), location (head, body, tail), relationship to the main pancreatic duct (close vs. far from the duct, and communicating or noncommunicating), evolution in the subgroup of patients who underwent more than one MRCP (stable, decreased, increased in dimensions and/or number). For reporting purposes, the pancreatic head, body and tail, were defined as the portions of the gland: i) lying to the right of the superior mesenteric vein (including the uncinate process); ii) lying to the left of the superior mesenteric vein; iii) extending into the splenic hilum, respectively [3]. Cysts were defined as close to or far from the main pancreatic duct based on the distance measured on sagittal reformation reconstructions by the electronic caliper, i.e. less or more than 5 mm, respectively. Independently from distance, cysts were considered as communicating with the main pancreatic duct when a thin duct-like image was clearly visible on source images and at multiplanar reformations. Types of pancreaticobiliary junction were recorded and classified as “common”, if a unique channel was present at the vaterian complex, or “separate”, if a double channel was present, including cases of pancreas divisum or biliodigestive anastomoses. Cyst distribution and/or aspect was defined as “IPMN-like” in the case of: i) one single cyst ≥6 mm in diameter showing communication with the main pancreatic duct; ii) three or more cysts ≥ 3 mm in diameter, at least one communicating with the main pancreatic duct; iii) 4 or more cysts close to the main pancreatic duct (even with clear communication), at least one being 6 mm or larger in diameter. An IPMN-like pattern was defined as “branch-type” if involving secondary ducts or “mixed-type” if involving both secondary ducts and the main pancreatic duct [7]. Simple (or complex) cysts without a typical imaging pattern were classified as “indeterminate” [8].
Based on variations in number and dimensions, the cysts were defined as “stable” if no changes occurred, “increased” or “decreased” if at least one cyst was definitely new (or, alternatively, no longer visible) and/or the difference in the new diameter exceeded 20%.q
In addition, the presence of dilation of the main pancreatic duct (threshold 4 mm) or secondary ducts was recorded. Final diagnosis of biliary complications was obtained by reviewing the clinical histories and reports of interventional procedures of the livertransplanted patients.
ETHICS
Institutional review board approval was obtained for this retrospective study. Informed consent was obtained from the study participants. The study was performed in accordance with the Helsinki Declaration criteria.
STATISTICS
We calculated the prevalence of pancreatic cysts [9], together with the 95% confidence intervals (95% CI). The 95% confidence intervals were calculated according to the following equation:
P ± 1.96 √ (P (P-1)/N)
where P was the prevalence of cysts in our series, and N the number of liver-transplanted patients [9]. Univariate analysis using the Fisher exact test was carried out to verify the association between cysts, pre- OLT features (sex, age, etiology of cirrhosis and presence of hepatocarcinoma before OLT), and post- OLT features (presence of biliary complications, presence of lithiasic biliary complications, and time elapsed from OLT and baseline MRCP). For the analysis, the features were categorized as follows: male vs. female for sex, 61 years or older vs. 60 years or younger, infectious vs. non-infectious and alcoholic vs. non-alcoholic for the etiology of cirrhosis, lithiasic vs. non-lithiasic for the type of biliary complication, early vs. late if the baseline MRCP was performed earlier or later than 6 months from the OLT. The same analysis was performed depending on the presence of a common or separate channel between the choledochus and the main pancreatic duct in OLT-recipients, and on the presence or absence of additional pancreatic abnormalities as well (main pancreatic duct dilation and/or secondary duct dilation and/or parenchymal sign abnormalities). Based on the results of the univariate analysis, a multivariate analysis using multiple logistic regression (with the forward approach) was carried out including all features with a P<0.25 [10]. The Pearson chi-square test was used to analyze the pancreatic location of the cysts.
A P value less than 0.05 was considered statistically significant. Statistical analysis was carried out using commercially available software (MedCalc 9.2.0.1, Mariakerke, Belgium).
RESULTS
Cyst Prevalence, Distribution and Communication with the Main Pancreatic Duct
Ninety-five pancreatic cysts were found in 28/47 livertransplanted patients, corresponding to a prevalence of 59.6% (95% C.I. 43.0-76.0). The mean cyst diameter was 5.4 mm. Thirty-nine (41.0%) cysts were located in the head, 22 (23.1%) in the body and 34 (35.7%) in the tail of the pancreas. The number and dimensions of the cysts at the time of the baseline MRCP are reported according to pancreatic location, and relationship to and communication with the main pancreatic duct (Table 1) as well as distribution on a per-patient basis (Table 2).
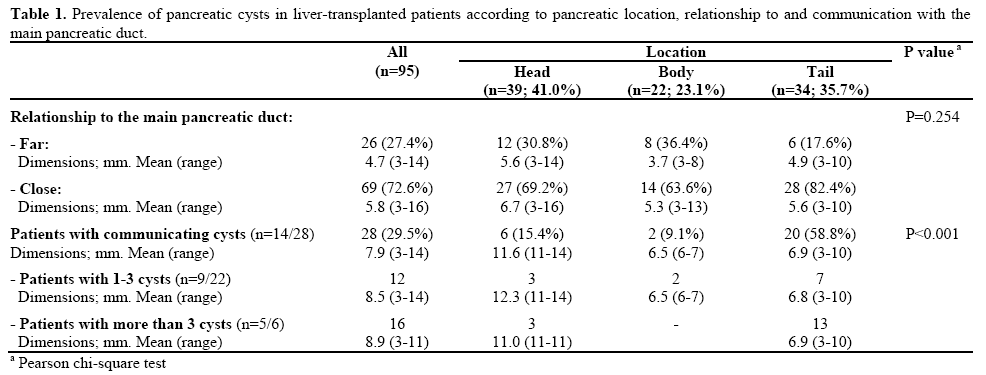

No lesions met the criteria for complex cysts (Figures 1 and 2). Communication with the main pancreatic duct was observed in 28 (29.5%) cysts in 14 (50.0%) livertransplanted patients (Figure 3). Cysts communicating with the main pancreatic duct were prevalently located in the tail of the pancreas (P<0.001; Table 1).
Figure 1. Incidental pancreatic cysts in liver-transplanted patients
undergoing MRCP for suspected biliary complications. Pancreatic
cysts were prevalently small and few on a per-patient basis, and
showed a simple appearance in all cases. a. Curve-reformatted
heavily T2w cholangiographic image in a liver-transplanted patient
with cholestatic liver disease shows a solitary, very small cyst (3
mm) at the body, far from the main pancreatic duct. Solitary cysts
were 21.4% of the total number of pancreatic cysts. b. Maximum
intensity projection reconstruction of the biliopancreatic tree of a
liver-transplanted patient with mild biliary anastomotic stricture.
Three 3-11 mm, paraductal non-communicating pancreatic cysts are
visible at the head and tail. Cysts were 2-3 per patient in 57.2% of
the liver-transplanted patients. All cysts in (a.) and (b.) were
classified as indeterminate in nature (see text for details).
Figure 2. Liver-transplanted patient showing ischemic damage of the
biliary tract with stenoses at the hepatic confluence and a distal
extrahepatic biliary duct. A biliary stent is present. a. A 12 mm large
pancreatic cyst is evident at the pancreatic neck, far from the main
pancreatic duct. b. Communication with the main pancreatic duct is
best appreciated on sagittal reformatted image. The cystic pattern
was classified as a branch-duct intraductal-papillary-mucinousneoplasia
(IPMN)-like type (see text for details).
Figure 3. Liver-transplanted patient with intrahepatic lithiasis and
extrahepatic biliary anastomotic stricture. Maximum intensity
projection reconstruction of the pancreaticobiliary tract shows
previously unknown multiple pancreatic cysts both far from and
close to the main pancreatic duct (see text for details), the largest
ones 10-11 mm in diameter. The cystic pattern was classified as a
branch-duct IPMN-like type (see text for details). Numerous cysts (5
to 14) occurred in a minority of liver-transplanted patients (n=6,
21.4%).
According to established criteria, of the 28 patients with cysts, 12 (42.9%) showed an IPMN-like pattern, of branch duct-type in 11 cases and mixed-type in 1 case. In fact, among 6 liver-transplanted patients with
more than 3 cysts, 5 patients had from 6 to 11 cysts, all being close to the main pancreatic duct and at least one communicating with it. Segmental slight dilation of the main pancreatic duct at the tail was present in one of these 5 patients (Figure 4). Moreover, among the 22 liver-transplanted patients with 1-3 cysts, 7 patients showed communication with large (9-12 mm) and/or multiple cysts. The remaining two patients showing communication with the main pancreatic duct (Table 1)
Figure 4. Liver-transplanted patient with suspected vanishing bile
duct syndrome. a. Maximum intensity projection reconstruction
shows the presence of pancreatic cysts communicating with the main
pancreatic duct at the pancreatic tail, the largest one of10 mm in
diameter. b. A focally, slightly dilated (4 mm) main pancreatic duct
is best appreciated on curved-reformation. Pancreatic abnormalities
were classified as a mixed-type IPMN-like pattern (see text for
details).
were not classified within IPMN-like lesions because they were single cysts with dimensions smaller than the established threshold of 6 mm in diameter. Nine of the 12 patients with an IPMN-like pattern of cysts (75.0%) underwent OLT due to alcohol-related cirrhosis. According to the established criteria, the other 16 patients (16/28, 57.1%) showed simple, indeterminate cysts.
Cyst Evolution Over Time
In 14/15 (93.3%) liver-transplanted patients, the cysts remained stable in number and dimensions at follow-up examinations. The only exception was one patient who showed an increase in cyst number (from 5 to 14) and dimensions (from 12 to 15 mm for the largest one) after 9 months (Figure 5). At endoscopic ultrasonography- guided biopsy, this patient was proven to have an IPMN. Histology was not available at the time of the study for the other patients with IPMN-like cyst pattern.
Figure 5. Multiple simple cysts in a liver-transplanted patient
investigated for suspected biliary stenosis (not confirmed).
Pancreatic cysts increased in number and dimensions between the
first MRCP (a.) and the follow-up examination at 9 months (b.). An
endoscopic ultrasonography-guided fine-needle biopsy of the largest
cyst demonstrated the presence of IPMN.
Features Associated with the Cysts
Pancreaticobiliary junction was found to be common in 24 of the 47 liver-transplanted patients (51.1%) and separate in 23 cases (48.9%) (including 5 pancreas divisum and 7 Roux-en-Y choledochojejunostomies). A final diagnosis of biliary complication was obtained in 37 of the 47 liver-transplanted patients (78.7%); 9 (24.3%) of these complications were lithiasic (19.1% in the overall population). Fifteen patients (15/47; 31.9%) showed MRCP pancreatic abnormalities (including pancreas divisum), as detailed in Table 3. In these patients: i) segmental dilation of the main pancreatic duct was minimal (up to 4 mm in diameter) and associated with an IPMN-like pattern in one case; ii) dilated secondary ducts were 2-3 in number, and associated with an IPMN-like pattern of co-existing cysts (Table 3). On these bases: i) none of the abnormalities were referable to chronic pancreatitis; ii) an IPMN-like pattern was present in one patient with pancreas divisum; iii) 7 out of 8 ductal abnormalities were referable to the co-existing IPMN-like pattern.

The results of the univariate analysis are shown in Table 4. Features associated with pancreatic cysts were alcoholic hepatic cirrhosis and the presence of hepatocellular carcinoma in the pre-transplantation period (P=0.005 and P=0.007, respectively), together with an MRCP finding of the aforementioned pancreatic abnormalities (P=0.012).
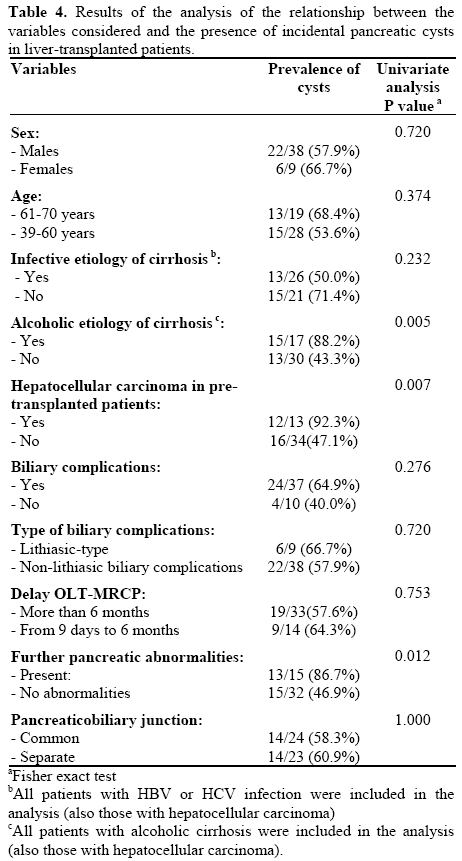
An alcoholic vs. non-alcoholic etiology of pre-OLT cirrhosis was the only variable significantly associated with the presence of cysts (P=0.006) at multivariate analysis. The Odds ratio for this feature corresponded to 9.81 (95% CI: 1.90-50.69).
DISCUSSION
Our results suggested that incidental pancreatic cysts are frequent in liver-transplanted patients, with a prevalence of 59.6%. This rate is notably higher than the range of 0.47-36.7% reported for the general population [2, 3, 4]. Interestingly, the prevalence of pancreatic cysts has been estimated in a recent series by means of an MRI single-shot fast spin-echo sequence [11], 16 slice-MDCT [3] or a combination of ultrasonography and not-otherwise specified CT [2], rather than using three-dimensional T2-weighted MRCP. To our knowledge, no data are currently available regarding the relative accuracy of the latest generation MRI and MDCT systems in detecting pancreatic cysts, especially the simple, small ones. Nevertheless, MRCP has been shown to be more accurate than MDCT in characterizing and classifying cystic tumors such as IPMNs [12]. Therefore, it might be argued that the high prevalence of pancreatic cysts found in liver-transplanted patients is due to the inherently superior contrast provided by heavily T2- weighted MRCP images for small pancreatic lesions showing a fluid signal. In fact, the majority of the pancreatic cysts in our series were small, with a mean diameter of 5.4 mm, and equal to or less than 3 in number in the majority of patients. Thus, our results might support the hypothesis that the frequency of incidental pancreatic cysts is actually higher than expected in the general population rather than in livertransplanted patients in particular, when the pancreas is imaged by MRCP.
Conversely, the high prevalence of pancreatic cysts might be a genuine characteristic of liver-transplanted patients, related to unsuspected pre- or post-OLT determining factors. Features found to be associated with the prevalence of pancreatic cysts (together with their aggressiveness or tendency to increase [2, 4]) are age or Asian race [3]. However, an age of greater than 60 years was not associated with pancreatic cysts in our study on a Caucasian population. Although univariate analysis showed a significant association between cysts and the presence of hepatocarcinoma in the pre-OLT period, and of further ductal or parenchymal pancreatic abnormalities, these were not confirmed at multivariate analysis. In addition, no correlation was found with sex, coexistence of biliary complications, or conditions, such as the presence of biliary stones and type of pancreaticobiliary junction, as potential causes of raised intraductal pressure in the main pancreatic duct [13]. OLT associated with alcoholic cirrhosis was the only feature significantly associated with the presence of pancreatic cysts (P=0.006). Pancreatic alcoholrelated damage has been correlated with aggregates of an increased proteic component of pancreatic juice, triggering the formation of calculi and elevated pressure in the main pancreatic duct and, consequently, in the secondary ducts. Nevertheless, parenchymal fibrosis rather than cyst formation is associated with alcohol abuse [14]. A possible explanation of our results might be that, since there is no correlation between hepatic and pancreatic alcohol-induced damage, genetic factors have been advocated to contribute to the development of one or the other [14]. A predisposition to prevalent hepatic damage which led our patients to cirrhosis and OLT, and the interruption of alcohol assumption before OLT, might be related to a stage of pancreatic damage manifesting itself as obstruction of the secondary ducts with cyst formation rather than with more advanced pancreatic fibrosis. In this hypothetical mechanism, cysts could represent a subclinical marker of alcoholic pancreatic damage in patients without clinical and imaging signs of chronic pancreatitis. However, neither pancreatic cysts (IPMNlike or indeterminate) nor the additional pancreatic abnormalities found in 15 patients (including pancreas divisum, non-specific minimal dilation of the main pancreatic duct, and dilation of the secondary ducts in the IPMN-like context) are referable to MRCP findings of chronic pancreatitis as recently revised [15]. The absence of an association between the pancreatic cysts and the time interval from OLT could confirm the role of pre-OLT factors, such as the etiology of cirrhosis, as a potential explanation for the presence of pancreatic cysts, rather than the effect of post-OLT factors (e.g., including the effect of the immunosuppressive therapy).
Given the uncertainty in the knowledge of etiology, pathogenesis and biological behavior of asymptomatic pancreatic cysts [3], in particular the smallest ones, their management is challenging, and both a surgical approach and a long-term imaging follow-up have been advocated as the most appropriate strategies [1]. According to Fernandez-del Castillo et al. [4], although the risk of malignancy for asymptomatic incidental pancreatic cysts measuring 20 mm or smaller is 3.5% in patients referred for surgery, 46.4% of these lesions are premalignant. These data support previous findings that pancreatic cyst size does not enable the prediction of malignancy [16]. On the contrary, Handrich et al. [17] showed that, although 41% of simple, incidental pancreatic cysts 20 mm or smaller can increase in size to a mean of 26 mm at imaging follow-up, morbidity and mortality are extremely different. Moreover, almost all (35/36) the simple pancreatic cysts 30 mm or smaller found by Sahani et al. were benign [18]. Since the biologic behavior of pancreatic cysts is uncertain, the finding of pancreatic cysts is particularly challenging in the set of post-solid organ-transplanted patients who are at higher risk of malignancy due to long-term immunosuppression [6]. All pancreatic cysts in our liver-transplanted patient series were simple in appearance; the majority were few in number on a perpatient basis (1-3), small in size (up to 16 mm of diameter) and showed no interval changes in 14/15 cases at follow-up. Nonetheless, one liver-transplanted patient who showed an increase in cyst number and dimensions was proven to have an IPMN. Moreover, 42.9% of the liver-transplanted patients with cysts (12/28) showed only a few or multiple, relatively larger cysts along the main pancreatic duct, with at least one of them communicating with it, i.e., showing an IPMNlike pattern (of branch-duct-type in 11 cases, and mixed-type in 1 case, respectively). We have no explanation for such a high prevalence of potentially aggressive lesions in our series, and whether it could be an effect of alcohol-induced damage (9/12 patients had pre-OLT alcoholic cirrhosis) rather than an underlying actual IPMN. To our knowledge, no data have been reported in the literature regarding a higher prevalence of IPMNs (or additional cystic tumors of the pancreas) in patients with alcohol-related hepatic cirrhosis or in liver-transplanted patients in particular as compared to the general population. Therefore, the majority of such lesions remained stable during the follow-up period.
As any retrospective study, ours has some limitations, in particular the lack of a systematic follow-up and definite characterization of the pancreatic cysts. Nevertheless, it has recently been shown that branchduct- type IPMNs in solid organ transplant recipients, including liver-transplanted patients, remain stable over a short-term follow-up [6]. Moreover, in a context of uncertainty, such as that of pancreatic cysts, information regarding their evolution, even for livertransplanted patients, is likely arguable from the aforementioned data [2, 4, 16, 17, 18]. On the other hand, extensive surgery for pancreatic cysts in livertransplanted patients is impracticable and unethical. Echoendoscopic and/or histological correlations for pancreatic cysts are available only for the patient with proven IPMN. Additional cases have been classified as IMPN-like lesions and indeterminate cysts. Our patients did not routinely undergo echoendoscopy after MRCP for the following reasons: i) they suffered from biliary complications, which represented the main clinical issue, and a source of invasive procedures of direct cholangiography; ii) it was considered unethical to have them undergo additional invasive diagnostic procedures since the majority of liver-transplanted patients showed few and very small cysts with a probably low risk of malignancy, and MRCP was available as a follow-up tool. Not all liver-transplanted patients in our institution undergo MRCP; this might lead to a selection bias with under- or over-estimation of pancreatic cyst prevalence, and contribute uncertainty of association with pre- and post-OLT features. Moreover, it is questionable whether larger pancreatic cysts were not evident or were simply overlooked at the pre-OLT imaging screening, which includes a MDCT in our institutional protocol. Unfortunately, not all MDCTs were available for a reevaluationat the time of the study, mainly because some were performed in other centers. In any case, all reports excluded any pancreatic abnormality, including parenchymal calcifications. Finally, a potential selection bias could be represented by the enrollment of patients with mild clinically-overlooked pancreatitis. Nevertheless, since no clinical and imaging signs of pancreatitis were observed during the pre-transplant work-up and at MRCP, the inclusion of such patients would contribute to supporting our hypothesis that the cysts may represent early, subclinical ductal damage from alcohol rather than representing a bias.
Further studies using MRCP are required to confirm our clinical observations and to define how to manage liver-transplanted patients with an incidental finding of pancreatic cysts, given the potential risk of malignant transformation due to immunosuppressive therapy. Moreover, a matter for debate might be whether MRCP is cost-effective as an adjunctive tool in the state-ofthe- art evaluation of patients in the pre-transplant period and what value should be attributed to incidental pancreatic cysts. As a consequence, the etiology of pancreatic cysts in liver-transplanted patients (and solid organ-transplanted subjects in general) needs to be further elucidated.
In conclusion, small, simple pancreatic cysts are a frequent incidental finding in liver-transplanted patients evaluated with MRCP and are likely to be associated with the alcoholic etiology of cirrhosis. Cysts are mostly small in number and size, and do not show a tendency to evolution. The IPMN-like pattern found in 42.9% of patients with cysts emphasizes the question of how to manage pancreatic cysts in the preand post-OLT period.
Conflict of interest The authors have no potential conflicts of interest
References
- Katz MHG, Mortenson MM, Wang H, Hwang R, Tamm EP, Staerkel G, et al. Diagnosis and management of cystic neoplasms of the pancreas. J Am Coll Surg 2008;207:106-120. [PMID 18589369]
- Lee SH, Shin CM, Park JK, Woo SM, Yoo JW, Ryu JK, et al. Outcomes of cystic lesions in the pancreas after extended follow-up. Dig Dis Sci 2007;52:2653-2659. [PMID 17404855]
- Laffan TA, Horton KM, Klein AP, Berlanstein B, Siegelmn SS, Kawamoto S, et al. Prevalence of unsuspected pancreatic cysts on MDCT. AJR 2008;191:802-807. [PMID 18716113]
- Fernandez-del Castillo C, Targarona J, Thayer SP, RattnerDw, Brugge WR, Warshaw AL. Incidental pancreatic cysts: clinicopathologic characteristics and comparison with symptomatic patients. Arch Surg 2003; 138:427-43. [PMID 12686529]
- Fulcher AS, Turner MA. MR. Pancreatography: a useful tool for evaluating pancreatic disorders. Radio Graphics 1999;19:5-24. [PMID 9925389]
- Gill KR, Pelaez-Luna M, Keaveny A, Woodward TA, Wallace MB, Chari ST, et al. Branch duct intraductal papillary mucinous neoplasm of the pancreas in solid organ transplant recipients. Am J Gastroenterol 2009;104:1256-1261. [PMID 19352341]
- Procacci C, Megobow AJ, Carbognin G, Guarise A, Spoto E, Biasutti G, Pistolesi GF. Intraductal papillary mucinous tumor of the pancreas: a pictorial essay. Radio Graphics 1999;19:1447-1463. [PMID 10555668]
- Walsh RM, Vogt DP, Henderson JM, Zuccaro G, Vargo J, Dumot J, et al. Natural history of indeterminate pancreatic cysts. Surgery 2005;138:665-671. [PMID 16269295]
- Shuman WP. Incidence and prevalence: proper use. AJR 1985;145:649-650. [PMID 3875267]
- Katz MH. Multivariable Analysis. Cambridge: Cambridhe University Press, 2008 (3rd edition).
- Zhang XM, Mitchell DG, Dohke M, Holland GA, Parker L. Pancreatic cysts: depiction on Single-shot Fast Spin Echo MR Images. Radiology 2002;223:547-553. [PMID 1997566]
- Waters JA, Schmidt CM, Pinchot JW, White PB, Cummings OW, Pitt HA, et al. CT vs MRCP: optimal classification of IPMN type and extent. J Gastrointest Surg 2008;12:101-109. [PMID 17917784]
- Wang HP, Wu Ms, Lin CC, Chank LY, Kao AW, wang HH, et al. Pancreaticobiliary diseases associated with anomalous pancreaticobiliary ductal union. Gastrointest Endosc 1998;48:184- 189. [PMID 9717785]
- Pandol SJ, Raraty M. Pathobiology of alcoholic pancreatitis. Pancreatology 2007;7:105-114. [PMID 17592222]
- Cereser L, Bali MA, Delhaye M, Matos C. Chronic pancreatitis. The role of MR Imaging. In: Balthazar EJ, Megibow AJ, PozziMucelli R (eds.) Imaging of the Pancreas. Berlin Heidelberg: Springer-Verlag, 2009 (1st edition): 183-207.
- Spinelli KS, Fromwiller TE, Daniel RA, et al. Cystic pancreatic neoplasms : observe or operate. Ann Surg 2004;239:651-659. [PMID 15082969]
- Handric SJ, Hough DM, Fletcher JG, Sarr MG. The natural history of the incidentally discovered small simple pancreatic cyst: long-term follow-up and clinical implications. AJR 2005;184:20-23. [PMID 15615944]
- Sahani DV, Saokar A, Hahn PF, et al. Pancreatic cysts 3 cm or smaller: how aggressive should treatment be? Radiology 2006;238:912-919. [PMID 16439566]






