Keywords
Neoplasms; Pancreatitis; Steroids; therapy
Abbreviations
AIP autoimmune pancreatitis; CT computed
tomography; DM diabetes mellitus; ICDC International Consensus
Diagnostic Criteria
INTRODUCTION
The concept of autoimmune pancreatitis (AIP) was first
proposed by Yoshida et al. [1] in 1995 as a specific from
of chronic pancreatitis that responds to corticosteroid
treatment. Clinically, AIP is characterized by diffuse
pancreatic enlargement and narrowing of the main
pancreatic duct. Hamano et al. [2] discovered elevated
serum IgG4 levels in AIP patients, and the serum IgG4 levels
were sensitive biomarkers of AIP. AIP is classified into 2
types based on its pathological features [3]. Type 1 AIP
is characterized by IgG4-positive plasma cell infiltration
around the pancreatic duct, obliterative phlebitis, and
storiform fibrosis, and type 2 AIP is characterized by
granulocytic epithelial lesions (GELs). IgG4-positive
plasma cells are not found in type 2 AIP. Extrapancreatic
lesions, including sclerosing cholangitis, retroperitoneal The short-term prognosis of type 1 AIP is improved
by steroid therapy, and since steroid withdrawal results
in AIP relapse [5], in Japan AIP patients receive long-term
steroid therapy. In other countries, however, AIP patients
have also been treated with immunosuppressant therapy
and anti-CD20 antibody therapy [6]. While the long-term
prognosis of AIP remains unclear, the development of
various malignant neoplasms, including pancreatic cancer
[7, 8], colon cancer, gastric cancer [9, 10, 11, 12], and
lymphoma [13, 14, 15], has been reported in AIP patients
in several case studies and retrospective studies. Although
whether AIP is associated with a higher incidence of
malignant neoplasms is unknown [16, 17], Shiokawa et al. [18] reported finding that AIP patients are at high risk
of various cancers and suggested that they may develop a
paraneoplastic syndrome.
In this study, we retrospectively investigated the
relationship between type 1 AIP and the occurrence of
malignant neoplasms.
MATERIAL AND METHODS
Patients
This study was carried out in accordance with the
Declaration of Helsinki and was approved by the Institutional
Review Board of Tokyo Women’s Medical University. The cases of 78 patients who were diagnosed with type 1 AIP
based on the International Consensus Diagnostic Criteria
(ICDC) and Japan diagnostic criteria at Tokyo Women’s
Medical University Hospital during the period between April
2000 and February 2015 were retrospectively reviewed
to determine their incidence of malignant neoplasms and
to identify risk factors. They were followed up regularly,
including by performing a range of examinations and
collecting clinical data, including serum IgG4 levels and
serum tumor marker levels, and computed tomography (CT)
examinations. Malignant neoplasms were diagnosed based
on the clinical data and pathological evidence.
Malignant Neoplasms of the AIP Patients
We analyzed the characteristics of the AIP patients
with malignant neoplasms, including their age and sex,
and presence or absence of steroid therapy, diabetes
mellitus (DM), the time malignancies were detected, and
relapse of AIP after treating the malignancies. We also
investigated whether the time when the malignancies
were detected was associated with the type of malignancy,
serum IgG4 level, relapse of AIP, steroid therapy, family
history of malignancies, and diagnostic imaging findings
in the pancreas. Since steroid therapy and DM are known
risk factors for malignancy, we investigated whether total
steroid dose and the presence of DM were associated with
the development of malignancies in the AIP patients.
Statistical Analysis
Continuous data were analyzed for significant differences
by the χ2 test and Wilcoxon test, and Fisher’s exact test
was used for categorical data. The statistical analysis was
performed using the JMP version 12.0 software (SAS Institute
Inc., Cary, NC). All statistical tests were two-sided, and a p
value <0.05 was considered statistically significant.
RESULTS
Patient Characteristics
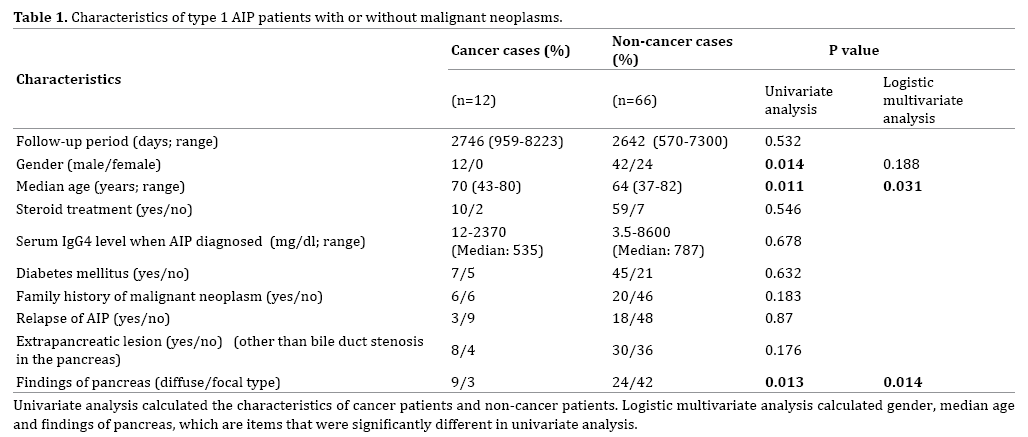
Twelve (15.4%) of the 78 type 1 AIP patients developed
a malignant neoplasm. Their follow-up periods after the diagnosis of type 1 AIP ranged from 959 to 8223 days (Table 1). Their median age was 70 years. Ten patients
had received steroid therapy when the malignancy
was detected. The median serum IgG4 level of the 12
patients at the time AIP was diagnosed was 535 mg/dl,
and the range was 12-2370 mg/dl. DM was present in 7
patients, and 6 patients had a family history of malignant
neoplasms. Eight patients had an extrapancreatic lesion
other than bile duct stenosis in the pancreas. The diffuse
type of pancreatic swelling was present in 9 cases, and the
focal type was present in 3 cases. There were significant
differences in gender, median age, and type of pancreatic
swelling between the group of AIP patients with malignant
neoplasms and the group without malignant neoplasms,
but there were no significant differences between the
group in whether they had received steroid therapy, had
DM, extrapancreatic lesions, a relapse of AIP, or a family
history of malignancies, or in their serum IgG4 levels.
The logistic multivariate analysis showed a significant
difference in type of pancreatic swelling (Table1).
The most common malignancy was colon cancer, which
was diagnosed in 5 cases (41.7%), and it was followed by lung
cancer, pancreatic cancer, and gastric cancer in 2 cases each
(16.7%), and hepatocellular cancer in 1 case (8.3%).
Time the Malignant Neoplasms Were Diagnosed in
Relation to the Time Type 1 AIP was Diagnosed
We investigated whether there were differences
between the group of patients with malignant neoplasms
that had been diagnosed within 1 year after the diagnosis
of AIP and the group of patients with malignant neoplasms
that had been diagnosed more than 1 year after the
diagnosis of AIP (Table 2). Twelve of the 78 AIP patients
had developed a malignancy. The malignancy had been
detected within a year after the diagnosis of AIP in 7 (9.0%)
of the 78 patients, and they accounted for 58.3% of the 12
AIP patients with a malignancy.

Five of the 78 AIP patients had been diagnosed with a
malignancy more than a year after the diagnosis of AIP, and another 5 patients had been diagnosed with a malignancy
before the diagnosis of AIP, and thus the 7 AIP patients
whose malignant neoplasms were detected within a year
after the diagnosis of AIP formed the largest group. We
compared the frequency of malignant neoplasms in both
the groups. There were 3 cases of colon cancer, and one
case each of lung cancer, pancreatic cancer, gastric cancer,
and hepatocellular cancer in patients whose malignant
neoplasms were detected more than a year after the
diagnosis of AIP. There were 2 cases of colon cancer and
1 case each of lung cancer, pancreatic cancer, and gastric
cancer in patients whose malignant neoplasms were
detected malignant neoplasms more than a year after the
diagnosis of AIP. The incidence of colon cancer among
the AIP patients was higher than the incidences of the
other cancers, and there were no statistically significant
differences between the both the groups with respected to
types of malignancies.
Treatment of the Malignant Neoplasms and Relapse of
AIP after Cancer Treatment
Ten of the 12 patients underwent surgery or endoscopic
mucosal resection (EMR) for a malignant neoplasm that
was detected after the diagnosis of AIP, and 2 of them had
pancreatic cancer. One of the 2 patients with pancreatic
cancer received adjuvant chemotherapy after surgery, and
the other patient underwent surgery alone. Five patients
had colon cancer, and one of them underwent EMR. We
discontinued steroid maintenance therapy in four of the
10 patients, but none of them experienced a postoperative
relapse. Because of their poor performance status the 2
lung cancer patients could not be treated surgically or by
chemotherapy.
Histological Findings and Stage of Malignant Neoplasms
Two of the 5 patients in the present study who
developed colon cancer had stage IIIA, and one each had
stage IIIB, stage I, and carcinoma in situ. One of 2 patients
with pancreatic cancer had stage I, and the other had stage
III. One of the 2 patients with gastric cancer had stage I.
The one patient with hepatocellular carcinoma had stage
III. Both patients with lung cancer had unresectable
advanced stage. The pancreatic cancer in both patients
was detected in the resectable stage. One pancreatic cancer
patient presented with stenosis of the pancreatic duct;
the preoperative pathological diagnosis was high-grade
dysplasia. Histological findings of the surgical specimen
revealed pancreatic cancer cells in the small part of main
pancreatic duct, with diffuse inflammatory IgG4-positive
plasma cells, lymphocytes infiltration, and obliterative
phlebitis in the pancreatic head. The other pancreatic cancer patient presented with atrophic pancreas and
infiltrated IgG4-positive plasma cells and lymphocytes
around the main pancreatic duct. Cancer cells were
detected in the pancreatic head, which metastasized to the
lymph nodes.
Total Steroid Dose and Duration of DM
The total steroid dose varied. Three of the 12 patients
who developed malignancies after the diagnosis of AIP
had not received steroid therapy, and the other 9 patients
(75%) had received total steroid doses of 2.9-15.9 g. Nine
of the 12 patents had received steroid therapy (Table 3),
and maintenance steroid therapy was continued in 8 of the
9 patients. To clarify the effect of steroid therapy on the
risk of malignancy, we compared the total steroid doses
of the group of AIP patients with a malignancy that had
been detected after the diagnosis of AIP and the group of
AIP patients in whom a malignancy had not been detected (Figure 1). The differences between the total steroid
doses of the two groups were not statistically significant,
suggesting that steroid therapy does not promote the
development of malignancy and is not a risk factor for
malignancy in AIP patients. Finally, we investigated the
association between the presence of DM and occurrence of
malignancies in AIP patients, but the results showed that
the presence of DM was not associated with an increase
the incidence of malignancy (Table 1).
Figure 1: Analysis of the relation between total steroid dose administered to AIP patients and the development of malignant neoplasms
DISCUSSION
Previous studies have reported malignancy prevalence
of 10.4%-18% in AIP patients [18, 19, 20, 21], a prevalence
range that was consistent with our own findings in the
present study, and the most frequent type of malignancy
in the AIP patients in the previous studies was colon
cancer, which was followed by lung cancer and then
gastric cancer. A recent multicenter international analysis
revealed that malignant neoplasms had been found in 57 of
978 type 1 AIP patients, and the most frequent malignancies
in descending order of incidence were gastric cancer, lung
cancer, prostate cancer, colon cancer, and pancreatic cancer
[17]. Earlier studies also reported higher incidences of gastric
cancer, lung cancer, and colon cancer than pancreatic cancer
in Japanese AIP patients [18, 20, 22, 23]. It seems that patients
who regularly attend a hospital clinic because of AIP are
more likely than healthy subjects to receive gastrointestinal
endoscopic examinations and that may have led to early
detection of their gastrointestinal cancers.
A malignant neoplasm was detected within a year after
the diagnosis of AIP in 9.0% of the 78 type 1 AIP patients in
the present study, and they accounted for 58.3% of the 12 AIP patients in whom a malignancy had been detected after
the diagnosis of AIP. The incidence of malignant neoplasms
tended to be higher within a year after the diagnosis of AIP,
and there were no AIP relapses after cancer treatment,
suggesting that the development of malignant neoplasms
among AIP patients is associated with the occurrence of
autoimmune disease.
While it is unclear why malignant neoplasms often
develop within a year after the diagnosis of AIP, there are
several hypotheses to explain the association between
malignancies and AIP. First, chronic inflammatory disease
causes malignancies such as colitic cancer in ulcerative colitis, hepatocellular carcinoma in hepatitis C, and
pancreatic cancer in chronic pancreatitis [24]. Kamisawa
et al. reported detecting more frequent K-ras mutations
in the gastric and colonic mucosae of AIP patients as well
as in their pancreatic epithelia [25, 26]. Mutationally
activated K-ras is the earliest genetic mutation in
precancerous lesions and has been found in more than
95% of pancreatic cancer patients and in 27% of chronic
pancreatitis patients. Based on these findings, oncogenic
K-ras mutations are thought to promote gastric and colon
cancer in AIP patients. While K-ras mutation is an early step
in the progression toward pancreatic cancer, the incidence of pancreatic cancer was lower than the incidences of other
gastrointestinal cancers in the present study as well as in
previous studies [18, 19, 20, 23]. Pancreatic intraepithelial
neoplasia (PanIN) is recognized as the precursor lesion of
invasive pancreatic cancer, and activated K-ras mutations
are almost always present in the early stage of PanIN.
Gapta et al. have reported detecting PanIN and PanIN
2 in 82% and 25%, respectively, of AIP cases [27]. Their
reports support the hypothesis that AIP is associated with
an increased risk of malignancy. Pancreatic cancer was
diagnosed in 2 of the 78 AIP patients in our study. One of
the 2 patients with pancreatic cancer had both a history of
three cancers in different organs before the diagnosis of
AIP, and a family history of pancreatic cancer, suggesting
that genetic factors play a major role in the development
of pancreatic cancer. The pancreatic cancer in the other
patient was diagnosed 9 years after the diagnosis of AIP,
and the patient had received steroid maintenance therapy
for 9 years because of repeated AIP relapses. Thus, K-ras
mutations and PanIN lesions are likely to be involved in
the progression of malignancies in patients with a longer
duration of AIP.
The second hypothesis to explain the development
of malignancies in AIP is the existence of an
immunosuppressed state induced by steroid therapy.
Long-term administration of immunosuppressive drugs
such as azathioprine has been reported to increase the risk
of carcinogenesis [28]. Although 10 of the 12 AIP patients
found malignant neoplasms within 1 year after diagnosis
of AIP in our study had received steroid therapy, two
patients who had not received steroid therapy after being
diagnosed with AIP developed malignancies. Although the
total steroid doses received by the group of AIP patients
with malignancies and the group of AIP patients without
malignancies were not significantly different according to
the results of a univariate analysis, there were significant
differences according to the results of a multivariate
analysis. Hirano et al. reported finding that univariate
analysis identified age at onset of IgG4-RD >65 years and
the presence of DM as significant risk factors for malignancy
in patients with IgG4-related disease, but that DM was
not found to be a significant risk factor in a multivariate
analysis [20]. Consistent with their results, the difference
between the incidences of malignancies in the group of AIP
patients with DM and the group of AIP patients without DM
in our own study was not statistically significant. A study
by Shimizu et al. found that 6 out of 9 patients developed a
malignancy after the diagnosis of AIP, but steroid therapy
was administered after development of the malignancy in
all 6 cases. These results suggest that steroid therapy itself
does not increase the risk of malignancies in AIP.
A third hypothesis to explain the development of
malignancies in AIP is that the immunological response
that the malignant neoplasm itself induces promotes the
infiltration by IgG4-positive plasma cells. Liu et al. reported
observing that IgG4-positive plasma cells had infiltrated
pancreatic cancer lesions and the surrounding area and that a high level of intratumoral IgG4-positive plasma
cell infiltration was correlated with a poor outcome [29].
Fukui et al. also found that IgG4-positive cells infiltrated
pancreatic cancer lesions, peritumoral pancreatitis lesions,
and obstructive pancreatitis lesions along with pancreatic
cancer and that the number of IgG4-positive cells or the
ratio of IgG4-positive cells to IgG-positive cells was higher
in the pancreas of AIP patients than of pancreatic cancer
patients [30]. They also found a significant correlation
between the numbers of regulatory T-cells (T-regs) and
IgG4-positive cells in obstructive pancreatitis lesions. A
similar immune mechanism appears to be involved in the
production of IgG4-positive cells in AIP and in obstructive
pancreatitis in pancreatic cancer. We therefore speculated
that the development of AIP within a year after the diagnosis
of malignancy is related to a cancer-associated immune
response and that the development of a malignancy several
years after the diagnosis of AIP is associated with chronic
inflammation and/or a genetic mutation.
Three of 5 colon cancers occurred within a year after
the diagnosis of AIP, and we thought that they are related
to the cancer-associated response. On the other hand, the
other two of 5 colon cancers occurred after 8 years and
20 years, and chronic inflammation was not found in their
surgical specimens. As the incidence of colon cancer was
generally high and colonoscopy was frequently performed
during screening, we suspect that the number of colon
cancer patients in our study was higher than that of patients
with our study types of cancer. While it is important to
clarify the immune mechanism of type 1 AIP regarding
the development of colon cancer, the association between
immune mechanism in type 1 AIP and the incidence of
colon cancer in this study remain unclear.
In conclusion, although the mechanism underlying
the development of malignant neoplasms in AIP patients
has yet to be identified, the incidence of malignancies was
relatively high within a year after the diagnosis of AIP.
Because of the high incidence of malignant neoplasms in
AIP patients, it is recommended that male AIP patients
over 70 years old who have been diagnosed with AIP
within the previous year be examined for malignancy by
a combination of gastrointestinal endoscopy, either chest
X-ray or CT scan, and abdominal ultrasound.
Conflicts of Interest
The authors state that they have no conflicts of interest
(COI) to declare.
References
- Yoshida K, Toki F, Takeuchi T, Watanabe S, Shiratori K, Hayashi N. Chronic pancreatitis caused by an autoimmune abnormality. Proposal of the concept of autoimmune pancreatitis. Dig Dis Sci 1995; 40:1561-8. [PMID: 7628283].
- Hamano H, Kawa S, Hoshiuchi A, Unno H, Furuya N, Akamatsu T, el al. High serum IgG4 concentrations in patients with sclerosing pancreatitis. N Engl J Med 2001; 344:732-8. [PMID: 11236777].
- Shimosegawa T, Chari ST, Frulloni L, Kamisawa T, Kawa S, Mino-Kenudson M, et al. International consensus diagnostic criteria for autoimmune pancreatitis. Guideline of the International Association of Pancreatology. Pancreas 2011; 40:352-8. [PMID: 21412117].
- Hart PA, Kamisawa T, Brugge WR, Chung JB, Culver EL, Czako L, et al. Long-term outcomes of autoimmune pancreatitis: a multicenter, international analysis. Gut 2013; 62:1771-6. [PMID: 23232048].
- Hirano K, Tada M, Isayama H, Yagioka H, Sasaki T, Kogure H, et al. Long-term prognosis of autoimmune pancreatitis with and without corticosteroid treatment. Gut 2007; 56:1719-24. [PMID: 22249131].
- Hart PA, Topazian MD, Witzig TE, Clain JE, Gleeson FC, Klebig RR, et al. Treatment of relapsing autoimmune pancreatitis with immunomodulators and rituximab: The Mayo Clinic experience. Gut 2013; 62:1607-1615. [PMID: 22936672].
- Kamisawa T, Chen PY, Tu Y, Nakajima H, Egawa N, Tsuruta K, et al. Pancreatic cancer with a high serum IgG4 concentration. World J Gastroenterol 2006; 12:6225-8. [PMID: 17036401].
- Fukui T, Mitsuyama T, Takaoka M, Uchida K, Matsushita M, Okazaki K. Pancreatic cancer associated with autoimmune pancreatitis in remission. Intern Med 2008; 47:151-5. [PMID: 18239323].
- Kountouras J, Zavos C, Chatzopoulos D. Autoimmune pancreatitis, Helicobacter pylori infection, and apoptosis: a proposed relationship. Pancreas 2005; 30:192-3. [PMID: 15714146].
- Kountouras J, Zavos C, Chatzopoulos D. A concept on the role of Helicobacter pylori infection in autoimmune pancreatitis. J Cell Mol Med 2005; 9:196-207. [PMID: 15784177].
- Koizumi S, Kamisawa T, Kuruma S, Tabata T, Chiba K, Iwasaki S, et al. Immunoglobulin G4-related gastrointestinal disease, are they immunoglobulin G4-related diseases? World J Gastroenterol 2013; 19:5769-74. [PMID: 24124321].
- Li M, Zhou Q, Yang K, Brigstock DR, Zhang L, Xiu M, et al. Rare case of Helicobacter pylori-positive multiorgan IgG4-related disease and gastric cancer. World J Gastroenterol 2015; 21:3429-34. [PMID: 25805956].
- Masaki Y, Sugai S. Lymphoproliferative disorders in Sjögren’s syndrome. Autoimmune Rev 2004; 3:175-82. [PMID: 15110228].
- Uehara T, Ikeda S, Hamano H, Kawa S, Moteki H, Matsuda K, et al. A case of Mikulicz’s disease complicated by malignant lymphoma: a postmortem histopathological finding. Intern Med 2012; 51: 419-23. [PMID: 22333380].
- Kauppi M, Pukkala E, Isomaki H. Elevated incidence of hematologic malignancies in patients with Sjögren’s syndrome compared with patients with rheumatoid arthritis. Cancer Causes Control 1997; 8:201-4. [PMID: 9134244].
- Yamamoto M, Takahashi H, Shinomura Y. IgG4-related Disease and malignancy. Int Med 2012; 51:349-50. [PMID: 22333367].
- Hart PA, Law RJ, DierkhisingRA, Smyrk TC, Takahashi N, Chari ST. Risk of cancer in autoimmune pancreatitis: a case-control study and review of the literature. Pancreas 2014; 43:417-21. [PMID: 24622072].
- Shiokawa M, Kodama Y, Yoshimura K, Kawanami C, Mimura J, Yamashita Y, et al. Risk of cancer in patients with autoimmune pancreatitis. Am J Gastroenterol 2013; 108:610-7. [PMID: 23318486].
- Yamamoto M, Takahashi H, Tabeya T, Suzuki C, Naishiro Y, Ishigami K, et al. Risk of malignancies in IgG4-related disease. Mod Rheumatol 2012; 22:414-8. [PMID: 21894525].
- Hirano K, Tada M, Sasahira N, Isayama H, Mizuno S, Takagi K, et al. Incidence of malignancies in patients with IgG4-related disease. Intern Med 2014; 53:171-6. [PMID: 24492683].
- Shimizu S, Naito I, Nakazawa T, Hayashi K, Miyabe K, Kondo H, et al. Correlation between long-term outcome and steroid therapy in type 1 autoimmune pancreatitis: relapse, malignancy and side effect of steroid. Scand J Gastroenterol 2013; 42:506-10. [PMID: 26061806].
- Lowenfels AB, Maisonneuve P, Cavallini G, Ammann RW, Lankisch PG, Andersen JR, et al. Pancreatitis and the risk of pancreatic cancer. International Pancreatitis Study Group. N Engl J Med 1993; 328:1433-7. [PMID: 8479461].
- Nishino T, Toki F, Oyama H, Shimizu K, Shiratori K. Long-term outcome of autoimmune pancreatitis after oral prednisolone therapy. Intern Med 2006; 45:497-501. [PMID: 16702740].
- Ikeura T, Miyoshi H, Uchida K, Fukui T, Shimatani M, Fukui Y, et al. Relationship between autoimmune pancreatitis and pancreatic cancer: a single-center experience. Pancreatology 2014; 14:373–9. [PMID: 25278307].
- Kamisawa T, Horiguchi S, Hayashi Y, Yun X, Yamaguchi T, Tsuruta K, Sasaki T. K-ras mutation in the major duodenal papilla and gastric and colonic mucosa in patients with autoimmune pancreatitis. J Gastroenterol 2010; 45:771-8. [PMID: 20157749].
- Kamisawa T, Tsuruta K, Okumoto A, Horiguchi S, Hayashi Y, Yun X, et al. Frequent and significant K-ras mutation in the pancreas, the bile duct, and the gallbladder in autoimmune pancreatitis. Pancreas 2009; 38: 890-5. [PMID: 19752775].
- Gapta R, Khosroshahi A, Shinagare S, Femandez C, Ferrone C, Lauwers GY, et al. Does autoimmune pancreatitis increase the risk of pancreatic carcinoma? : a retrospective analysis of pancreatic resections. Pancreas 2013; 42:506-10. [PMID: 23271394].
- Axelrad JE, Lichtiger S, Yajnik V. Inflammatory bowel disease and cancer: The role of inflammation, immunosuppression, and cancer treatment. World J Gastroenterol 2016; 28:4794-801. [PMID: 27239106].
- Liu Q, Niu Z, Li Y, Wang M, Pan B, Lu Z, et al. Immunoglobulin G4 (IgG4)-positive plasma cell infiltration is associated with the clinicopathologic traits and prognosis of pancreatic cancer after curative resection. Cancer Immunol Immunother 2016; 65:931–40. [PMID: 27271551].
- Fukui Y, Uchida K, Sumimoto K, Kusuda T, Miyoshi H, Koyabu M, et al. The similarity of Type 1 autoimmune pancreatitis to pancreatic ductal adenocarcinoma with significant IgG4-positive plasma cell infiltration. J Gastroenterol 2013; 48:751-61. [PMID: 23053421].


