Keywords
etiology; Humans; Pancreas; Pancreatitis; Pancreatic
Neoplasms; pathophysiology; Pancreatic Diseases; Postoperative
Complications; secretion; physiology
Abbreviations
CP chronic pancreatitis, DM diabetes mellitus; DP distal
pancreatectomy
INTRODUCTION
The endocrine consequences of distal pancreatectomy
(DP) are an evolving phenomenon. The development of
de-novo DM is a well-documented complication of DP,
however, the incidence rate reported is highly variable,
ranging between 8% and 57%, depending on the length of
follow-up reported [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11]. Endocrine
dysfunction post-pancreatectomy may present as either
worsening of pre-existing, or development of de-novo
diabetes mellitus (DM). The American Diabetic Association
(ADA) refers to de-novo DM as pancreatogenic or type 3c
diabetes [1, 2].
Previous studies have hypothesized demographic
and operative risk factors such as gender, body mass
index (BMI), and volume of resected pancreas; however,
the results have been inconsistent [9, 12, 13, 14]. The
understanding of de-novo DM after DP along with the
associated perioperative risk factors is imperative, bearing
in mind the substantial morbidity associated with DM,
which is the seventh leading cause of death in the United
States, and those with diabetes have double the overall
risk of death than those without [1].
The aim of this study was to approach the question
of the relationship between the volume of pancreas
resected and the incidence of new onset DM utilizing
precise pathological specimens instead of radiological
measurements as performed in all prior studies. The
secondary goals of this study were to identify significant
baseline comorbidities associated with de-novo DM, and
furthermore to examine the effect of patient demographics
and the etiology of pancreatic disease on the incidence of
de-novo DM following DP.
PATIENTS AND METHODS
The subjects of this study were identified from a
prospectively-maintained, pancreatectomy database. The
database contains details of all adult patients (≥18 years of
age) who have undergone elective pancreatectomy at our
institution, and for the purposes of this study, the period
2005 through 2015 was chosen for analysis. We only
included patients who underwent a distal pancreatectomy
± splenectomy for a pancreatic pathology. We excluded
all patients who had a concomitant resection of other organs, and as such patients undergoing DP as part of
a gastrectomy or during resection of a retroperitoneal
sarcoma were excluded. All patients who met the inclusion
criteria regardless of their preoperative diabetic status
where included, patients without a preoperative diagnosis
of diabetes where analyzed as a subgroup.
The patient’s demographic data (gender, age, race,
body mass index [BMI]) at the time of operation were
documented as was any history of pancreatitis, exocrine
pancreas insufficiency (EPI), or prior diagnosis of DM.
EPI was defined as the primary or secondary disturbance
of the exocrine pancreatic function leading to maldigestion,
numerous invasive and noninvasive diagnostic tests are
performed [15]. All patients who utilized pancreatic enzyme
replacement therapy where identified as having EPI.
The patients BMI was calculated from weight and
height measurements performed at the time of hospital
admission prior to surgery.
The histopathological diagnosis was extracted from the
final pathology report. The volume of resected pancreas
was calculated by physician investigators using the three
dimensions reported by anatomical pathologists in their
report template. The resected pancreas volume was
reported in cubic centimeters (cm3).
All available peri-operative random plasma glucose
levels were recorded and analyzed. Patients with
preoperative impaired glycemic control or DM were
identified. Among the patients with normal preoperative
plasma glucose levels we analyzed the postoperative
levels and stratified them by development of de-novo DM
postoperatively; i.e. “de-novo DM” and “no de-novo DM”.
The American Diabetic Association (ADA) guidelines
were used to diagnose patients with DM namely: random
plasma glucose levels of ≥200 mg/dL (11.1 mmol/L) or
post hospital hemoglobin A1C ≥6.5% (48 mmol/mol)
[2]. Plasma glucose levels used for diagnosis of de-novo
DM excluded any measurements taken after 72 hours
post-operatively to account for physiological stress
hyperglycemia secondary to inflammation [16]. If patients
were on intravenous fluids at this stage, or were on enteral
or parenteral nutrition then the glucose level used to confir
a diagnosis of DM was delayed until the patient was on an
oral diet.
Categorical and continuous variables were reported
as frequencies (n, %) and median (interquartile range),
respectively. Due to the skewness of the variables’
distribution we used Wilcoxon rank-sum tests and
Kruskal-Wallis equality-of-populations tests to examine
the significance of differences in patients who developed
de-novo DM and who did not. Bivariate linear regression
models were fit to examine the contribution of factors
found to be significant (P<0.2) in the respective univariate
analyses performed. A P<0.05 indicated the presence of
a statistically significant association. All analyses were
performed using IBM SPSS Statistics for Windows, Version
24 (IBM Corp., Armonk, NY., USA)
RESULTS
We identified a total of 327 patients who underwent
DP between 2005 and 2015. We included 317 patients
after applying the inclusion and exclusion criteria. There
was a female predominance (n=188, 59.3%) in the study
population with a median age of 62 (Interquartile Range
[IQR] = 50.23 - 68.8) years. The median body mass index
was 27 (IQR = 24 - 31) Kg/m2.
The most common final pathological diagnoses
were: pancreatic ductal adenocarcinoma [PDAC] (n=79,
24.9%); pancreatic neuroendocrine tumor (n=72, 22.7%);
intraductal papillary mucinous neoplasm [IPMN] (n=57,
18%); chronic pancreatitis [CP] (n=52, 16.4%); and
mucinous cystic neoplasm [MCN] (n=36, 11.4%) (Table
1). The median volume of tissue excised during DP was
92.9 cm3 (IQR = 51.9 – 157.7).
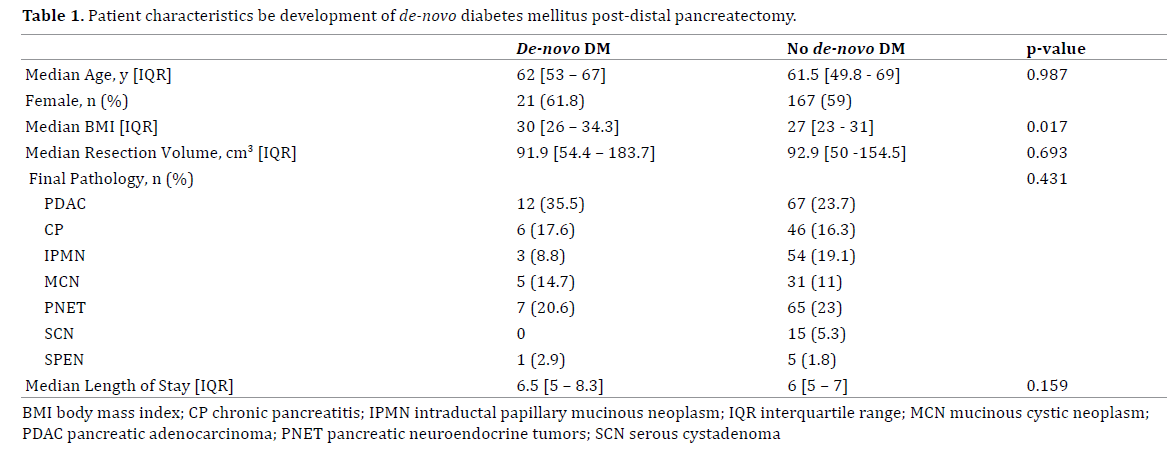
Assessing the incidence of De-novo DM by pathology,
we noted that it was highest in patients with pancreatic
ductal adenocarcinoma (n=12, 35.3%) followed by
pancreatic neuroendocrine tumors (n=7, 20.6%), chronic
pancreatitis (n=6, 17.6%) and mucinous cystic neoplasm
(n=5, 14.7%) while none of the patients with serous cyst
adenoma developed de-novo DM. Development of de-novo
DM was independent of the histopathology of the pancreas
resected (P>0.05).
Assessment of the correlation between the volume of
pancreas resected and de-novo DM did not demonstrate
an increased risk for the development of this complication
as although patients with de-novo diabetes were noted
to have larger volume resections than those who did not
develop new diabetes, the difference was not statistically
significant (P=0.693).
Neither gender nor age appeared to influence patients’
risk of developing DM post-operatively. The median BMI
of patients who developed de-novo DM post was however
significantly greater than those who did not (30 Kg/m2
versus 27 Kg/m2; P=0.017).
DISCUSSION
Understanding the true incidence and risk factors for
the development of diabetes in the post-operative period
should lead to better and more predictable outcomes for
patients undergoing distal pancreatectomy. Being able
to accurately counsel patients regarding potential postoperative
challenges is increasingly important as the
number of pancreatic resections performed annually in
the USA exceeds 10,000 cases [17]. Postoperative diabetes
was found to have the largest negative impact on leisure
and physical activities during a study examining quality of
life after partial pancreatic resection [18].
The primary finding of the study was the identification
of a significant incidence of post-operative de-novo DM in
our study population at 14.7%. This result is lower than
the systematic review of 1,731 patients by De Bruijin et al.
which reported an incidence of 39% in patients undergoing
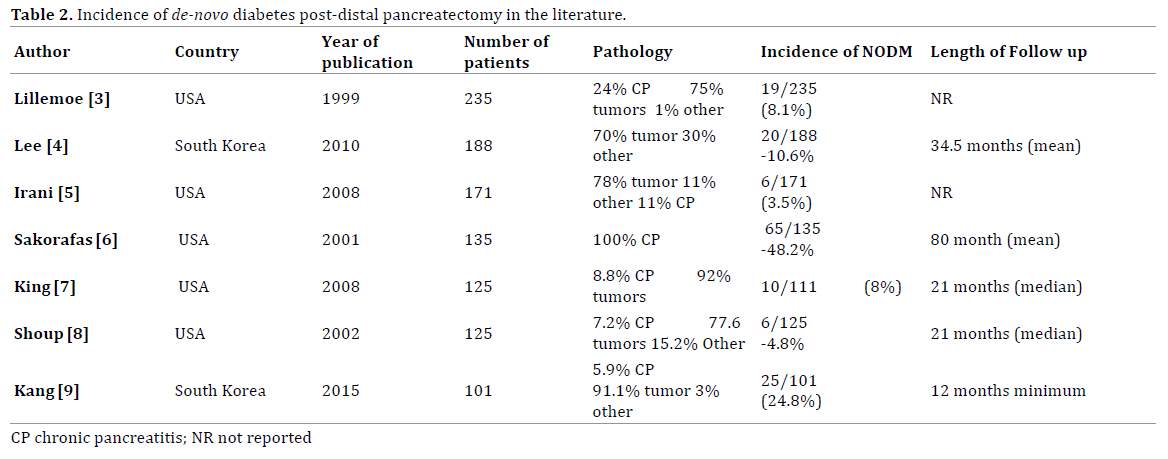
resection for CP and 14% in patients without CP [18, 19]. When isolating all published series that included over 100
patients, we found the mean incidence of de-novo DM to be
15.4% (Table 2).
In order to try not to overcall the incidence of DM in
the early postoperative period, we excluded plasma glucose
levels prior to 72 hours post-operatively. This decision
was instituted based on the findings of Davis et al. who
found the incidence of stress hyperglycemia in the general
surgery population increased daily for the first 72 hours.
Additionally for patients requiring prolonged intravenous
support, or enteral/parenteral nutrition the glucose levels
used to define DM were taken once those patients had
resumed a solid diet.
Interestingly, we did not see any correlation between the
volume of pancreatic resection and risk of developing postoperative
de-novo DM. This potential relationship has been
demonstrated in several studies, although, no relationship
has yet been established by gross specimen volume [1, 7, 20].
In the current study we calculated the volume of the resected
pancreas whereas prior studies that reported a correlation
used percentage of total pancreatic parenchyma [1, 7, 20].
Shirakawa et al. and Kang et al. both found the volume of
pancreatic tissue to be an independent risk factor of de-novo
post-operative DM by measuring resection volume by
computed tomography volumetry [9, 13].
Our results affirm the findings of Kang et al. who
reported high BMI is a pre-operative risk factor for de-novo
DM after DP [9]. High pre-operative BMI can also
be implicated in other perioperative complications as
established by Tee and colleagues, who investigated the
outcomes of elective distal pancreatectomy in patients
with metabolic syndrome, their principle findings included
a 42% greater odds of major morbidity (P<0.01), 59%
greater odds of deep/organ space surgical site infection
(P<0.01), and two-fold greater odds of respiratory failure
(P<0.01) [21]. The effects of pre-operative obesity are not
limited to the consequences of glucose metabolism they
also have an association with pancreatic steatosis which is
a known risk factor for developing pancreatic fistulas after
elective partial pancreatectomy [22, 23, 24, 25].
Although our results determine there is not a
statistically significant correlation with the volume of
pancreas resected and the incidence of de-novo DM
there are limitations to this conclusion, most notably the
standardization and length of follow up. Requisition of
long term outcomes were difficult due to out initiation being a quaternary referral center where often many of
our patients do not follow up with primary care physicians
in our health system. Our study analyzed preoperative
and post-operative serum plasma glucose levels which
are more difficult to establish plasma glucose trends from
when compared to serum hemoglobin A1c levels. Future
studies may benefit from incorporating pre-operative
serum hemoglobin A1c values into their protocols to
examine the predictive nature of preoperative plasma
glucose control on post-operative outcomes.
The high prevalence of obesity and the associated
risk factors of developing de-novo DM when entering
the operating room with a high BMI give this study
important clinical implications, the most notable being
the need to diligently monitor patients with high BMI’s
for de-novo DM after distal pancreatectomy. Diabetes
has been shown to be a predictor of worse survival in
all stages of disease and specifically is associated with
negative clinical outcomes in those with pancreatic
ductal adenocarcinoma and those undergoing elective
distal pancreatectomy [26, 27, 28].
CONCLUSION
De-novo diabetes is common following DP but its
development is independent of the size of the resection
specimen. Furthermore, patient demographic factors, and
the histopathological diagnosis did influence the incidence
of de-novo DM. It would however appear that a high preoperative
BMI is a significant risk factor for developing de-novo
post-operative DM, and obese patients should be counseled
as to a higher risk for diabetes, and be closely monitored
for the development of this important complication. The
association of DM and individual pancreatic pathologies of
both benign and malignant disease may indicate that there is
subclinical DM prior to surgery, possibly due to parenchymal
obstruction and destruction that is not appreciated clinically.
This important finding requires further evaluation in a
detailed prospective study.
Conflict of Interest
The authors declare that they have no conflicts of
interest.
References
- Slezak LA, Andersen DK. Pancreatic resection: Effects on glucose
metabolism. World J Surg 2001; 25:452-460. [PMID: 11344398]
- American Diabetes Association. Classification and diagnosis of
diabetes. Diabetes Care 2016; 39(Suppl 1):S13e22. [PMID: 26696675]
- Lillemoe KD, Kaushal S, Cameron JL, Sohn TA, Pitt HA, Yeo CJ. Distal
pancreatectomy: Indications and outcomes in 235 patients. Ann Surg
1999; 229:693-8; discussion 698-700. [PMID: 10235528]
- Lee SE, Jang JY, Hwang DW, Lee KU, Kim SW. Clinical efficacy of organpreserving
pancreatectomy for benign or low-grade malignant potential
lesion. J Korean Med Sci 2010; 25:97-103. [PMID: 20052354]
- Irani JL, Ashley SW, Brooks DC, Osteen RT, Raut CP, Russell S, et al.
Distal pancreatectomy is not associated with increased perioperative
morbidity when performed as part of a multivisceral resection. J
Gastrointest Surg 2008; 12:2177-2182. [PMID: 18677539]
- Sakorafas GH, Sarr MG, Rowland CM, Farnell MB. Postobstructive
chronic pancreatitis: Results with distal resection. Arch Surg 2001;
136:643-648. [PMID: 11387000]
- King J, Kazanjian K, Matsumoto J, Reber HA, Yeh MW, Hines OJ, et al.
Distal pancreatectomy: Incidence of postoperative diabetes. J Gastrointest
Surg 2008; 12:1548-1553. [PMID: 18543045]
- Shoup M, Brennan MF, McWhite K, Leung DH, Klimstra D, Conlon KC.
The value of splenic preservation with distal pancreatectomy. Arch Surg
2002; 137:164-168. [PMID: 11822953]
- Kang JS, Jang JY, Kang MJ, Kim E, Jung W, Chang J, et al. Endocrine
function impairment after distal pancreatectomy: Incidence and related
factors. World J Surg 2016; 40:440-446. [PMID: 26330237]
- Malka D, Hammel P, Sauvanet A, Rufat P, O'Toole D, Bardet P, et al. Risk
factors for diabetes mellitus in chronic pancreatitis. Gastroenterology
2000; 119:1324-1332. [PMID: 11054391]
- DiNorcia J, Ahmed L, Lee MK, Reavey PL, Yakaitis EA, Lee JA, et al.
Better preservation of endocrine function after central versus distal
pancreatectomy for mid-gland lesions. Surgery 2010; 148:1247-54;
discussion 1254-6. [PMID: 21134558]
- Lee BW, Kang HW, Heo JS, Choi SH, Kim SY, Min YK, et al. Insulin
secretory defect plays a major role in the development of diabetes in
patients with distal pancreatectomy. Metabolism 2006; 55:135-141.
[PMID: 16324932]
- Shirakawa S, Matsumoto I, Toyama H, Shinzeki M, Ajiki T, Fukumoto
T, et al. Pancreatic volumetric assessment as a predictor of new-onset
diabetes following distal pancreatectomy. J Gastrointest Surg 2012;
16:2212-2219. [PMID: 23054900]
- You DD, Choi SH, Choi DW, Heo JS, Ho CY, Kim WS. Long-term effects
of pancreaticoduodenectomy on glucose metabolism. ANZ J Surg 2012;
82:447-451. [PMID: 22571457]
- Dominguez-Munoz JE. Pancreatic exocrine insufficiency: diagnosis
and treatment. J Gastroenterol Hepatol 2011; 26(Suppl 2):12-6.
[PMID: 21323992]
- Davis G, Fayfman M, Reyes-Umopierrez D, Hafeez S, Pasquel FJ,
Vellanki P, et al. Stress hyperglycemia in general surgery: why should we
care? J Diabetes Complications 2018; 32:305-309. [PMID: 29273446]
- Burkhart RA, Gerber SM, Tholey RM, Lamb KM, Somasundaram A,
McIntyre CA, et al. Incidence and severity of pancreatogenic diabetes
after pancreatic resection. J Gastrointest Surg 2015; 19:217-225.
[PMID: 25316483]
- Epelboym I, Winner M, DiNorcia J, Lee MK, Lee JA, Schrope B, et al.
Quality of life in patients after total pancreatectomy is comparable with
quality of life in patients who undergo a partial pancreatic resection. J
Surg Res 2014; 187:189-196. [PMID: 24411300]
- De Bruijn KM, van Eijck CH. New-onset diabetes after distal
pancreatectomy: A systematic review. Ann Surg 2015; 261:854-861.
[PMID: 24983994]
- Hutchins RR, Hart RS, Pacifico M, Bradley NJ, Williamson RC. Longterm
results of distal pancreatectomy for chronic pancreatitis in 90
patients. Ann Surg 2002; 236:612-618. [PMID: 12409667]
- Tee MC, Ubl DS, Habermann EB, Nagorney DM, Kendrick ML, Sarr
MG, et al. Metabolic syndrome is associated with increased postoperative
morbidity and hospital resource utilization in patients undergoing
elective pancreatectomy. J Gastrointest Surg 2016; 20:189-98; discussion
198. [PMID: 26553267]
- Gaujoux S, Cortes A, Couvelard A, Noullet S, Clavel L, Rebours V,
et al. Fatty pancreas and increased body mass index are risk factors of
pancreatic fistula after pancreaticoduodenectomy. Surgery 2010; 148:15-
23. [PMID: 20138325]
- Lee SE, Jang JY, Lim CS, Kang MJ, Kim SH, Kim MA, et al. Measurement
of pancreatic fat by magnetic resonance imaging: Predicting the
occurrence of pancreatic fistula after pancreatoduodenectomy. Ann Surg
2010; 251:932-936. [PMID: 20395858]
- Mathur A, Pitt HA, Marine M, Saxena R, Schmidt CM, Howard TJ, et
al. Fatty pancreas: A factor in postoperative pancreatic fistula. Ann Surg
2007; 246:1058-1064. [PMID: 18043111]
- Smits MM, van Geenen EJ. The clinical significance of pancreatic
steatosis. Nat Rev Gastroenterol Hepatol 2011; 8:169-177.
[PMID: 21304475]
- Walter U, Kohlert T, Rahbari NN, Weitz J, Welsch T. Impact of
preoperative diabetes on long-term survival after curative resection of
pancreatic adenocarcinoma: A systematic review and meta-analysis. Ann
Surg Oncol 2014; 21:1082-1089. [PMID: 24322532]
- Yuan C, Rubinson DA, Qian ZR, Wu C, Kraft P, Bao Y, et al. Survival
among patients with pancreatic cancer and long-standing or recentonset
diabetes mellitus. J Clin Oncol 2015; 33:29-35. [PMID: 25403204]
- Hart PA, Bellin MD, Andersen DK, Bradley D, Cruz-Monserrate Z,
Forsmark CE, et al. Type 3c (pancreatogenic) diabetes mellitus secondary
to chronic pancreatitis and pancreatic cancer. Lancet Gastroenterol
Hepatol 2016; 1:226-237. [PMID: 28404095]

