Introduction
There is good
evidence that reduction in cardio-vascular events and mortality can be achieved
in coronary heart disease (CHD) patients by lowering serum cholesterol,
controlling blood pressure, and taking aspirin and making lifestyle changes
such as stopping smoking.[1–5] Therefore a good scientific con-sensus
exists on e¡ective measures in secondary pre-vention of CHD.[6,7] The
potential for preventive action is great in CHD patients but research indicates
that considerable improvement is needed in practice.[8] In Scotland it
is not known how these recommendations are followed and to what extent health
board level programmes can improve the situation.
Based on the European recommendations all cor-onary patients should
have their blood pressure con-sistently below 140/90 mmHg.[6] If the
goal is not achieved with lifestyle changes, drug therapy should be used. In
blood total cholesterol the goal is below 5 mmol/l and in low-density lipids
(LDLs) 3 mmol/l. Statins should be used if the goal is not achieved by dietary changes.
Aspirin should be given to virtually all patients, beta-blockers after
myocardial infarction (MI), and angiotensin converting enzyme (ACE) inhibitor
to patients with heart failure.
Scotland has one of the highest rates of CHD in the world and CHD is
therefore a major national and local priority.[9,10] The decision to
target secondary preven-tion was made after a local review of CHD services. A
practice nurse survey was also performed which high-lighted the need for
training and better patient information materials. These led to the formation
of the Hearts in the Borders project, which is a multi-disciplinary
multi-organisational initiative with the aim of providing the highest possible
standards of care, and improving the health of patients with CHD in the
Scottish Borders. This paper describes the successful implementation
initiative.
Methods
The Scottish
Borders is a large (4700 km2) rural area with a population of 106
000, of which 19% are over 65 years. Healthcare is provided by a single health
board and by one acute hospital trust, one primary care trust (PCT), and two
local health care co-operatives, which include 87 general practitioners (GPs)
and 22 practices.
The project’s multidisciplinary steering group con-sisted of a
cardiologist/physician, guidelines advisor, audit co-ordinator, health
promotion specialist, sup-port pharmacist, GPs, practice and hospital nurses,
dietician, and
public health consultant. The project’s implementation plan was divided into
three sections with smaller multidisciplinary subgroups set up to manage each
stage (see Figure 1).

Figure 1: The project's implementation plan showing the flow of events
Stage 1
A local
guideline for the management of secondary prevention of CHD was developed and a
draft presented at a consensus meeting to improve the acceptance and
implementation (see Figure 2). The guideline was modified in the light of the
comments made and a system was set up to review the evidence. The guideline was
updated after two years.

Figure 2: The Borders secondary prevention of CHD updated guidelines.
BGH: Borders General Hospital; BMI: Body mass index; BP: blood pressure;GPERS: GP Exercise Referral Scheme (a scheme where GPs are
able to prescribe exercise to patients. Patients then atttend their local sports centre where they are assessed by a sports trainer, and an
exercise programme is developed for that person).
To measure the impact of implementing the devel-oped guideline, a
baseline audit was conducted prior to their publication and a disease
management system for secondary prevention of CHD introduced. An audit database
was set up of patients under 75 years with a recent event or past medical
history of MI, angioplasty and/or coronary artery bypass grafting (CABG) based
on review of medical records in health centres and hospitals.
Following the baseline audit the guideline was released and an audit
report provided sta¡ with feed-back regarding their practice and comparisons
between practices of targeted standards for improve-ments. The targeted
standards were blood cholesterol levels, blood pressure, lifestyle measures
(that is, smoking, dietary and exercise advice) and prescribing of aspirin,
statins, ACE inhibitors and beta-blockers. Data on hospital admissions were
also collected. The audit cycle was repeated at a 12- and 24-month interval
after the baseline audit.
Stage 2
Following the
baseline audit, practices set up disease registers to facilitate the management
(for example, recall of these targeted patients). The audit allowed us to
identify areas where change was necessary (for example, smoking cessation
counselling). Auditing was both labour intensive and expensive under the
current auditing system which involved manual data collection at each practice
and inputting the informa-tion into a central CHD database for analysis and
reporting. In order to improve e¤ciency and e¡ect-iveness and enhance the
project’s achievements, a subgroup was set up to introduce a system that will
facilitate paperless data collection and automatic analysis and reporting,
allowing easy identification of this high-risk group of patients and their
modifiable risk factors.
We are currently piloting a system that involves electronic data
collection using the Clinical Disease Support System (CDSS) for the General
Practice Support System for Scotland (GPASS) at
practice level. From GPASS the anonymised information can flow into a
central SQL database for automatic Borders-wide analysis and reporting. At
practice level electronic auditing functions will also be provided through CDSS
and GPASS.
Stage 3
Following the
outcome of the practice nurse survey a subgroup was set up to address patients’
lifestyles. A training programme was introduced and a resource pack was
developed to support it, containing informa-tion sheets, lea• ets, patient
diaries, etc, covering generic motivational interviewing and the major lifestyle risk
factors. The information contained in the pack is consistent with current
knowledge, on CHD risk factors and relevant to the area (for example, walking
groups in the Borders).
The lifestyle counselling training programme was developed locally and
attendance is multidisciplinary. A two-day course on motivating change is
followed by topic-based courses on stress management, smoking cessation,
healthy eating, safer drinking and working with people with learning disabilities.
Uptake of this rolling programme is high with 225 participants in the first two
years. Feedback from the courses ensures quality.
The resource pack is used in all training and sent to every practice,
hospital and pharmacy. Combining the use of the resource pack with all the
training ensures that all health
professionals in the Borders provide consistent and up to date information
regardless of professional background or location. A questionnaire survey of
users of the pack found it to be useful.
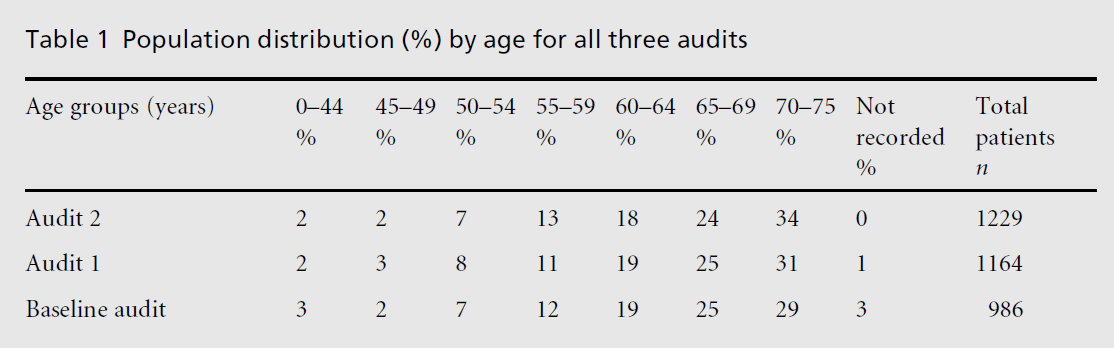
Results
For all three
audits the sex distribution was approxi-mately three-quarters male to
one-quarter female. The percentage prevalence was calculated by dividing the
CHD population by all patients registered with a GP and multiplying by 100. The
overall prevalence of CHD increased with age, peaking in the 70–75 years age
group (see Table 1) with an overall prevalence of 0.93% (n = 986) at
baseline, which stabilised at around 1.1% for the other two audits (that is,
1.10% (n = 1164) for audit 1 and 1.14% (n = 1229) for audit 2),
re• ecting improved case finding.
Cigarette smoking habits remained at 19% (see Figure 3) despite
targeted resources to reduce this. However, the number of ex-smokers increased
from 48% (n = 476) at baseline to 51% (n = 594) and 53% (n = 651) for audits 1 and 2 respectively, suggesting better
recording. Over the three audits carried out, dietary advice was given to
patients more often than exercise advice (see Figure 4). Dietary advice given
increased from 66% (n = 702) at baseline to 90% (n = 995) in the
last audit. Similarly, exercise advice given improved from 52% (n = 516)
to 72% (n = 883) in the final audit. This shows the huge focus on
lifestyle issues re• ected by the guidelines, training and the resources pack.
In the baseline audit, the number of patients with target total blood
cholesterol below 5 mmol/l was 29% (n = 283) (see Figure 5). This
increased to 45% (n = 528) 12 months later (that is, audit 1) and 62% (n = 763) by audit 2. This improvement was mainly achieved through targeted statin
prescribing which rose from 51% (n = 507) at baseline to 63% (n =
739) at audit 1 and 75% (n = 917) at audit 2 (see Figure 6). The
evidence-based benefits of lowering total choles-terol are reduced morbidity
and mortality, and the results show improving standards of care for this
high-risk group of patients.

Figure 3: The distribution of cigarette smoking habits.

Figure 4: The distribution of dietary and exercise advice given to patients.

Figure 5:The distribution of total blood cholesterol
for all patients in the Hearts in the Borders project.

Figure 6:The distribution of statin prescribing in the
Hearts in the Borders project. The percentage at the
top of each column represents the total number of
patients taking a statin. The tint-coded columns
indicate the distribution of each statin drug. Note:
cerivastatin was withdrawn after the second audit
and is no longer available.
The number of patients within the target systolic blood pressure of
below 140 mmHg increased from 43% (n = 428) at baseline to 49% (n = 565) by audit 1 and 55% (n = 679) by audit 2, showing an improving
trend in patients within the target systolic blood pressure (see Figure 7). Target diastolic blood pressure showed a similar improving trend
with 61% (n = 601) of patients with a diastolic blood pressure below the
target of 85 mmHg at baseline increasing to 66% (n = 766) by audit 1 and
74% (n = 905) by audit 2 (see Figure 8).

Figure 7:The distribution of systolic blood pressure
for patients in the Hearts in the Borders project.

Figure 8:The distribution of diastolic blood pressure
for patients in the Hearts in the Borders project.
In the baseline audit, aspirin prescription level was 87% (n =
862), increasing to 88% foraudit 1 (n = 1025) and remaining at
88% for audit 2 (n = 1085) (see Figure 9). In all the audits 5% of
patients had a contraindication to aspirin use.
In the baseline audit 15% (n = 149) of patients had been
admitted with a cardiac episode (see Figure 10). By audit 1, 12 months later,
cardiac admissions had reduced to 11% (n = 132) and a further reduction
to 10% (n = 124) was achieved by audit 2. The percentage of patients
admitted to hospital for other reasons was reduced from 17% (n = 164) at
baseline to 10% (n = 122) by audit 2. Overall, total
admissions were reduced from 32% (n = 313) at baseline to 20% (n = 246) by audit 2.

Figure 9:The distribution of aspirin prescribing for
patients in the Hearts in the Borders project.
Discussion
Major
improvement occurred in cholesterol control: the proportion of patients with
their cholesterol below 5 mmol/l, which was the target in the programme,
increased from 29% to 62%. The main reason for this was the increase in statin
treatment. Reducing choles-terol to this extent, by extrapolation from the
4S-study, suggests that over a five-year period in this population, 31–65
coronary events will be avoided, and 11–27 coronary deaths avoided or delayed.[1]
Hospital admissions decreased from 15% to 10% for cardiac events while
non-cardiac admissions for this group decreased from 17% to 10%. A reduction in
acute admissions was also found in Campbell’s study and requires more
investigation.[11,12] It suggests that disease management programmes
in primary care can keep CHD patients out of hospital. This is a major benefit
for patients and can generate considerable hospital savings. The local health
board has recognised this success by allocating additional funds to the primary
care prescribing budget for statins. The additional funding was important not
only for bud-geting reasons, but as recognition for GPs that the local
decision-making process re• ected the increasing costs of improving quality in
primary care.

Figure 10:The distribution of cardiac and
non-cardiac hospital admissions for secondary
prevention of CHD patients in the Hearts in the
Borders project.
However, the percentage of patients who had received dietary advice was
relatively low at baseline. There can be two main reasons for this: dietary
advice is not regarded as treatment and it is not recorded in the medical files, or it is not given to patients for the same reason. The e¡ect of dietary
changes depends on the baseline diet and individual sensitivity to dietary
changes. In spite of the huge number of studies done on blood cholesterol and
diet, the original Key’s equation is still valid. Cholesterol decline depends
mainly on the decline in saturated and increase in polyunsaturated fats
following the formula: decline in cholesterol (mmol/l) = 0.0397 £ (2 £ decline
in saturated fats as energy percent + increase in poly-unsaturated fats as
energy percent). If we take a typical traditional western diet with 20% of
energy intake in saturated fats and 5% of polyunsaturated fats, and change it
to 8% of saturated and 8% of polyunsatu-rated, the serum cholesterol will
decline by about 1 mmol/l.[13] However, there is a large variation in
how individual people react to dietary changes. By the last audit with the
large focus on lifestyle changes through training and the resource pack,
‘dietary advice given’ had risen to 90% and ‘exercise advice’ to 72%. This demonstrates the
e¡ectiveness of a centrally driven approach. With the targeted training and
resource pack, not only has the lifestyle advice given to patients improved but
also the quality of the advice given (that is, it is up to date and evidenced
based).
Aspirin is an evidence-based cost-e¡ective drug and prescribing was
high in all three audits. Trends towards better control of blood pressure, both
for systolic and diastolic pressure, were evident. The evidence suggests that
lowering blood pressure and prescribing aspirin has a beneficial e¡ect in
reducing cardiovascular events.[14]
There was no change with regard to smoking cessation despite the focus
and resources allocated to this. This suggests that for patients who have not
given up smoking following a myocardial episode, giving up smoking may prove
more di¤cult. Introduction of practice-based smoking cessation support, with
nico-tine replacement therapy or bupropion, could be the most important health
intervention for these cardio-vascular patients. If CHD patients continue
smoking, the risk of new infarction or graft occlusion is much higher compared
with patients who quit smoking.[4] Following the last audit, new
methods of helping this high-risk group of patients are being investigated.
Conclusion
One major positive
e¡ect of the audits was that all practices now have a CHD register. Also new
ways of working across professional and organisational divides, re• ected in
the guideline, training pro-gramme and resource pack, were developed. Evidence
alone seldom changes practice but recently we have understood better how to
lead improvements.[15,16] The successful implementation of this
project is due to the use of multiple approaches including system redesign,
clinical leadership, evidence-based guidelines, audit and feedback, training,
peer group e¡ects and prac-tical support for the participating practices
including IT-based solutions. Lessons learnt have allowed more rapid planning
of a project to implement hypertension guidelines throughout the region.
Acknowledgements
We are grateful
to all 22 primary healthcare teams in the Scottish Borders, who participated in
this project. The project was funded by grants from the Primary Care
Development Fund of the Scottish Executive, Borders NHS Board and an educational
grant from Bayer PLC.
References
- Scandinavian
Simvastatin Survival Study Group. Ran-domised trial of cholesterol lowering in
4444 patients with coronary heart disease: the Scandinavian simva-statin
survival study (4S). Lancet 1994;344:1383–9.
- Sacks FM, Pfe¡er MA,
Moye LA et al. The e¡ect of pravastatin on coronary events after
myocardial infarc-tion in patients with average cholesterol level. New England
Journal of Medicine 1996;335:1001–9.
- Brower WS and Hulley
SB. Clinical trials of hyperten-sion treatment: implications for subgroups. Hyperten-sion 1989;13(Suppl 1):151–6.
- Daly LE. Long term
e¡ect on mortality of stopping smoking after unstable angina and myocardial
infarc-tion. British Medical Journal 1983;287:324–6.
- Antiplatelet Trialists’
Collaboration. I: Prevention of death, myocardial infarction, and stroke by
prolonged antiplatelet therapy in various categories of patients. British Medical Journal 1994;308:81–106.
- Prevention of Coronary
Heart Disease in Clinical Prac-tice. Recommendations of the Second Join Task
Force of European and other Societies on Coronary Prevention. European Heart Journal 1998;19:1434–503.
- Scottish
Intercollegiate Guidelines Network. Secondary Prevention of Coronary
Heart Disease Following Myocar-dial Infarction. National clinical guideline.
Edinburgh:SIGN Publication Number 41, January 2000.
- EUROASPIR Study Group.
EUROASPIR. A European Society of Cardiology survey of secondary prevention of
coronary heart disease: principal results. European Heart Journal 1997;181:569–82.
- World Health
Organization. Health in Europe 1997. Report of third evaluation of
progress towards health for all in the European Region of WHO (1996–1997). Geneva:World Health Organization, 1997.
- NHS Scotland. Our
National Health: a plan for action, a plan for change. Edinburgh:
NHS Scotland, ScottishExecutive, 2000.
- Campbell N, Thain J,
Deans FG, Ritchie LD, Rowles JM and Squair JL. Secondary prevention clinics
for coronary heart disease: randomised trial of e¡ect on health. British Medical Journal 1998;316:1434–7.
- Murchie P, Campbell NC,
Ritchie LD, Simpson JA and Thain J. Secondary prevention clinics for coronary
heart disease: four year follow up of a randomised controlled trial in primary
care. British Medical Journal 2003; 326(7380):84.
- Keys A, Anderson JT and
Grande F. Serum cholesterol response to changes in the diet. IV: Particular
saturated fatty acids in diet. Metabolism 1965;14:776–87.
- Hansson L, Zanchetti A,
Carruthers SG et al. E¡ects of intensive blood-pressure lowering and
low-dose aspirin in patients with hypertension: principal results of the
Hypertension Optimal Treatment (HOT) randomised trial. Lancet 1998;351:1755–62.
- Berwick DM. A primer on
leading the improvement of systems. British Medical Journal 1996;312:619–22.
- Grol R. Beliefs and
evidence in changing clinical prac-tice. British Medical Journal 1997;315:418–21.
Conflicts of Interest
None.

