Keywords
Diuresis; Fluid Therapy; Pancreatitis; Saline Solution,
Hypertonic
Abbreviation
SIRS systemic inflammatory response syndrome
INTRODUCTION
Acute pancreatitis has a high annual incidence of
13 – 85/100,000 persons worldwide with mortality up
to 20% in case of infected pancreatic necrosis [1, 2, 3, 4, 5]. Persistent (multi) organ failure further increases
mortality to 35% [5]. Adequate fluid resuscitation and
pain management are the cornerstones in early treatment
of acute pancreatitis. Based on retrospective studies, early fluid resuscitation seems to be associated with a reduced
incidence of systemic inflammatory response syndrome
(SIRS), organ failure and mortality [6, 7]. Current
international guidelines for the management of acute
pancreatitis recommend vigorous infusion of a balanced
salt solution (Ringer’s lactate 5-10 ml/kg/h) to maintain
a urinary output of >0.5 – 1.0 ml/kg/h [8]. However, the
recommendation for Ringer’s lactate is mainly based on
one relatively small and early-terminated randomized trial
in patients suffering from mild acute pancreatitis [9]. The
latter might explain the fact that many physicians still treat
acute pancreatitis patients with normal saline infusion.
The composition of the infusion fluid used has received
increasing attention in recent years [10]. Balanced salt
solutions better match the composition of blood plasma
than the widely used normal saline [11]. In clinical trials in
patients with pathologies other than pancreatitis (i.e. renal
transplantation, dehydration, abdominal aortic aneurysm surgery), balanced salt solutions have been shown to
prevent the development of hyperchloremic acidosis and
to reduce the need for blood transfusion compared to
resuscitation with normal saline [12, 13, 14, 15, 16, 17, 18]. In acute pancreatitis, balanced salt solutions have
been suggested to reduce inflammation [9, 14]. Although
metabolic and clinical advantages of balanced salt infusion
are promising, convincing evidence for a clinical benefit
is lacking. Most clinical outcome studies have used
heterogeneous patient populations, various types and
volumes of infusion fluids as well as different endpoints,
which might have obscured the clinical benefit of balanced
salt solutions. Moreover, the effects of large infusion
volumes on urinary output, laboratory parameters (i.e.
plasma sodium and potassium level, acid-base status)
and morbidity (i.e. organ failure) in patients with acute
pancreatitis are unknown.
We aimed to evaluate current clinical practice regarding
infusion fluid (i.e. volume) in a homogenous multicenter
patient population with predicted severe acute pancreatitis
between 2008 and 2012, a period in which normal saline
was predominantly used, and to describe biochemical
parameters. We performed a post-hoc analysis on data
collected during a randomized controlled trial, which
consisted of a homogenous patient population that was
treated with well-documented infusion therapy and of
which biochemical parameters had been prospectively
collected. Insight into the infusion policy and its effect
on biochemical parameters will help to refine future
recommendations on type and volume of infusion fluid in
pancreatitis patients.
METHODS
Study Population and Design
In this study a post-hoc analysis was performed in
all patients of the ‘Pancreatitis, very early compared
with normal start of enteral feeding’ (PYTHON) trial,
a randomized controlled, multicenter trial in patients
with predicted severe acute pancreatitis conducted in 19
Dutch hospitals (6 university medical centers and 13 large
teaching hospitals) from August 2008 through June 2012
[19, 20]. The original trial protocol was approved by the
institutional review board of the University Medical Center
Utrecht and all the participating centers. Also patients or
their legal representatives provided written informed
consent [20].
Acute pancreatitis was defined by at least two of the
following features: typical abdominal pain, a serum lipase
or amylase that was more than 3 times the upper limit of
normal, or characteristic findings on abdominal CT-scan
[20]. Predicted severe disease was defined by an Acute
Physiology and Chronic Health Evaluation (APACHE) II
score of 8 or higher [21], a modified Glasgow score of 3 or
higher [22], or a serum C-reactive protein (CRP) level higher
than 150 mg/L [23], within 24 hours after presentation
to the emergency department [20]. In the PYTHON trial,
patients were randomized between early nasoenteric tube feeding (within 24 hours after randomization) or
oral feeding (within 72 hours) [19, 20]. Intravenous fluid
therapy was commenced at the emergency department,
as judged by the attending physician, and continued
throughout the first days. The trial protocol specified
no specific type of fluid therapy. Vital signs and serum
markers were used to titrate the amount of fluid [20].
Objective
The objective of the present study was to analyze the
infusion regimen (i.e. volume) given during admission
and to evaluate the urinary output, plasma sodium and
potassium level, acid-base status, inflammatory parameters
and the need for correction of biochemical abnormalities.
Target urine production was defined as a urine output
of >0.5 ml/kg/h according to the current international
guidelines for the management of acute pancreatitis [8].
Hypernatremia was defined by a plasma sodium level
>146 mmol/L, hypokalemia indicated a plasma potassium
level <3.8 mmol/L and acidosis was defined by a pH <7.35.
Statistical Analysis
Categorical data were presented as frequencies and
percentages, continuous data as mean and standard
deviation (SD) or median and interquartile range (IQR),
depending on normality of distribution. The association
between the amount of fluid therapy and organ failure was
evaluated using the chi-square test for categorical data.
T-tests were used for normally distributed continuous
variables and Mann-Whitney U-tests for non-normally
distributed continuous variables. Correlations were
determined with the Spearman’s rank correlation for nonnormally
distributed continuous variables. A two-sided
P value of less than 0.05 was considered to be statistical
significant. All analyzes were performed using IBM SPSS
Statistics for Windows (version 21, IBM Corp, Armonk, NY,
USA).
RESULTS
Baseline Characteristics and Infusion Regimen
The study population consisted of 205 patients with
predicted severe acute pancreatitis. Mean age was 65±15
years. Baseline characteristics are summarized in Table 1.
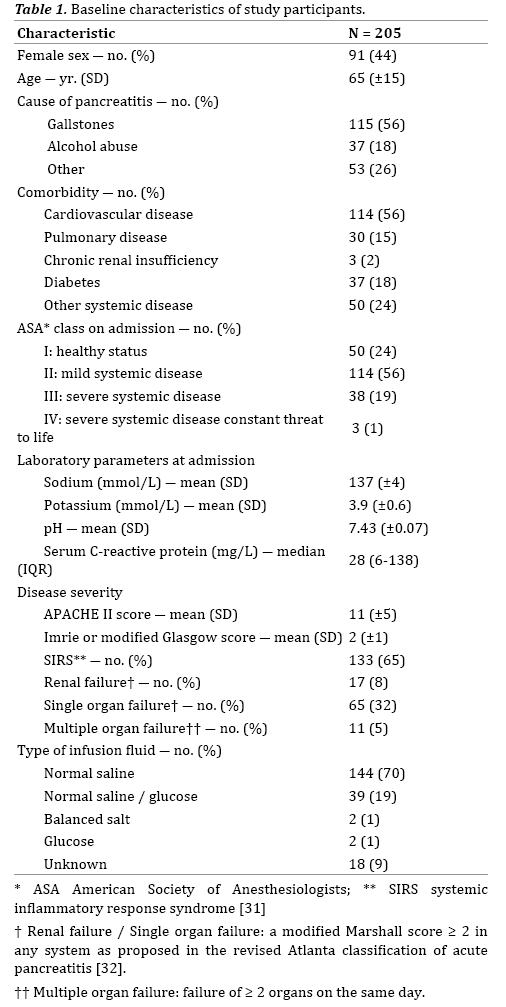
The majority of patients received intravenous fluid
resuscitation with normal saline (144 patients, 70%),
while only 2 patients (1%) were treated with a balanced
salt solution. Forty-one patients (20%) were treated with
a glucose-containing solution and in 18 patients (9%) the
type of infusion fluid was not specified.
In patients receiving normal saline, the median volume
was 3000, 3200 and 3000 ml at day 1, 2 and 3 respectively,
thereafter the volume decreased quickly (Figure 1). Both
total volume as well as volume per kg body weight were
relatively stable during the first 72 hours, but decreased
thereafter. Because the majority of patients were treated
with normal saline, no comparison could be made between
the administration of normal saline and a balanced salt solution. Therefore further analysis on biochemical
parameters was performed solely in the patients receiving
normal saline.
Figure 1. Volume of infusion fluid delivered during admission.
Diuresis in Patients Receiving Normal Saline
On the day of admission, patients who were treated
with normal saline had a limited diuresis that increased
in the following days (Figure 2). Table 2 shows patients
who achieved the target urine production of >0.5 ml/kg/h
during the first 72 hours. In 111 (77%), 89 (62%) and 85
(59%) patients the data on urine production at 24, 48 and
72 hours, respectively, were lacking.
Figure 2. Diuresis during admission.

Patients who did not reach the target urine output had
a median diuresis of 0.39 ml/kg/h (IQR 0.33 – 0.47 ml/
kg/h) at 24 hours, 0.37 ml/kg/h (IQR 0.25 – 0.41 ml/kg/h)
at 48 hours and 0.37 ml/kg/h (IQR 0.12 – 0.44 ml/kg/h) at 72 hours. As a result of the large volume of infusion fluid
administered with a limited diuresis, the fluid balance was
positive during the first 3 days (Figure 3), with a significant
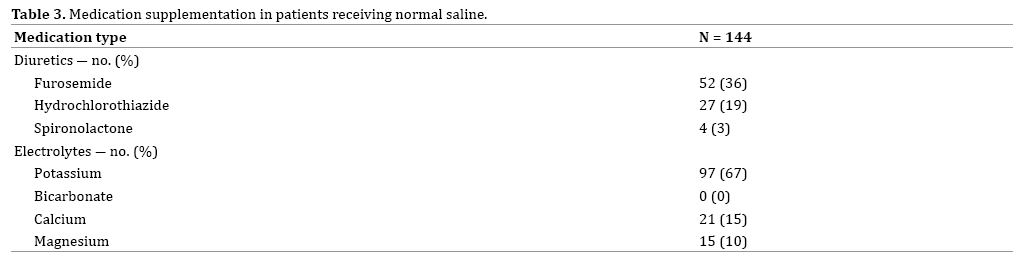
mean weight increase of 3.1±3.7 kg (P=0.002). Diuretics
were given to 68 patients (47%) during admission. In
these cases, furosemide was primarily used (Table 3).
Plasma Electrolytes and Acid-Base Status in Patients
Receiving Normal Saline
The plasma sodium level increased significantly during
admission, compared to baseline, for patients receiving
normal saline (1.8 mmol/L at 24 hours, 2.6 mmol/L at 48
hours and 2.2 mmol/L at 72 hours). Hypernatremia was
present in 2 patients (1%) at 24 hours, 4 patients (3%) at
48 hours and 6 patients (4%) at 72 hours.
There was a significant decrease of the mean plasma
potassium from 3.9±0.6 mmol/L to 3.7 ± 0.5 mmol/L at 72
hours. During admission 97 patients (67%) were treated
with potassium supplementation (Table 3). Hypokalemia
occurred frequently in patients receiving normal saline,
with 66 patients (46%) at 24 hours, 77 patients (53%)
at 48 hours and 89 patients (62%) at 72 hours, while at
these times more than 50% already was treated with oral
or intravenous potassium supplementation.
In addition, during the first 48 hours, administration of
normal saline was associated with a significant decrease
in pH from 7.43±0.07 to 7.28±0.13 (Figure 4) with
subsequent development of an acidosis (pH <7.35) in 8%
of patients.
Figure 4: Mean pH during admission.
Morbidity and Mortality in Patients Receiving Normal
Saline
The patients in this study with predicted severe acute
pancreatitis had significant morbidity and mortality. At
baseline 67% met the criteria for severe inflammatory
response syndrome. At that same time, 6% of the patients
receiving normal saline had multiple organ failure, 8% had
renal failure and 31% had single organ failure. Six months
after inclusion, 8% of the patients had died.
DISCUSSION
The present study shows that, between 2008 and
2012, fluid therapy in patients with predicted severe
acute pancreatitis was suboptimal. Most patients were
treated with normal saline with volumes less than
currently recommended. Due to this fact, no comparison
could be made regarding outcomes between patients
receiving normal saline and patients receiving a balanced
salt solution. For the patients receiving normal saline,
the urinary output target seemed to be reached in only
a minority of patients and in a substantial number of
patients hemodynamic and metabolic disturbances
occurred. Regarding the use of normal saline in this
patient cohort it should be noted that the guidelines,
which recommend aggressive infusion of a balanced
salt solution aiming at a urinary output of >0.5 ml/kg/h,
were introduced one year after the randomization for the
PYTHON trial was finished [8]. Despite the fact that the diuresis goal was reached and registered in only 35% of
patients, a significant mean weight increase occurred with
the need for administration of diuretics in 47% of patients.
In addition, patients receiving normal saline infusion had
a significant increase in plasma sodium level in the first 72
hours and a significant decrease in plasma potassium level
despite potassium supplementation was given in 67% of
these patients. Finally, acidosis developed in 8% of the
patients.
This study found that that infusion therapy with normal
saline led only in a minority of patients to the currently
recommended urine output of >0.5 ml/kg/h, while many
patients suffered from volume overload as indicated by
the applied diuretic therapy. The main goal of infusion
therapy is to ensure adequate tissue perfusion. However,
one might question whether urine output truly reflects
tissue perfusion, which possibly explains the low level
of recommendation (weak) in the current international
guidelines [8]. Interestingly, the amount of chloride a
specific infusion fluid contains, plays an important role in the effect of infusion fluid on diuresis. Infusion fluids
containing supra-physiological concentrations of chloride,
as is the case with normal saline, will induce intrarenal
vasoconstriction, suppress renin and subsequently
decrease glomerular filtration rate [11, 24, 25]. The ensuing
decrease in diuresis increases the risk of intravascular
volume overload. One might speculate that with the use
of the recommended balanced salt solutions, with a more
physiological chloride content, diuresis will better reflect
intravascular volume, and therefore prevent the need for
diuretic therapy [11].
Currently, there are no comparable studies that have
described the use of normal saline in patients with predicted
severe acute pancreatitis and their urinary output, need
for diuretics, plasma electrolytes and pH. Two previous
studies have only described other biochemical parameters
and clinical outcomes. Aboelsoud et al. investigated 198
patients with acute pancreatitis, admitted to the intensive
care unit (ICU), who received a median amount of 5600 ml
normal saline (130 patients) or 7200 ml Ringer’s lactate (68 patients) in the first 24 hours [26]. Patients receiving
normal saline had a significant higher mortality, decrease
in serum bicarbonate and increase in serum chloride, as
compared to those receiving Ringer’s lactate. However,
the ICU stay was significantly longer in the Ringer’s lactate
group. Wu et al. compared 21 patients who were treated
with normal saline with 19 patients treated with Ringer’s
lactate and showed that infusion of a mean volume of 4500
ml Ringer’s lactate, led to an 84% reduction in SIRS and a
significant lower CRP level at 24 hours from baseline [9].
The study of Aboelsoud is comparable to the present study
regarding the number of patients receiving normal saline.
However, both studies of Aboelsoud and Wu used a larger
volume of infusion fluid, described a shorter time period
and did not investigate the urinary output, use of diuretics,
plasma electrolytes and pH. In addition, there is one study
that investigated 103 patients who received 1000 ml
Ringer’s lactate or normal saline, followed by a 5% glucose
solution (1000–1500 ml) and a multi-electrolyte solution
(500–1000 ml) [27]. There was no significant difference
in pancreatic necrosis, administration of enteral nutrition,
duration of hospital stay and mortality between the two
groups. It is difficult to compare the latter study to our study
because of an entirely different composition of infusion
fluid. The present study gives an overview of biochemical
parameters in severe acute pancreatitis patients receiving
a large volume of normal saline, although it was not
possible to confirm causality in our post-hoc analysis.
The development of acidosis in the present study is in
agreement with previous studies on infusion therapy in
other diseases. Four studies in kidney transplant patients showed that normal saline infusion (2868 – 6100 ml)
significantly induced metabolic acidosis (pH 7.28 – 7.36),
whereas infusion of a balanced salt solution did not
affect the acid-base status [16, 17, 28, 29]. However, it
is important to note that renal transplant patients differ
from pancreatitis patients with respect to the underlying
disease and therapeutic interventions. Up to now, only
2 studies have investigated a non-surgical population.
Williams et al. studied healthy volunteers who were
treated with normal saline and, after a cross-over, received
Ringer’s lactate, wherein normal saline led to a significant
decrease of pH (from 7.42 to 7.38) and increase in serum
sodium level (from 140 to 141 mmol/L) [12]. Hasman et
al. confirmed the decrease in pH (from 7.40 to 7.36) in
dehydrated patients in the emergency department who
were treated with normal saline [18]. It is of note that the
follow up in these two latter studies is relatively short (1-2
hours compared to more than 3 days in the present study),
thereby possibly overlooking metabolic disturbances that
occur after 2 hours.
A significant decrease in serum potassium level, as seen
in our study, has so far been shown in one other study. Chua
et al. retrospectively studied patients with a diabetic ketoacidosis
who received 4425 ml of normal saline and had a
significant decrease in serum potassium level (from 5.6 to
4.3 mmol/L), however this effect might also be explained
by other interventions like insulin infusion [30]. The
previous mentioned studies of Hadimioglu and Hasman
showed a non-significant decline in serum potassium
with normal saline and O’Malley even showed an increase
in serum potassium (from 4.2 to 5.1 mmol/L) [16, 17, 18]. The result of this last study could be explained by
the fact that the kidney transplantation in itself can
be associated with a potassium release due to tissue
damage. Interestingly, despite the fact that balanced
salt solutions contain potassium, the infusion of these
solutions was not associated with a significant increase
in potassium.
The most important limitations of the current study
are the lack of randomization and retrospective design
with post-hoc analysis and concomitant missing data.
However, it is the first study outlining the actual clinical
practice in the Netherlands regarding the use of infusion
fluid in predicted severe acute pancreatitis. In addition, it
is tempting to speculate that infusion policies play a crucial
causal role in the development of metabolic disturbances
and fluid overload.
In conclusion, low urine output, need for diuretics and
biochemical abnormalities necessitating correction were
seen in a considerable amount of patients with predicted
severe acute pancreatitis, treated with normal saline.
Future intervention studies should assess to what extent
optimized fluid therapy (i.e. amount and composition)
can improve morbidity and mortality in patients with
predicted severe acute pancreatitis.
Acknowledgements
AES, JvG, ACA, MGB and MBR designed the protocol of
the present study. AES, CB, OJB and SvB collected the data.
AES and JvG analyzed the data. AES drafted the manuscript
together with JvG, ACA, OJB, MGB and MBR. All co-authors
(JvG, ACA, CB, OJB, WJB, HCS, MJB, HvG, SvB, MGB and
MBR) critically edited the manuscript and approved the
final version.
Conflicts of Interest and Source of Funding
There are no conflicts of interest and no sources of
funding.
References
- Yadav D, Lowenfels AB. The epidemiology of pancreatitis and pancreatic cancer. Gastroenterology 2013; 14:1252-61. [PMID: 23622135]
- Spanier B, Bruno MJ, Dijkgraaf MG. Incidence and mortality of acute and chronic pancreatitis in the Netherlands: a nationwide record-linked cohort study for the years 1995-2005. World J Gastroenterol 2013;19:3018-26. [PMID: 23716981]
- Omdal T, Dale J, Lie SA, Iversen KB, Flaatten H, Ovrebo K. Time trends in incidence, etiology, and case fatality rate of the first attack of acute pancreatitis. Scand J Gastroenterol 2011;46:1389-98. [PMID: 21830851]
- Munigala S, Yadav D. Case-fatality from acute pancreatitis is decreasing but its population mortality shows little change. Pancreatology 2016;16:542-50. [PMID: 27161172]
- vanSantvoort HC, Bakker OJ, Bollen TL, Besselink MG, Ahmed Ali U, Schrijver AM, et al. A conservative and minimally invasive approach to necrotizing pancreatitis improves outcome. Gastroenterology 2011;141:1254-63. [PMID: 21741922]
- Warndorf MG, Kurtzman JT, Bartel MJ, Cox M, Mackenzie T, Robinson S, et al. Early fluid resuscitation reduces morbidity among patients with acute pancreatitis. ClinGastroenterolHepatol 2011;9:705-9. [PMID: 21554987]
- Gardner TB, Vege SS, Chari ST, Petersen BT, Topazian MD, Clain JE, et al. Faster rate of initial fluid resuscitation in severe acute pancreatitis diminishes in-hospital mortality. Pancreatology 2009;9:770-6. [PMID: 20110744]
- Working Group IAPAPAAPG. IAP/APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology 2013;13(4 Suppl 2):e1-15. [PMID: 24054878]
- Wu BU, Hwang JQ, Gardner TH, Repas K, Delee R, Yu S, et al. Lactated Ringer's solution reduces systemic inflammation compared with saline in patients with acute pancreatitis. ClinGastroenterolHepatol 2011;9:710-7 e1. [PMID: 21645639]
- Pfortmueller CA, Fleischmann E. Acetate-buffered crystalloid fluids: Current knowledge, a systematic review. J Crit Care 2016;35:96-104. [PMID: 27481742]
- Severs D, Hoorn EJ, Rookmaaker MB. A critical appraisal of intravenous fluids: from the physiological basis to clinical evidence. Nephrol Dial Transplant 2015;30:178-87. [PMID: 24463187]
- Williams EL, Hildebrand KL, McCormick SA, Bedel MJ. The Effect of Intravenous Lactated Ringer's Solution Versus 0.9% Sodium Chloride Solution on Serum Osmolality in Human Volunteers. AnesthAnalg 1999;88:5. [PMID: 10320158]
- Scheingraber S, Rehm M, Sehmisch C, Finsterer U. Rapid Saline Infusion Produces Hyperchloremic Acidosis in Patients Undergoing Gynaecologic Surgery. Anesthesiology 1999;90:6. [PMID: 10319771]
- Waters JH, Gottlieb A, Schoenwald P, Popovich MJ, Sprung J, Nelson DR. Normal Saline Versus Lactated Ringer’s Solution for Intraoperative Fluid Management in Patients Undergoing Abdominal Aortic Aneurysm Repair: An Outcome Study. AnesthAnalg 2001;93:6. [PMID: 11574339]
- Takil A. Early postoperative respiratory acidosis after large intravascular volume infusion of lactated ringer's solution during major spine surgery. AnesthAnalg 2002;95:294-8. [PMID: 12145036]
- O'Malley CM, Frumento RJ, Hardy MA, Benvenisty AI, Brentjens TE, Mercer JS, et al. A randomized, double-blind comparison of lactated Ringer's solution and 0.9% NaCl during renal transplantation. AnesthAnalg 2005;100:1518-24. [PMID: 15845718]
- Hadimioglu N, Saadawy I, Saglam T, Ertug Z, Dinckan A. The effect of different crystalloid solutions on acid-base balance and early kidney function after kidney transplantation. AnesthAnalg 2008; 107:264-9. [PMID: 18635497]
- Hasman H, Cinar O, Uzun A, Cevik E, Jay L, Comert B. A Randomized Clinical Trial Comparing the Effect of Rapidly Infused Crystalloids on Acid-Base Status in Dehydrated Patients in the Emergency Department. Int J Med Sci 2012;9:6. [PMID: 22211091]
- Bakker OJ, van Santvoort HC, van Brunschot S, Ahmed Ali U, Besselink MG, Boermeester MA, et al. Pancreatitis, very early compared with normal start of enteral feeding (PYTHON trial): design and rationale of a randomised controlled multicenter trial. Trials 2011;12:73. [PMID: 21392395]
- Bakker OJ, van Brunschot S, van Santvoort HC, Besselink MG, Bollen TL, Boermeester MA, et al. Early versus on-demand nasoenteric tube feeding in acute pancreatitis. N Engl J Med 2014;371:1983-93. [PMID: 25409371]
- Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: A severity of disease classification system. Critical care medicine 1985;13:12. [PMID: 3928249]
- Corfield AP, Cooper MJ, Williamson RC, Mayer AD, McMahon MJ, Dickson AP, et al. Prediction of severity in acute pancreatitis: prospective comparison of three prognostic indices. The Lancet 1985. [PMID: 2863441]
- Neoptolemos JP, Kemppainen EA, Mayer JM, Fitzpatrick JM, Raraty MG, Slavin J, et al. Early prediction of severity in acute pancreatitis by urinary trypsinogen activation peptide: a multicentre study. The Lancet 2000;355:1955-60. [PMID: 10859041]
- Berend K, van Hulsteijn LH, Gans RO. Chloride: the queen of electrolytes? Eur J Intern Med 2012;23:203-11. [PMID: 22385875]
- Wilcox CS. Regulation of renal blood flow by plasma chloride. J Clin Invest 1983;71:725-35. [PMID: 6826732]
- Aboelsoud MM, Siddique O, Morales A, Seol Y, Al-Qadi MO. Fluid Choice Matters in Critically-ill Patients with Acute Pancreatitis: Lactated Ringer's vs. Isotonic Saline. R I Med J (2013)2016; 99:39-42. [PMID: 27706278]
- Lipinski M, Rydzewska-Rosolowska A, Rydzewski A, Rydzewska G. Fluid resuscitation in acute pancreatitis: Normal saline or lactated Ringer's solution? World J Gastroenterol 2015;21:9367-72. [PMID: 26309362]
- Khajavi MR, Etezadi F, Moharari RS, Imani F, Meysamie AP, Khashayar P, et al. Effects of normal saline vs. lactated ringer's during renal transplantation. Ren Fail 2008;30:535-9. [PMID: 18569935]
- Modi MP, Vora KS, Parikh GP, Shah VR. A comparative Study of Impact of Infusion of Ringer's Lactate Solution Versus Normal Saline on Acid-BAse Balance and Serum Electrolytes during Live Related Renal Transplantation. Saudi J Kidney Dis Transpl 2012;23:135-7. [PMID: 22237237]
- Chua HR, Venkatesh B, Stachowski E, Schneider AG, Perkins K, Ladanyi S, et al. Plasma-Lyte 148 vs. 0.9% saline for fluid resuscitation in diabetic ketoacidosis. J Crit Care 2012;27:138-45. [PMID: 22440386]
- Committee MotACoCPSoCCMCC. American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference: Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Crit Care Med 1992; 20:864-74. [PMID: 1597042]
- Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, et al. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut 2013;62:102-11. [PMID: 23100216]





