Keywords
hyperlipidaemia, self-medication, statins
Introduction
Cardiovascular
disease is one of the leading causes of morbidity and mortality.[1]
HMG-CoA reductase in-hibitor (statin) drugs are medications used to inhibit
cholesterol synthesis in the liver and are well docu-mented as being
effective in both primary and sec-ondary prevention of cardiovascular
disease.[2] Despite the evidence for effectiveness in primary
prevention, individuals at moderate ten-year risk of a first time
cardiovascular event are often not taking appropriate lipid lowering therapy.
More than 60% of individuals without previous coronary heart disease but
possess-ing multiple risk factors are not receiving statin treatment.[3]
In 2004 low dose simvastatin (10 mg) was re-classified in Great Britain
from prescription-only to over-the-counter (OTC) status.[4] This was
the first reclassification of a statin from prescription-only status in the
world. The OTC product license restricts sales to individuals likely to be at
moderate (10–15%) ten-year risk of a first coronary event. Further, this change
in status requires that pharmacists carry out a cardiovascular risk assessment,
but they do not need to measure cholesterol or blood pressure prior to sale.
Instead, the focus is on risk factors like age, smoking, family history of
early heart attack, overweight/obesity and race/ethnicity. Pharmacists are
encouraged to help patients in their determination of eligibility for these
products.
Allowing statins to be sold without a prescription has been widely
debated in Great Britain, Canada and the USA.[5–7] Issues of concern
include the ability of
consumers to
self-select drugs, monitoring and poten-tial interactions with prescribed
drugs.[6,8–10]
Little data actually exist regarding the impact of this policy and who
is receiving this treatment. One study assessed the impact of the OTC statin
policy on statin prescribing by looking at statin prescriptions written by
general practitioners (GPs) before and after the policy and concluded that,
because the number of statin prescriptions had dropped after the
implemen-tation of the policy, patients were getting their statins OTC.[11]
However, that study did not actually assess whether any patient received OTC
statins so the change in prescribing could have been due to other factors.
Thus, the purpose of this study is to examine the prevalence of OTC statin use
in the general population of adults in England and to specifically characterise
whether this policy was filling professed need to address the treatment gap for
individuals at moderate coronary risk.
Methods
We undertook an analysis of the 2006 Health
Survey for England (HSE). The HSE is a yearly survey that is based on a
nationally representative probability sam-pling design. Each year the HSE
focuses on a separate topic area or group. Available data for this study are
found in the 2006 HSE which focused on cardiovascu-lar disease (CVD) and risk
factors.[12]
We limited this study to adults
aged 20 and older (unweighted n=10 007).
Variables
Use of statins
Participants were first asked: ‘Are you
taking or using any medicines, pills, syrups, ointments, puffers or
injections prescribed for you by a doctor?’ The nurse was then prompted: ‘If
statins have been prescribed by a doctor, please code them here. If they are
bought without a prescription, code at the statins question.’ A follow-up
question was included in the HSE which assessed acquisition of statins without
a prescription. The question was: ‘Are you taking statins (drugs to lower
cholesterol) bought over the counter from a pharmacist, without the
prescription of a doctor?’ Participants who bought statins over the counter
(OTC) were then asked: ‘Have you taken/used any statins in the last seven
days?’ Persons who had not used statins in the last seven days were excluded
from the OTC statin users group. Use of prescription medications was assessed
through a question asking for the patient’s current medications prescribed by a
doctor. Up to 22 different medicines were recorded for each person in the
HSE. Prescriptions for ‘lipid-regulating drugs’ were identified using the
British National Formulary code of 02.12.00.
Eligibility criteria for OTC simvastatin
We followed the practice guidance
information re-leased by the Royal Pharmaceutical Society of Great Britain
which allowed us to categorise the population into three groups:
1 individuals eligible for OTC simvastatin
2 individuals who should be
referred to a general practitioner because of higher risk of CHD or
contraindications for statins, and
3
individuals who
presumably do not warrant statin therapy.[13]
Persons eligible for OTC simvastatin
include any male between 55 and 70 years old, with or without a risk factor,
males between 45 and 54 years old with a risk factor, and females between 55
and 70 years old with a risk factor. Risk factors include current smoking or having quit
within the past five years, family history of cardiovascular disease
(operationalised as parent having angina, heart attack or stroke before age 55
years for a natural father and before age 65 years for a natural mother), body
mass index >25 kg/m2 and South Asian race/ethnicity. Persons who
should be referred to a GP include men 55 or more years old with a family
history of early heart disease and one other risk factor as outlined above;
persons with cardio-vascular disease including diabetes, angina, previous heart
attack, stroke and hypertension; persons tested and having high blood
cholesterol; and persons who drink alcohol on five or more days per week.
Patients who were currently on a prescribed statin were con-sidered to meet the
‘refer to a GP’ criteria. Individuals not meeting the criteria for either OTC
simvastin or being referred to a GP would presumably not require either OTC or
prescribed statin therapy.
Patient
characteristics
Both patients
that were OTC statin users and patients eligible for OTC statins were
characterised by age (20– 44, 45–64 and >65 years old), gender, race (white
versus non-white), income (<£15 000 or >£15 000) and edu-cation
(qualification or student versus no qualification). Patients in each group were
also characterised as to whether or not a doctor had told them that they had
high cholesterol, and whether they had high total serum cholesterol (<5
versus >5 mmol/l) according to the laboratory examination conducted during
the HSE.[14] Patients were considered disadvantaged if they had low
income, low education or were from an ethnic minority.
Analysis
We initially
computed the characteristics of the indi-viduals eligible for OTC simvastatin
therapy. We also computed the characteristics of individuals on OTC statin
therapy. We compared the differences between individuals meeting
different criteria and OTC statin use through chi square analysis. In
addition, we com-puted a logistic regression examining the relationship between
age, gender, disadvantaged status and OTC statin eligibility with receipt of
statins.
All analyses used the recommended weighting scheme outlined in the HSE
description.[13] Design variables were cluster and primary sampling
unit (PSU). The HSE 2006 is a random sample of 720 PSUs for the core sample and
468 PSUs for the child boost sample. For most analyses we used the nurse weight
to analyse demographics and questions asked during the nurse visit. The nurse
weight takes into account non-response to the nurse section of the survey. For
the total cholesterol results for the blood sample we used the blood weight as
recommended in the HSE User Guide.[15]
Results
In the HSE,
among the total adult population, 44.1% met the criteria to be referred to a GP
for CHD risk, 9.7% met the eligibility for OTC statins and 46.1% did not meet
the eligibility for prescribed or OTC statin therapy. In the population, less
than 1% (0.7%) were taking OTC statins. Among individuals eligible for OTC
statins, because of the eligibility categorisation, none had been told that
according to their most recent cholesterol test they had a high cholesterol,
yet 81.7% had total serum cholesterol of >5 mmol/l (Table 1). The proportion
of individuals using OTC statins among individuals eligible for them was
similar to the overall population, with only 0.2% taking OTC statins.
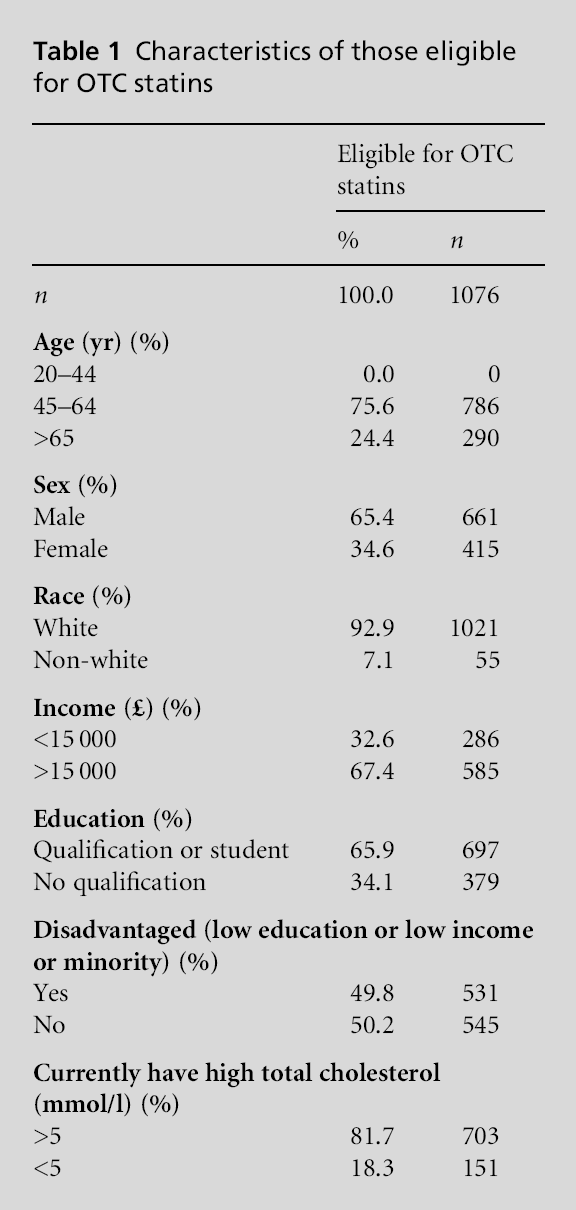
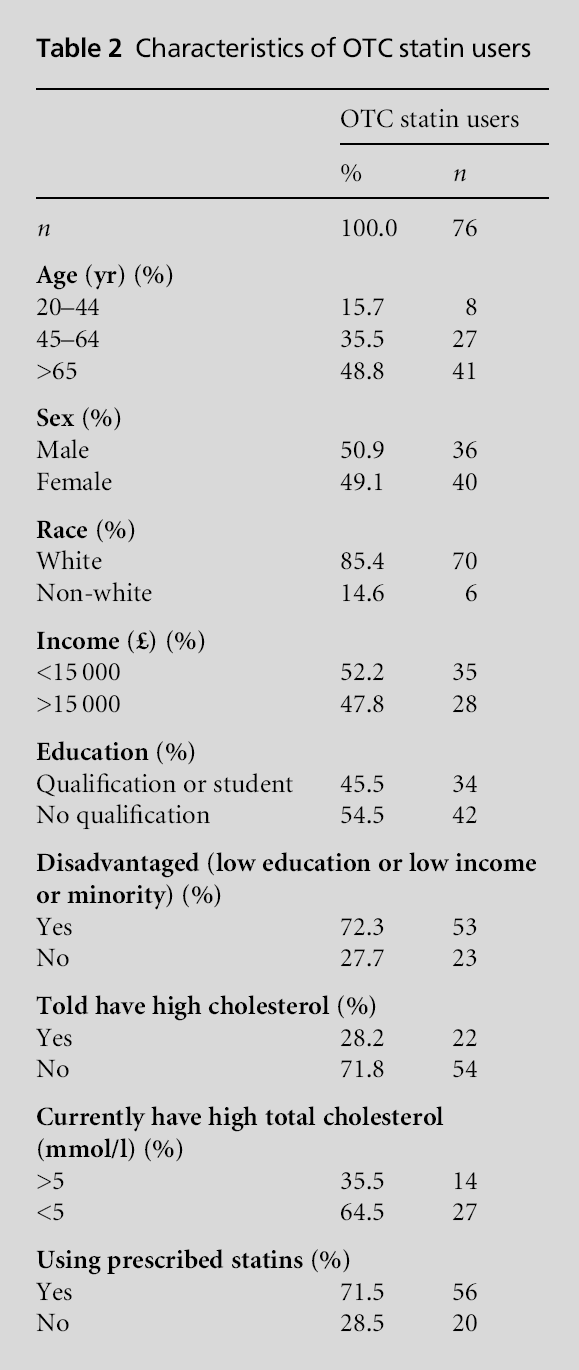
Table 2 presents the characteristics of individuals taking OTC statins.
Among those taking OTC statins 79.9% met the criteria for being referred to a
GP, 18.1% did not meet the criteria for statins and only 2.0% actually met the
criteria for eligibility for OTC statins (P<0.001). The use of prescribed
statins over-lapped with OTC statin use rather than these being two
different groups. Among those taking OTC statins 71.5% were also taking
prescribed lipid lowering agents. Looked at another way, among patients taking
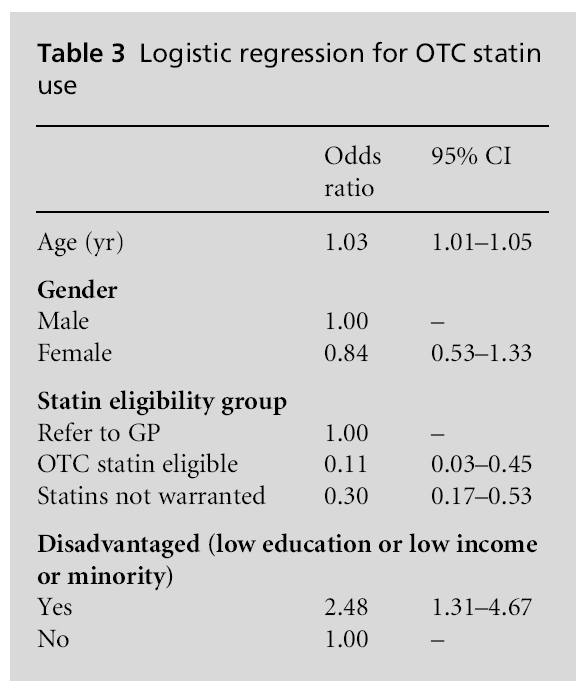
prescribed statins, 4.2% of patients also reported taking OTC statins. The
information in Table 3 indicates a significant relationship between
disadvantaged indi-viduals and OTC statin use independent of age, gender and
eligibility.
Discussion
The results suggest that the aim of
addressing the treatment gap among individuals at moderate risk by offering
access to OTC statins has not been achieved two years after the implementation
of the policy. Few individuals who are at risk are using OTC statins and the
majority of the individuals who are using OTC statins are either not among the
target population or are concurrently using prescribed lipid lowering agents.
While 81.7% of individuals eligible for OTC statins had high total serum
cholesterol at the time of the examination less than 1% of those eligible for
OTC statins were using them. OTC statins seem to be more of a supplement to
prescribed statins, rather than filling the needs of a different and
at-risk population.
The rationale for addressing the lack of treatment for a large group of
individuals at moderate risk for CHD who may benefit from statins appears to
have support. Nearly 10% of the adult population in England are eligible for
OTC statins but fewer than 1% of the eligible population get them. This lack of
use of OTC statins may be because the eligible patient population is not
getting the message from the healthcare sector that they are at risk for
cardiovascular disease and could benefit from treatment. Further, these
individ-uals may not consider the use of OTC medication worthwhile for a
chronic problem and may be more compliant with
physician prescriptions of medication. These data show that eligible
individuals have not been told that they have high cholesterol while 82% have
elevated total cholesterol. This suggests that this population may benefit from
wider use of statins. However, it is unclear whether OTC statins at such low
doses are a useful treatment because of a general lack of study of these doses
in large clinical trials.[16]
]
The introduction of OTC statins is another step in a process leading to
more self-medication by patients. Increasing the role of patients in medication
decisions and decreasing the role of physicians in the decisions may not be
warranted based on the present data. The current data indicate that the group
which should get the treatment is not receiving it and OTC statins are being
used by patients who are already prescribed statins. Further, in the OTC
eligible group, a substan-tial majority currently has high cholesterol but has
not been informed of this; thus they are unlikely to see themselves as having
this risk factor and may not make either lifestyle changes or get treatment.
These findings suggest that more rigorous detection of hyperlipi-daemia by the
healthcare system would be a more appropriate strategy than moving lipid
regulating treatment to OTC status. Whether this suggests a greater role for
pharmacists in the screening and risk assessment of patients remains to be
seen.
There are several limitations that must be con-sidered in this study.
First, these data are from 2006. Although this relatively short time frame
allows us to examine the impact of the policy two years after its
implementation the presented numbers may not be representative of current OTC
statin use. Second, the information regarding the use of OTC statins is self-reported
and may be affected by recall bias or con-fusion in remembering
medications. However, it is unlikely that the real rate of use would vary
twofold or more, thus the conclusions from the current report of low rates of
use of OTC statins by the eligible popu-lation are likely to be valid.
In conclusion, relatively few individuals who have the appropriate
cardiovascular risk characteristics are using OTC statins. Further, the
majority of the indi-viduals who are using OTC statins are not in the target
population for use of such agents. Further research is clearly needed to
evaluate the impact of current OTC statin policies and to determine how such
policies should be modified to improve the use of statins by the target at-risk
population.
References
- Rosamond W, Flegal K,
Friday G et al. Heart disease and stroke statistics – 2007 update: a report
from the American Heart Association Statistics Committee and Stroke Statistics
Subcommittee. Circulation 2007;115: e69–e171.
- Baigent C, Keech A, Kearney
PM et al. Cholesterol Treatment Trialists’ (CTT) Collaborators. Efficacy
and safety of cholesterol-lowering treatment prospective meta-analysis of data
from 90 056 participants in 14 randomised trials of statins. The Lancet 2005;366:1267–
78.
- Nag SS, Pearson TA, Ma
L et al. Estimating cholesterol treatment rates among individuals with multiple
risk factors and without coronary heart disease rates. American Journal of Cardiology 2005;95:862–4.
- Royal Pharmaceutical
Society of Great Britain. Practice Guidance: OTC simvastatin. 2004. www.rpsgb.org.uk/
pdfs/otcsimvastatincardguid.pdf (accessed
December 2008).
- Editorial. OTC statins:
a bad decision for public health. The Lancet 2004;363:1659.
- Tinetti ME. Over-the-counter
sales of statins and other drugs for asymptomatic conditions. New England Journal of Medicine 2008;358:2728–32.
- Rashid S. Should
cholesterol-lowering medications be available in Canada without a prescription? Canadian Journal of Cardiology 2007;23:189–93.
- Brass EP, Vassil T,
Replogle A et al. Can consumers self-select for appropriate use of an
over-the-counter statin? The Self
Evaluation of Lovastatin to Enhance Choles-terol Treatment Study. American Journal of Cardiology 2008;101:1448–55.
- Fuster V. A new
perspective on nonprescription statins: an opportunity for patient education
and involvement. American Journal of Cardiology 2007;100:907–10.
- Hanford D, Cunningham
S, John D, McCaig D and Stewart D. Community pharmacists’ views, attitudes and
early experiences of over-the-counter simvastatin. Pharmacy World and Science 2007;29:380–5.
- Filion KB, Delaney JAC,
Brophy JM, Ernst P and Suissa S. The impact of over-the-counter simvastatin on
the number of statin prescriptions in the United Kingdom: a view from the
General Practice Research Database. Pharmacoepidemiology and Drug Safety
2007;16:1–4.
- Practice Division of
the Royal Pharmaceutical Society of Great Britain. Practice Guidance: OTC
simvastatin. London: Royal Pharmaceutical Society of Great Britain, 2004.
- Craig R and Mindell J
(eds). Health Survey for England 2006. Volume 3: Methodology and documentation.
Leeds: The Information Centre, 2007.
- National Institute for
Health and Clinical Excellence (NICE). Lipid Modification: cardiovascular risk
assess-ment and the modification of blood lipids for the primary and secondary
prevention of cardiovascular disease. NICE Clinical Guideline 67. London: NICE,
2008.
- Anonymous. User Guide,
Health Survey for England 2006, Cardiovascular Disease and Risk Factors.
London: Joint Health Surveys Unit, National Centre for Social Research,
Department of Epidemiology and Public Health, University College London, 2006.
- Kizer JR, Madias C,
Wilner B et al. Relation of different measures of low-density lipoprotein
cholesterol to risk of coronary artery disease and death in a meta-regression
analysis of large-scale trials of statin therapy. American Journal of Cardiology 2010;105:1289–96.
Funding
This work was
supported in part by a grant from the Blue Cross and Blue Shield Foundation of
South Carolina.
Ethical Approval
This study was
approved by the Medical University of South Carolina Independent Review Board.
Peer Review
Not
commissioned; externally peer reviewed.
Conflicts of Interest
None.

