Key words
cultural competence, culture, mental health services research, participatory research
Introduction
Inequities in access, service quality and outcomes are pervasive, long-standing and well documented among individuals from diverse racial, ethnic and cultural backgrounds (United States Department of Health and Human Services, 2001). Discussing the omission of culture from mental healthcare in particular, the President’s New Freedom Commission’s Final Report (New Freedom Commission on Mental Health, 2003) noted that mental healthcare systems have failed to incorporate the histories, traditions, beliefs, values and language systems of culturally diverse groups, resulting in their having to shoulder a greater disability burden than their White peers. As a result of these findings, the subsequent Substance Abuse Mental Health Services Administration (SAMHSA) Federal Action Agenda (United States Department of Health and Human Services, 2005) follows the lead of other federal reports and panels (e.g. United States Department of Health and Human Services, 2001) which recommend the identification and elimination of healthcare disparities as a major goal for the foreseeable future.
In addition to recruiting a more culturally diverse workforce, increasing cultural competence is frequently cited as an important strategy for eliminating disparities (Evans et al, 2005). As part of its initiative to increase cultural competence across the state-wide system of care, the Office of Multicultural Affairs of the Connecticut Department of Mental Health and Addiction Services contracted with the Yale Program for Recovery and Community Health to conduct a series of focus groups to explore service users’ views of how culture is and is not incorporated in their care and what they would recommend to make services more culturally responsive. In accord with the principles of participatory research (Wallcraft et al, 2009), both the focus groups and the analysis of focus group responses were carried out by teams of researchers and service users, who were trained in qualitative methods, as part of a state-wide Consumer Research and Evaluation Network. This article summarises the findings of these focus groups and discusses service users’ suggestions for creating a more culturally responsive behavioural healthcare system.
The research questions were as follows:
1 What is it like to be part of a particular cultural group?
Methods
This research, including participatory data analytic strategies, was approved by both the Yale University Human Investigation Committee and the Connecticut Department of Mental Health and Addiction Services Institutional Review Board. All of the participants in the focus groups and data analysis groups gave their consent to participate.
Study population
The participants in this research were consumers at state-operated and non-profit mental health and substance abuse agencies that are funded by theConnecticut (CT) Department of Mental Health and Addiction Services (DMHAS). The Commissioner of CT DMHAS wrote a memo to all state and non-profit agencies asking them to hold focus group discussions about consumers’ experiences of culturally competent care. Culturally homogeneous focus groups were conducted at various state agencies depending on whether they served particular cultural/ethnic groups (e.g. African American, Latinos) or populations (e.g. young adults), or had an active special-interest group (e.g. with regard to sexuality or sexual orientation). Focus groups were also conducted at the state-operated mental hospital. Once a focus group for a particular cultural group had been scheduled at an agency, it was advertised using flyers, and clinicians were requested to issue invitations to all clients who were part of the cultural group concerned. This request was made in order to prevent bias in the sample. In total, 22 focus groups were facilitated across the state, consisting of African Americans (7 groups), Latino Americans (6 groups; see Box 1), White Americans (3 groups), Asian (Cambodian) Americans (2 groups), young adults (1 group), lesbian, gay, bisexual, transgender, queer, intersex (LGBTQI) individuals (2 groups), and a culturally mixed group. Nine to ten individuals attended each group, giving a total of 210 participants.
Procedure
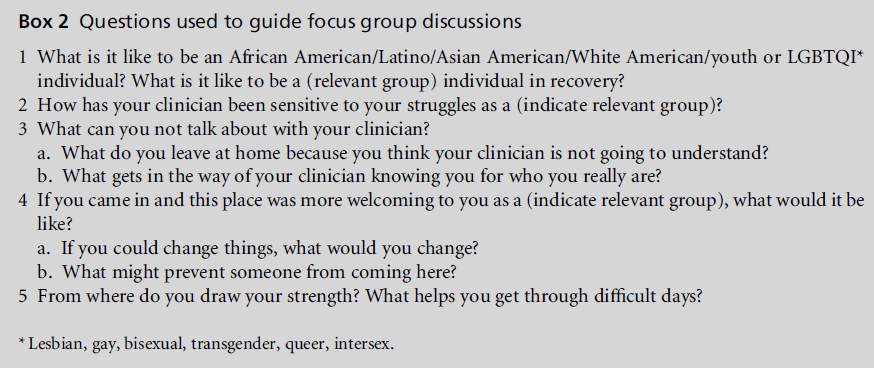
Focus groups were 1 to 2 hours in length and were digitally recorded and transcribed verbatim (see Box 2). Focus groups with Latino Americans were conducted in Spanish and were translated, transcribed and analysed in English. The focus group with Cambodian refugees was conducted with an interpreter present.
Verbal consent was obtained and participants were informed that personally identifying information would not be collected or reported in written summaries of aggregated findings. They were also assured that, if any content discussed during focus groups was potentially identifying, this information would be disguised in order to ensure anonymity.
Given the diversity of groups assessed in the research, we decided to conduct a preset number of focus groups with various cultural groups in the CT DMHAS system based on agency availability, rather than conducting focus groups until saturation was achieved.
Data analysis
People with lived experience of psychiatric disorders and indigenous knowledge of ethnic and sexual orientation diversity were recruited to work on this project, as part of a developing Consumer Research and Evaluation Network (CREN). They received a half-day basic training in the theory and techniques of qualitative data analysis, particularly content analysis (Charmaz, 2006; Weber, 1990). This training included working individually and as a group, with raw data from focus group transcripts, to identify and conduct open coding for important themes (Strauss, 1987). Prior to analysing the focus group transcripts, in order to increase the potential for trustworthiness and to build consistency in inter-investigator coding, trainees all coded one long excerpt from a single source and reviewed the work as a group. The consumer/family researchers were then teamed in a small group with one or more experienced qualitative researchers. Each team member independently read the same transcript(s) and coded for themes. They then met in small groups from three to five times to review the individual codings and come to a consensus about an integrated set of themes, identify segments of transcripts that exemplified the themes, and discuss short narratives within the transcripts that illustrated the theme. Finally, a one-day workshop was conducted to involve the teams in looking across all of the transcripts and analyses in order to develop a shared or overarching set of inductively derived themes (Krippendorf, 1980).
Results
Data analysis generated seven overarching themes, namely positive experiences with care, the barriers and bridges to trust, issues not discussed in treatment, stereotyping and negative experiences of care, language issues, persistent self-advocacy as a means of getting needs met, and clinician and agency recommendations. Within each theme, a number of sub-themes were identified; these are discussed within the presentation of each theme.
Positive experiences of care
Participants in many groups reported satisfaction with services and positive feelings about care. They described feeling listened to and understood by their clinicians, and many reported that they were ‘getting things done.’ A prominent sub-theme was that many participants who reported satisfaction with care also reported receiving services from ethnically and/or culturally similar programmes or providers:
This group helps too, the leaders are black and they understand us and we understand them too. I like coming here. It’s peaceful and gives me more experience talking to other people. I wish we could meet for two hours instead of once a week. They help us get things done and so does my therapist. Like the other day I was crying because I got laid off frommyjob and I toldmytherapist and she helped me find another job the next day. I am very happy. It’s going to work out real good for me. I’ve come a long way after getting clean. If it wasn’t for programmes like this I’d be in the gutter somewhere. But I’ve got faith now and confidence. I can never go back to where I was before.
(African-American woman, African-American group)
Similarly, a participant who sought services at an organisation with a number of bilingual/bicultural Latino American clinicians noted:
I feel appreciative of the help that they have given us here in this clinic because without it, I think that without this clinic we wouldn’t survive. It is very important in our lives, well at least in mine. This clinic is very important in my life.
(Hispanic participant)
Participants who received care from ethnically or culturally specific programmes reported a number of specific factors that contributed to their positive experiences. These included feeling as if they were working in partnership with their clinicians to achieve goals, feeling as if clinicians were ‘opening doors’ for them, feeling that their clinicians respected and cared about them, believing that service providers understood their cultural background, and feeling that they could talk about anything with their providers. Addressing several of these areas, one participant, who was being seen by an ethnically similar African- American provider, noted:
I like the clinician I have now, because she treats me as a human being. I can talk to her about anything, and I can see that she is listening and that she is concerned. She gives me feedback and whatnot and I can say things you can’t say to another one. I mean, you can say things that you can’t say to another person, you know, not African- American. So I try with my clinician – we’re real, real, real locked in. I’ve come here for depression. I’ve had a lot of help and it’s been a while since I’ve been in that depressed state, so I’m very thankful to God for these people, because I feel that I got the help I needed.
(African-American participant)
Although the majority of the participants who were receiving care from culturally similar providers reported a range of positive experiences of care, there were instances of positive experiences with culturally dissimilar providers. For instance, one participant of Latino origin reported satisfaction with services, noting that his non-Latino provider showed professionalism and worked hard to support his recovery:
In my case the therapist I have, I am not going to say names, is not Hispanic, because she’s not like us Hispanics, but she does find the way, and all the means to try to find an effective treatment for the persons she treats. I think that the same treatment of cordiality that she gives me and the same way she finds to help me get better, I imagine she gives to the rest. Because I cannot vote for the rest, but I think that I am satisfied and I think that although she is not Hispanic, she tries to give the maximum so that people will recover. To me she is a tremendous professional in her profession.
(Hispanic participant)
Other participants spoke positively of aWhite American psychiatrist who was highly sought after and well liked by many service users of Cambodian descent. They praised the psychiatrist’s dedication, his flexibility with time, his willingness to make home visits, and his efforts to learn about and understand their culture, including a visit to a refugee camp in Cambodia. They felt comfortable talking about their experiences of trauma under Communist rule, knowing that he had been to Cambodia and had seen some of the places that they described.When discussing their experiences of feeling listened to and understood, a member of staff in one programme, who was also a refugee camp survivor, reported:
Yes, he understands their experience. Yes, from their point of view, because he went to the [refugee] camp. Basically, he was at the house a long time ago where they were in the camp and he understands where they’re coming from, what they have gone through. And he listens instead of giving them ‘OK, here’s the medication. You can take this. Here’s the medication, take that.’ He listens.
(Asian-American participant)
Bridges and barriers to trust
In all of the focus groups the participants discussed a variety of factors that either fostered or impeded the development of trust and a positive working relationship with providers. A lack of confidentiality was noted as one such factor. Participants raised concerns about whether the information they gave to providers would be used against them:
Whether the clinician is black or white it don’t matter which colour he is first you have to trust. And then you still won’t come clean because of what they put down in your record. Whatever you say, they hold against you. So now you have to think, I want to talk to this guy, but some things that I say he is going to hold it against me.
(African-American participant)
Participants also raised concerns about personal information being shared in meetings with other providers:
I used to go to another place for depression, and I had trouble with this counsellor with something very, very personal. She went and told the other counsellor, and I could tell because of the way they looked at me or I read their body language and how they would be like smiling and stuff. I asked her if she had spoken about this. ‘Oh, we were just in a’ you know, their meeting. Still I felt that she shouldn’t have even said it to them. That caused me to yeah, I wouldn’t tell any of these counsellors, especially something personal, personal. I wouldn’t do that.
(African-American participant)
Another impediment to the development of trust was providers being too strict about rules. Participants described some providers as being more interested in exercising their power or satisfying their supervisors than in helping the people they were supposed to be serving. One participant told a poignant story of a situation in which he was sick and missed work because he had to go to the hospital to get medication for a sinus infection. The next day he woke up early to be able to take his medication and sign out in order to get to work by 7.00 am. However, when he went to the front desk his paperworkwas not there so he could not leave:
So they called the Director and the Director called back and said ‘Wait until seven.’ But at seven I have to be at work. When I called work they told me ‘Forget it, if you can’t be here by seven forget about the job.’ It didn’t pay a lot. I had to take two buses and walk a half hour. I would get there out of breath. Punch in at a minute to seven. But I wanted to make a few dollars for when I get out of here. That Friday I was going to be on leave too. I had put in for a request for some money that is mine, that is here being stored. When I went to tell the Director he says ‘No, we can’t give you that amount of money because you are no longer working.’ So I got a little mad and said ‘I lostmyjob because of you guys and now you’re going to tell me you can’t give me the usual amount of money today. But that’s my money and I lost my job because of negligence here. I was awake at 4.30 am.’ They can be so strict.
(Hispanic participant)
Another participant recalled a similar situation in which he was given a pass by his provider to leave the facility to obtain a prescription for medication. He went to his usual place, rather than the one that was indicated on the pass. When he returned with his medication, he was reprimanded for going to the wrong place and his provider filled out paperwork for him to go 21 days without a pass as punishment for going to the wrong place. Discussing how he felt about this situation, he stated:
So I got mad, but it’s likemyfriend here said, when you get mad, you have to keep it all inside, and when I get to the room I explode like a balloon. I was thinking about it and saying ‘Wow, this guy is wrong.’ How is he going to give me 21 days and tell another ‘I sent him to one place and he went to another, you know?’ He should have said ‘Well, I didn’t send you there. But you are showing me this as proof, so let’s leave it there and it’s between us. But next time when I send you somewhere go there’ He didn’t say ‘You OK?’ or anything. He only said ‘You didn’t go where I’d sent you.’ So I said ‘Wow, this guy isn’t here to help me then. He’s just here to bother me.’
(Hispanic participant)
Participants stated that a provider’s willingness to bend the rules, even a little, would help to establish trust and communicate a willingness to be helpful. In turn, this would encourage participants to open up to providers and share more in sessions. Discussing the experience quoted above, one participant commented that, with a more flexible approach, providers could say:
‘Look, I’m going to do this for you’ [and so] gain the trust of the person who doesn’t speak up, with that he would open up with the counsellor because he would say ‘Wow, he did this for me. Well, I have this problem and I haven’t spoken to you about this, but I now see you want to help me.’ If I see he wants to help me, I am going to open up more to him.
(Hispanic participant)
For many participants, cultural similarity facilitated the development of trust, in addition to a range of other positive care experiences as discussed in the previous theme. As one participant noted:
When there’s a program that doesn’t have a Hispanic counsellor, one feels deprived of saying what’s going on, but when there is a Hispanic counsellor, you feel more trust in talking to him. An American isn’t going to treat you the way a Hispanic is going to treat you.
(Hispanic participant)
Similarly, another participant noted:
My clinician, by her being white, I can’t open up and tell her how the black experience goes, you know, how proud I am to be a black man, how it feels to be in a black man’s shoes or a black woman’s shoes, things like that. I don’t care how much I think I trust her, I can’t I don’t trust her that way.
(African-American participant)
Issues not discussed in treatment
Some participants talked about the importance of not leaving anything at the door, not being ashamed of anything that they had done, because talking with a provider could help them to grow and feel better:
If there’s something that bad that I need to leave on the bed, I mean, he might help me to get it off there. I believe that in order for me to continue to grow, I have to let everything go and have trust in people.
(Hispanic participant)
However, in the majority of the focus groups, participants reported that they did not disclose a variety of issues to their providers. Their decisions not to disclose were directly related to the previous theme of trust and the degree to which they felt understood by their providers. This was particularly true for African- American participants who consistently reported that they did not discuss race or race-related issues:
Well, in other words, you can talk to your therapist about a lot of things, but when it comes to a race issue, then that’s taboo.
(African-American participant)
Many of the participants agreed, and reported similar experiences:
I discuss more of how can we get things done as far as my situation, as far as my housing, my social security, bills that need to be paid, how my depression is coming along. As far as being African-American and race, we never really discuss that.
(African-American participant)
In one exchange, and with a hint of surprise, several participants noted that they had never been asked about racial issues or their community:
I don’t remember any of them ever asking that question, how do it affect me as being an African-American or what’s going on in our community or whatever that’s where you could talk about some things that’s really, say, going on with us or in our neighbourhood, because we are involved in it. We are African American.
(African-American participant)
Many of the participants did not believe that service providers understood their experiences. This contributed both to their not wanting to talk about them and to their beliefs that the providers would not be able to help. Discussing these issues, one participant stated:
I think they wouldn’t really understand, because they don’t live in this community. They don’t live in the [neighbour]hood. They don’t live where we live at. So a lot of things I can’t really talk to them about, because they wouldn’t understand. It’s like we’re separated.
(African-American participant)
Participants discussed a number of neighbourhoodrelated and other experiences that they did not discuss in treatment, including violence, death of family members and young people, trying to get away from drug dealers, how White police officers ‘beat our kids and get away with it’, gang networks and experiences, being stereotyped and degraded when dealing with children’s schools, experiences of prejudice and racism when dealing with court systems and healthcare systems, employment, and other day-to-day experiences. Discussing how many of these issues were not addressed in care, one participant stated:
I think the services are OK, right, but do they get to the core of the matter about how things truly affect the community we live in? Not even a drop. Not even a drop in the bucket.
(African-American participant)
Participants in all of the other focus groups discussed a variety of additional issues that they did not disclose during treatment, including sexual relationships, the experience of being raped or molested, the experience of domestic violence in the past, buying or selling drugs, what it felt like to experience language barriers, and a range of LGBTQI issues. Many African-American and Latino participants noted that they were raised to believe that ‘what happens at home, stays at home’, and therefore it was not appropriate to discuss family matters outside the home. Furthermore, many young people talked about not wanting to open up and share personal information, as they did not want to be left vulnerable, particularly given the high staff and case manager turnover rates. Frequently switching providers discouraged them from opening up to or relying on providers who were likely to leave soon.
Stereotyping and negative experiences of care
Participants in most of the focus groups reported a number of negative experiences of care in which they felt stereotyped, disrespected or dismissed. These experiences were similar to those encountered in the broader society; hospitals and healthcare systems were a microcosm of the broader society, and, given this, participants were not surprised by their negative care experiences in these contexts. Discussing parallels between service systems and the broader society, one participant noted:
I’ve been here for seven years and I will say that this is a micro, microcosm of our larger society. You’re going to deal with racism in the larger society. You’re going to deal with racism here. We live in a society where people are not equal. I mean, a large society is not supposed to be racist, shouldn’t be racist, but it is.
(African-American participant)
Other participants reported feeling quite surprised, or even stunned, by their negative experiences, which evoked a range of emotional responses, including ‘stuffing’ their feelings, getting mad but not showing anger because they feared retaliation, going to their room and ‘exploding like a balloon,’ or working harder not to ‘be’ the stereotype. They speculated about the possible reasons for their provider’s behaviour, perhaps in an effort to make sense of these unexpected experiences. Illustrating many of these sub-themes, one person discussed a situation in which he was stereotyped for being in a gang as a result of his personal grooming:
One time I had a do-rag and they all jumped back and they were ready to arrest me. And they said ‘What is that on? Are you in some type of gang? Are you acting like those gangs out there, those black guys in the gangs?’ I said ‘No, you’ve got it wrong. You need to take some courses on African-American culture and behaviour. When black men groom, they always brush their hair’, and they had this blank look on their face, like ‘What is he talking about? He’s got an attitude.’ They are uneducated about African-American males the way they dress, their gait, their walk, the way they talk with their hands. They are very intimidated any type of aggressive activity I’m an alpha black male any type of aggression or assertiveness is viewed as hostility.
(African-American participant)
Many participants identified similar situations in which they felt stereotyped by service providers. For example, they believed that their medical records ‘followed them around’ and this contributed to their being judged by their past. Discussing this, one participant stated:
Get to know who I am not. They look at my report and that is all they see.
(African-American participant)
Others talked about feeling marginalised in society and having multiple strikes against them when applying for a job:
Strike one, to me, is being black. Strike two is coming out of jail. So, strike three is being black, coming out of jail, and out of a programme.
(African-American participant)
One participant shared an experience in which she felt both stereotyped as an African-American woman and betrayed by her service provider. When her mother passed away she relapsed after being clean for about a year. When she disclosed to her service provider of 15 years that she was drinking again, her provider asked her what she had to sell in order to use. Although the provider did not specify what she might have sold, the participant noted that she was hurt by the question and believed that the provider insinuated something negative that she sold her body or her furniture or something else to pay for alcohol. In discussing how she felt about this encounter, she stated:
It did something to me, but I’m the type of person that I’ll stuff it. I won’t say nothing. But it really did something to me, she knew all three of my kids, even my two oldest children who are adults, since they were small. My 15- year-old, she knew me before he was even born. She was my therapist. And she turned around and made another statement that the only time I can stay sober is if I’m on probation. She did that in front of everybody. I stuffed it. I didn’t get indignant. I didn’t respond. I just took it, and it hurt me. And not only was I humiliated, but there were men in this room when she made them comments to me. Somebody told me it’s just a job to her now. It’s just a pay cheque. Her compassion is gone.
(African-American participant)
In addition to reports of feeling stereotyped and disrespected, participants discussed a range of experiences in which they felt care was not useful, their expressions of distress were misunderstood, they felt invisible or their providers were disrespectful. For instance, many participants of Latino origin discussed how common cultural experiences or expressions of stress were often misunderstood, and how this contributed to their feeling labelled and stigmatised. One participant, who was also a peer counsellor, stated that:
you tell the doctor, ‘doctor, last night I saw my grandmother who died five years ago and she came to visit me.’ For us Hispanics that’s common, you know. A dream or something is not strange for us. But the psychiatrist is going to say ‘That person is hearing voices, is having hallucinations, he’s psychotic, let’s send him to the hospital.’ Or they get incorrect diagnosis.
(Hispanic participant)
Language issues
Language barriers emerged as a prominent theme in all of the focus groups conducted with individuals of Latino origin. Latino participants discussed the frustrations and difficulties they experienced when participating in treatment services that were offered only in English. Their inability to communicate with providers contributed to feelings of isolation, loneliness, depression and anger, and formany individuals resulted in their feeling as if they were being ‘choked out of the system.’ One participant shared an experience that summarised well several of these themes:
I spent 24 hours a day sleeping because they gave us therapy, but it was all in English. So I would take a pill in the morning and go to the room to sleep. I’d have breakfast and go to sleep at noon. Then they’d call us for lunch and then I’d take another pill, so I slept 24 hours a day for seven days. Everyone spoke in English and I would try to speak with my little English and they didn’t understand me. Even to ask for a fork I had to draw a picture. So, I’m depressed, I’m sick, but I get more depressed because it’s a barrier and they can’t help you.
(Hispanic participant)
Expressing similar concerns, another participant stated that he would rather wait for services that were offered in Spanish, because participating in services in English would be a waste of his time and would make him feel even worse:
I’m going to go in and leave worse than when I came in because they sent me to a place I wasn’t helped. I would rather wait for a programme where I can get involved and tell them ‘I have this problem. I have this emergency with my family or I have this situation, how can you help me? What are my benefits here, how can you help me? What does this programme give me so that I can come out doing well?’ If I don’t have language, I can’t do it.
(Hispanic participant)
Participants of Latino origin expressed preferences about interpreters. Some preferred not to use interpreters because they did not want to share confidential information with a third person who was not their provider. Others wanted Spanish-speaking interpreters present in the room with them during treatment; they did not want to use a telephone interpreting service. Moreover, it was not enough for providers or interpreters to speak Spanish. They also had to be both bilingual and bicultural, because understanding the culture was essential in providing help. A shared culture meant that providers could identify with clients, and clients themselves could express feelings that were difficult to express in English. Discussing these sub-themes, one participant stated:
There are times I don’t participate because the girls who run the programme are American. I speak very good English and I could identify with people speaking English, but there’s times I would like to express in my own language and I’m not able to do this because I don’t have a Hispanic clinician. There are a lot of things I would like to express in my own language that I cannot express in English.
(Hispanic participant)
Persistent self-advocacy as a means of getting needs met
Participants in all of the focus groups discussed a number of experiences in which they exercised persistence, voice or self-advocacy as a means of getting their needs met. For many, the need to engage in selfadvocacy emerged from situations in which they felt that providers either were not listening to them or were suggesting recommendations that did not suit them. For instance, one participant discussed an experience in which she was depressed and had physical health challenges, but her provider only attended to her housing needs. She felt that, by not addressing her emotional needs, her provider had pushed her away. Consequently, she decided to change providers:
I had a problem with living somewhere, and her first response was ‘I’m going to get you over there into the old WYMCA.After we get you situated with that, we’ll get you some food stamps.’ She actually said ‘That’s about the best I can do.’ She didn’t even want to work with me on my problem. She didn’t want to deal with the emotional problems. She figured that would solve it I was just another case to her, another black woman in trouble. I was sitting here major depressed, and she’s trying to tell me I had to go to some place I don’t even know.
(African-American participant)
For many participants, persistence in speaking up was an important part of getting the help that they needed. They believed that, if they expressed their needs consistently enough, and with intense emotion if necessary, the providers would eventually listen. One participant described a situation in which she wanted to be assigned to a new psychiatrist because she felt that the practitioner whom she was currently seeing had insulted her and was not addressing her concerns about medication, but reassignment did not take place until she ‘exploded and rebelled’:
I had to really explode and rebel. Then it happened. I finally got what I needed. I know what works for me and what doesn’t. I’ve been on this road with this bipolar thing since I was 26 years old. If anybody could tell you anything, it’s me. Listen to me. If you don’t listen because you know more than me, you got an education, that ain’t going to work. I’m happier when I have done something I know is right for me. I’m not miserable like I used to be.
(African-American participant)
Other participants reported many similar situations, adding that they persisted because they were trying to advance their recovery, and despite that fact that they sensed that the providers did not like them asking questions or pushing for their needs to be met.
Clinician and agency recommendations
In all of the focus groups, participants offered a range of recommendations that cluster into seven different areas, which are summarised in Table 1.
Discussion
The findings of this research highlight the complex and dynamic roles of race, ethnicity and culture in the helping relationship and in the development of services and systems that are responsive to the worldviews and values of diverse groups. Many of these findings are not new. Rather they echo previous research which has analysed the interaction of macro and micro levels of discrimination that affect health outcomes (e.g. Dovidio et al, 2008; Waldro, 2010). Many of the negative experiences reported here reflect similar themes in the national cultural competence and healthcare literature (e.g. Smedley et al, 2003). Thus themes that suggest racism, bias and discrimination are not unique to the north-east, but rather they mirror social patterns that have challenged healthcare and US culture in general for generations (Byrd, 1990; Hankin and Wright, 2010; Hollar, 2001; Sabshin et al, 1970; Saha, 2008) as well as healthcare globally (Gilburt et al, 2008; Hussey et al, 2008). Recent articles have also suggested that some forms of discrimination, such as coercion, might be more a part of the setting, such as the involuntary detention of psychiatric inpatients, than race/ethnicity (Bennewith et al, 2010).
Table 1: Clinician and agency recommendations
Nevertheless, these themes represent an important call to action. What is needed is the designing of unique and creative interventions to enhance attention to culture and service equity (Chin et al, 2007; Smith et al, 2007) and to offer care that is in harmony with individuals’ cultural beliefs, practices and values (Leininger and McFarland, 2006). Many of the recommendations offered by service users highlight possible system innovations, which reflects the assertions put forward in the recovery literature that, when asked, service users know what works for them (Mead and Copeland, 2000). Although it may not be feasible to implement them all simultaneously within a given system, some could be introduced with limited effort and/or cost, for example, enquiring about a person’s racial, ethnic or cultural background.
A comprehensive discussion of every recommendation offered by the service users is beyond the scope of this article, but two overarching themes will be examined here.
Provider and system strengths
Several provider and system strengths were reported, many of which are discussed in the broader multicultural literature as key competencies for working with diverse groups. Such strengths include providers’ abilities to understand their clients’ cultural backgrounds, to demonstrate respect and genuine compassion, to listen, to be flexible with time, and to speak in their clients’ primary language. Positive experiences were reported by participants treated by individuals who were ethnically similar and ethnically dissimilar, which indicates that ethnic matching alone does not translate to positive outcomes (Cabral, 2011). This suggests that the cultural sensitivity of providers is more likely to predict positive care experiences and outcomes (Maramba and Hall, 2002). From an organisational and system perspective, these findings also suggest that, although ethnically similar providers and programmes may be useful, others may also be helpful if they implement multicultural care practices (American Psychological Association, 2003). Provision of ongoing cultural competence education and training can help to improve providers’ skills in working with diverse groups (Smith et al, 2007).
Service users expressed an interest in being involved in interventions to improve care, offering such recommendations as the need for more peer-to-peer programmes and for service users to be involved in training providers. Involving service users in the development and implementation of training for providers could lead to the development of innovative training and education approaches, such as the use of recovery and culture narratives as a means of ensuring that important nuances of culture and recovery-oriented care are addressed.
The development of peer-to-peer programmes can serve as a cost-effective strategy for providing service users with additional support, and enable individuals to understand the process of receiving care, especially if the accessing of behavioural health services is not a traditional form of help seeking in their culture. Moreover, working with a peer mentor can help an individual to feel socially connected, understood and supported. In turn, such benefits can increase that person’s engagement in services and thus improve outcomes, and reduce recidivism rates and system costs. Increasing peer services and supports can also help to address language barriers. One cost-effective strategy for enhancing language assistance services would be to train bilingual/bicultural peers in translation services and hire them to provide this service.
System challenge and growth areas
Negative experiences formed a prominent theme in this research. They represent significant system challenges and the need for intervention. For instance, participants felt that service providers stereotyped them and did not understand their culture. These two factors undermined the development of trust and participants’ willingness to share cultural and other experiences that were having an impact on their lives. Such findings suggest that there is a need for providers to ask directly about important areas of culture that may influence a person’s life, as a means of enhancing trust and engagement in care. The use of such guides as the Cultural Formulation in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) (American Psychiatric Association, 2000), or other assessment tools that directly address cultural identity, language preferences, experiences of racism and discrimination, migration history, trauma, and cultural beliefs about mental health and formal help seeking, is also needed. Asking about culture and race can help to communicate cultural understanding and convey the important message that these are not taboo topics for therapy, but rather that they are important to discuss, particularly in instances where racial, ethnic or cultural issues are contributing to the distress in a person’s life.
Study limitations
There were several limitations to this study. First, focus groups were selected for data collection in order to gather experiences from a wide variety of participants. Although facilitators were trained to honour individual perspectives and not to encourage groups to come to a consensus, it is possible that some individual perspectives were compromised. Secondly, focus groups were planned and recruited only at CT DMHAS facilities that were willing to host them, which may also have limited the variety of opinions available.
Conclusion
Thirdly, given the large number of focus groups conducted and the large number of themes identified, the emphasis was on themes that were similar across groups, rather than on outlying or dissenting opinions. Fourthly, detailed sociodemographic information about the sample was limited, as some focus group facilitators did not return the data collection forms detailing the demographics of their focus group participants. Finally, another limitation of this paper is the uniquely US focus of this inquiry, which investigated a US system of care and focused on minority populations prominent in the USA, namely Latinos (Hispanic) and African Americans. The literature cited in this discussion also focuses on cultural competence as it is understood and conducted in the USA.
Conclusion
CT DMHAS is to be commended on its willingness to ask difficult questions and engage in self-reflection about the role of culture in the service delivery process. Undertaking this evaluative work speaks to the state’s long-standing commitment to creating a system of care that is responsive to the cultural values and needs of all individuals. Working in full partnership with service users, a critical next step will be to further develop and prioritise the recommendations offered, in an effort to improve attention to culture and service delivery outcomes for all individuals seeking care.
Acknowledgments
This research was funded by the Connecticut Department of Mental Health and Addiction Services, Office of Multicultural Affairs.
Tables at a glance

Table 1
Box 1
Box 2
References
- American Psychiatric Association (2000) Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR). Washington, DC: American Psychiatric Association.
- American Psychological Association (2003) Guidelines on multicultural education, training, research, practice and organizational change for psychologists. American Psychologist 58:377–402.
- Bennewith O, Amos T, Lewis G et al (2010) Ethnicity and coercion among involuntarily detained psychiatric inpatients. British Journal of Psychiatry 196:75–6.
- ByrdWM(1990) Race, biology, and health care: reassessing a relationship. Journal of Health Care for the Poor and Underserved 1:278–96.
- Cabral RR (2011) Racial/ethnic matching of clients and therapists in mental health services: a meta-analytic review of preferences, perceptions, and outcomes. Journal of Counseling Psychology 58:537.
- CharmazK(2006) Constructing Grounded Theory: a practical guide through qualitative analysis. Thousand Oaks, CA: Sage Publications. Chin MH, Walters AE, Cook SC et al (2007) Interventions to reduce racial and ethnic disparities in health care. Medical Care Research and Review 64(5 Suppl.):7–28S.
- Dovidio JF, Penner LA, Albrecht TL et al (2008) Disparities and distrust: the implications of psychological processes for understanding racial disparities in health and health care. Social Science and Medicine 67:478–86.
- Evans AC, Delphin ME, Simmons R et al (2005) Developing a framework for culturally competent systems of care. In: RT Carter (ed.) Handbook of Racial Cultural Psychology and Counseling, Training and Practice. New York: John Wiley & Sons. pp. 492–513.
- Gilburt H, Rose D and Slade M (2008) The importance of relationships in mental health care: a qualitative study of service users’ experiences of psychiatric hospital admission in the UK. BMC Health Services Research 8:92.
- Hankin JR and Wright ER (2010) Reflections on fifty years of medical sociology. Journal of Health and Social Behavior 51(1 Suppl):S10–14.
- Hollar M (2001) The impact of racism on the delivery of healthcare and mental health services. Psychological Quarterly 72:337–45.
- Hussey P, Anderson G, Berthelot J et al (2008) Trends in socioeconomic disparities in health care quality in four countries. International Journal for Quality in Health Care 20:53–61.
- KrippendorfK(1980) Content Analysis: an introduction to its methodology. Beverly Hills, CA: Sage Publications.
- Leininger MM and McFarland MR (Eds) (2006) Cultural Care Diversity and Universality: a worldwide nursing theory. Sudbury, MA: Jones and Bartlett Publishers, Inc.
- Maramba GG and Hall GC (2002) Meta-analysis of ethnic match as a predictor of dropout, utilization, and level of functioning. Cultural Diversity and Ethnic Minority Psychology 8:290–97.
- Mead S and Copeland ME (2000) What recovery means to us: consumer perspectives. Community Mental Health Journal 36:315–28.
- New Freedom Commission on Mental Health (2003) Achieving the Promise: transforming mental health care in America. Rockville, MD: Substance Abuse and Mental Health Services Administration.
- Sabshin M, Diesenhaus H and Wilkerson R (1970) Dimensions of institutional racism in psychiatry. American Journal of Psychiatry 127:87–93.
- Saha S (2008) Racial and ethnic disparities in the VA health care system: a systematic review. Journal of General Internal Medicine 23:654.
- Smedley B, Stith A and Nelson A (2003) Unequal Treatment: confronting racial and ethnic disparities in health care. Washington, DC: Institute of Medicine, National Academies Press.
- Smith WR, Betancourt JR, Wynia MK et al (2007) Recommendations for teaching about racial and ethnic disparities in health and health care. Annals of Internal Medicine 147:654–65.
- Strauss A (1987) Qualitative Analysis for Social Scientists. Cambridge: Cambridge University Press. United States Department of Health and Human Services (2001) Mental Health: culture, race, and ethnicity. A Supplement to Mental Health: A Report of the Surgeon General. Rockville, MD: US Department of Health andHuman Services, Public Health Service, Office of the Surgeon General.
- United States Department of Health and Human Services (2005) Transforming Mental Health Care in America. The Federal Action Agenda: first steps. Rockville, MD: US Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Mental Health Services, National Institutes of Health, National Institute of Mental Health.
- Waldro I (2010) The impact of inequality on health in Canada: a multi-dimensional framework. Diversity in Health and Care 7:261–70. `
- Wallcraft J, Amering M and Schrank B (eds) (2009) Handbook of Service User Involvement in Mental Health Research. Chichester: John Wiley & Sons.
- Weber RP (1990) Basic Content Analysis (2e). Newbury Park, CA: Sage Publications.


