Keywords
Pancreas; Pancreatitis (classification; etiology; genetics; history; immunology; therapy) Pancreatitis, Alcoholic; Pancreatic Diseases; Pancreatic Ducts; Pancreatic Insufficiency; Pancreatic Pseudocyst; Radiation Injuries
Abbreviations
CP: chronic pancreatitis; CT: computed tomography scan; ERCP: endoscopic retrograde cholangiopancreatography; SPINK1: serine protease inhibitor, Kazal type 1
Chronic pancreatitis (CP) is defined as a continuing inflammatory disease of the pancreas characterized by irreversible morphologic changes which typically cause pain and/or permanent loss of function, evolving over a period of several years into end-stage disease [1, 2, 3, 4, 5, 6]. In clinical practice, this definition distinguishes acute first-onset pancreatitis from advanced CP. However, between these two extremes, it is often difficult to precisely classify pancreatitis for various reasons, including the unavailability of routine means of assessing the early stage of CP [7, 8]. In this regard, pancreatic histology represents the diagnostic gold standard of early stage, but non-surgical access to bioptic specimens of the pancreas still remains difficult [9, 10]. Nowadays we are well aware of the clinical picture of CP, including its various complications, but the current classification systems of the disease give little information about etiology, pathogenesis and outcome.
The classification of any disease has a primary function which is to provide a common language among those caring for the patients. In addition, as for many other chronic diseases, an ideal classification system for CP would be simple, objective, accurate using non invasive procedures, and it should include etiology, pathogenesis, structure, function and clinical status in one overall scheme [8]. The proposed classification systems currently available have not met these criteria. These classifications (which basically reflect the state of the art at the time of promulgation) include a) the Marseille classification of 1963 [11] with revision in 1984 [12], b) the Marseille-Rome classification of 1988 [13], c) the Cambridge classification of 1984 [14], d) the Zurich classification [10] and e) the Japan Pancreas Society classification for CP [15].
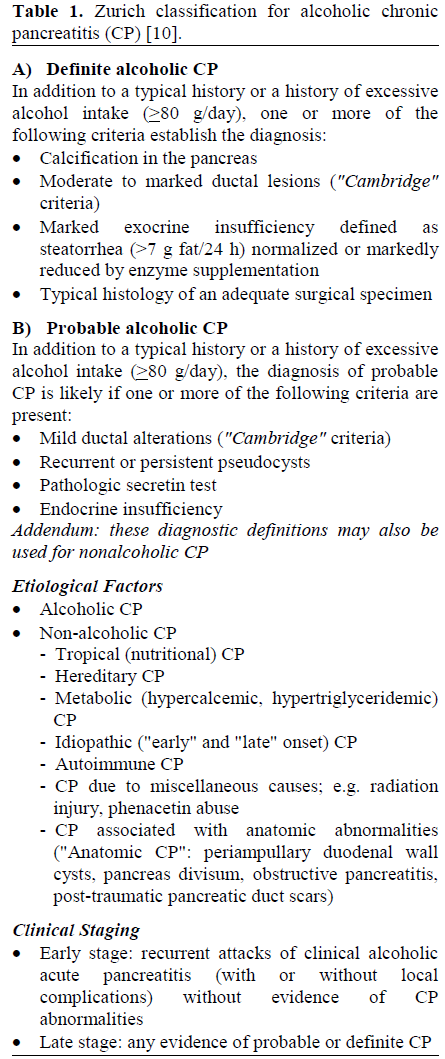
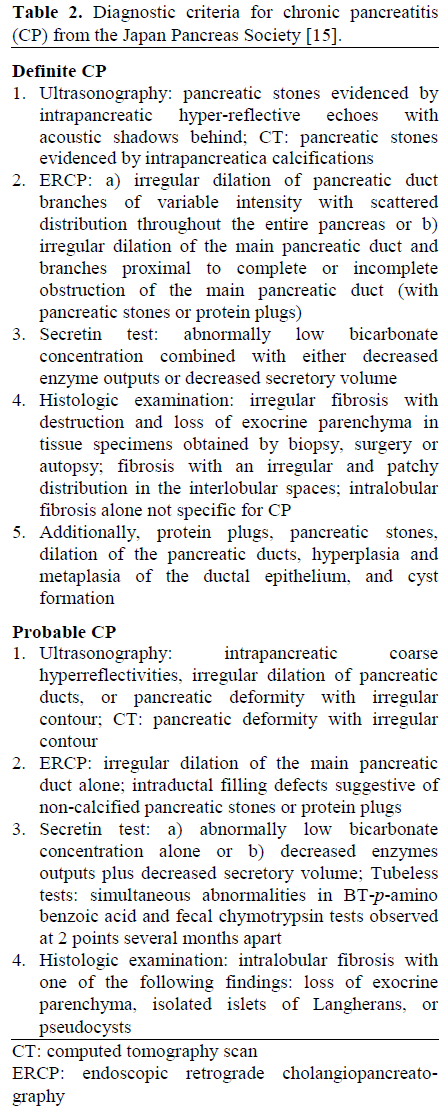
The Marseille and the Marseille-Rome classifications should now be considered inadequate and outdated in the light of the noteworthy understanding in pathophysiology and natural history of the disease obtained over the last fifteen years. The Cambridge classification uses imaging features to provide a grading and severity system but it does not distinguish the different forms of CP on the basis of etiology and clinical outcome. This system proves more useful as a staging system once the diagnosis is made rather than a system for classifying CP [8]. The Zurich classification [10], specifically addressed to the alcoholic form of CP, is quite complex (Table 1), considering diagnosis, etiology, clinical staging, and pain profile separately. This classification emphasizes the dynamism of the disease, but is not widely accepted. The Japan Pancreas Society classification for CP (Table 2) [15] is designed to standardize the diagnostic criteria but lacks etiological and pathogenetic features. Thus, this classification is only partially useful in a clinical setting.
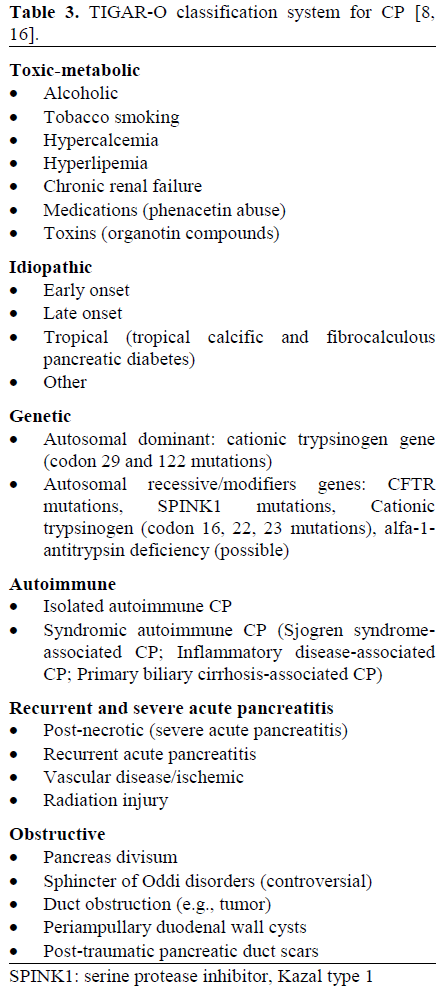
Another recent classification is the risk-factor classification system for CP [16], named TIGAR-O from the acronym of the causes of the disease (Table 3). This classification is based upon new developments for diagnosis and recent advances in genetics, providing new possibilities for the accurate, early identification of the risk factors leading to CP; in addition, the relationship between acute pancreatitis and the development of CP, a controversial issue [17], is also considered. Etemad and Withcomb [8], in a recent comprehensive and up-to-date review of new knowledge about CP, emphasize the usefulness, the potentiality and the clinical implications of this classification system. In fact, the exact knowledge of the etiology of CP remains the basis for understanding the natural and clinical history of the disease and for developing preventive and therapeutic measures [10].
When we are faced with a patient affected by CP, once the diagnosis is made and the contributing etiologic factors are determined, we are well on the way to correctly answering two important questions: "What is going to happen ? " and "What can be done ?".
"Felix qui potuit rerum cognoscere causas" (Vergilius, Georgica, II, 490). - “Happy is he who knows the reason why”.
References
- Sarles H. Definitions and classifications of pancreatitis. Pancreas 1991; 6:470-84. [AN 91343583]
- Kloppel G, Maillet B. Pathology of acute and chronic pancreatitis. Pancreas 1993; 8:659-70. [AN 94077849]
- Cavallini G. Is chronic pancreatitis a primary disease of the pancreatic duct? Ital J Gastroenterol 1993; 25:391-6. [AN 94108115]
- Amman RW, Heitz P, Kloppel G. Course of alcoholic chronic pancreatitis: a prospective clinicomorphological long-term study. Gastroenterology 1996; 111:224-31. [AN 96315564]
- Freedman SD. New concepts in understanding the pathophysiology of chronic pancreatitis. Int J Pancreatol 1998; 8:24:1-8. [AN 98419020]
- Clain JE, Pearson RK. Diagnosis of chronic pancreatitis: is a gold standard necessary? SurgClin North Am 1999; 79:829-45. [AN 99399345]
- Uomo G, Rabitti PG. Chronic pancreatitis: relation to acute pancreatitis and pancreatic cancer. [ANnItalChir 2000; 71:17-21. [AN 20288328]
- Etemad B, Whitcomb DC. Chronic pancreatitis: diagnosis, classification, and new genetic developments. Gastroenterology 2001; 120:682-707. [AN 21100106]
- Steer ML, Vaxman I, Freedman S. Chronic pancreatitis. N Engl J Med 1995; 332:1482-90. [AN 95258097]
- Amman RW. A clinically based classification system for alcoholic chronic pancreatitis: summary of an international workshop on chronic pancreatitis. Pancreas 1997; 14:215-21. [AN 97248027]
- Sarles H. Proposal adopted unanimously by the participants of the Symposium, Marseille 1963. BiblGastroenterol 1965; 7:7-8.
- Singer MW, Gyr K, Sarles H. Revised classification of pancreatitis : report of the Second International Symposium on the Classification of Pancreatitis in Marseille, France, March 28-30, 1984. Gastroenterology 1985; 89:683-5. [AN 85258858]
- Sarles H, Adler G, Dani R, Frey C, Gullo L, Harada H, et al. The pancreatitis classification of Marseille-Rome 1988. Scand J Gastroenterol 1989; 24:641-2. [AN 90048874]
- Sarner M, Cotton PB. Definitions of acute and chronic pancreatitis. ClinGastroenterol 1984; 13:865- 70. [AN 85025511]
- Homma T, Harada H, Koizumi M. Diagnostic criteria for chronic pancreatitis by the Japan Pancreas Society. Pancreas 1997; 15:14-5. [AN 97355292]
- Chari ST, Singer MW. The problem of classification and staging of chronic pancreatitis: proposal based on current knowledge and its natural history. Scand J Gastroenterol 1994; 29:949-60. [AN 95141031]
- Uomo G, Manes G, Rabitti PG. Role of hereditary pancreatitis and CTFR gene mutations in the etiology of acute relapsing pancreatitis of unknown origin. How are they important? JOP. J Pancreas (Online) 2001; 2:368-72. [AN 21872331]

