Keywords
acute renal colic, cross-cover, doctors at
night
Introduction
Acute renal colic is a common, often recurrent condition
with an annual incidence of one to two cases
per 1000 and a lifetime risk of 3–5% in women and
10–20% in men.[1]–[3] Most acute cases of renal colic
initially present to the general practitioner (GP)
with a sudden onset of severe unilateral flank pain
radiating into the groin or genitals.[4],[5]
Renal calculi formin the proximal urinary tract and
migrate distally. They commonly lodge at three points along the ureter: pelvico-ureteric junction, pelvic
brim (where the ureter crosses the iliac vessels) and
the vesico-ureteric junction. The pain is caused by an
obstruction to urinary outflow by the calculus, which
results in an increase in urinary wall tension. This in
turn triggers the synthesis and release of prostaglandins,
which further exacerbate the problem by creating a
diuresis and smooth muscle spasm.[6]
GPs have the frequently difficult task of clinically
diagnosing acute renal colic, deciding whether the
patient requires an acute hospital admission, and
then the arduous task of referring to the on-call junior
doctor or bed manager.[7],[8]
Many hospitals throughout Britain combine their
emergency urology coverwith another surgical specialty,
often, general surgery. This is becoming increasingly
more common with the advent of the European
Working Time Directive.[9],[10] This audit aims to assess
the accuracy of GPs at diagnosing and referring acute
renal colic. It also aims to assess whether patients
receive the ‘gold standard’ investigations and follow
up under a cross-cover system.[11]–[14] Since calcium
oxalate and uric acid constitute 80% of renal stones,
European guidelines recommend that patients presenting
with renal colic should have serum calcium and
uric acid levels checked.[15] These simple and inexpensive
blood tests may reveal a potentially reversible
metabolic condition.
The Royal Gwent Hospital, Newport is a busy 900-
bed district general hospital serving a population of
550 000. Over a six-month period the local GPs made
1548 acute general surgical and 211 acute urology
referrals. Acute urology referrals are assessed by the
on-call urology senior house officer (SHO) with the
exception of renal colic, which is dealt with by the
general surgeons. However, this remains a contentious
issue and some recurrent cases of proven renal
calculi can be referred directly to the urologists if the
GP liaises with the on-call urology SHO. It is well
documented that symptoms suggestive of acute renal
colic may be explained by an acute surgical abdomen
or a leaking abdominal aortic aneurysm.[16]
Method
All GP referrals are made via a nurse practitioner and
recorded in the bed management records at the Royal
Gwent Hospital. The bed management log was used to
identify all patients referred with the diagnosis of
possible renal colic or loin to groin pain over a sixmonth
period from August 2003 to February 2004.
The notes were examined and the diagnosis, investigations
and follow up were recorded.
Results
During the period August 2003–February 2004, 74
patients were admitted with loin to groin pain or
possible renal colic. This averages three admissions per
week; 73 sets of case notes were located and appraised.
The patients included 37 males and 36 females with
an age range from 22 to 84 years, the median being
49 years.
The local GPs were correct in diagnosing 40 cases of
renal colic out of the 73 cases referred (54.8%). Of the
73 cases, 52 were referred to general surgery, while
21 were referred directly to the urologists. The ‘gold
standard’ intravenous urogram (IVU) was used to
confirm that the 40 cases of renal colic were due to
calculi[17] (surgery 21/52 and urology 19/21).
The two remaining urology referrals were: a urinary
tract infection and a large renal cyst distorting the renal
pelvis. Several diagnoses accounted for the remaining
31 general surgical referrals. These are illustrated in Table 1.
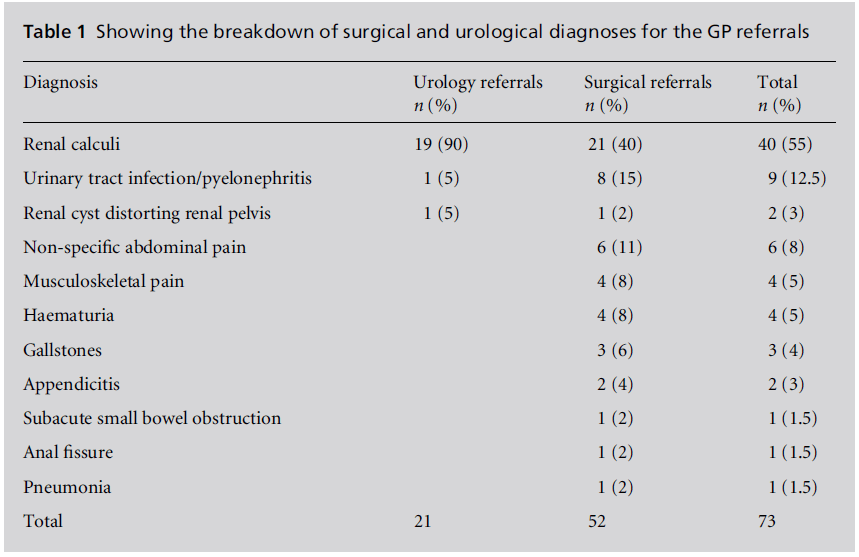

One-hundred percent of the urology referrals had a
urology condition, of which 90% were renal calculi;
65% of the surgical referrals had a urology condition,
of which 40% were renal calculi. Overall, the GPs were
accurate in diagnosing a urology condition 75.5% of
the time.
Only 18% of the referrals had a surgical diagnosis, of
which only 7% required an operation.
Investigations and follow up
Table 2 compares the urology and surgical admissions
for: haematological investigations, time from admission
to diagnosis of renal calculi by IVU and the
subsequent outpatient follow up.
Discussion
The results clearly show that GPs were correct in
diagnosing and referring recurrent cases of renal colic
to the urologists 90% of the time. However, the patients
referred to the general surgeons were not known to have
a previous history of urolithiasis. Thismay explain why
the GPs were less accurate at diagnosing renal colic in
the surgical case group. Perhaps where there was more
diagnostic uncertainty, the GPs chose to refer to the
surgeons rather than the urologists. Although, it is
important to note that 65% of the surgical referrals did
in fact have a urological condition.
Identifying the type of calculi can be helpful in
treating and minimising recurrent cases of renal colic.
Fifty per cent recur within five years. Investigating the
patient and correcting an underlying metabolic disturbance
can avoid this. Following idiopathic renal
colic, the most common metabolic causes can be investigated
with simple haematological tests, e.g. calcium
and urate levels. The less common causes can be
investigated further as an outpatient. Failure to identify
an underlying treatable condition can result in increased GP emergency workload and increased acute
hospital admissions and cause unnecessary distress
and loss of earnings for the patient. Patients admitted
under the care of the urologists are more likely to have
the further investigations and follow up. Another
worrying pitfall in the system is the failure to fully
investigate patients presenting with haematuria. A
quarter of the cases of haematuria did not receive
any routine investigations or follow up. The ‘gold
standard’ is that, ‘all patients with haematuria need
investigation even if they are taking anticoagulant
drugs’. This should include radiographic renal tract imaging, cystoscopy, urine microscopy and urine
cytology.[12],[18],[19] Microscopic haematuria may be the
only feature of an underlying urinary tract neoplasm.
There is no significant difference between the urologists
and surgeons in time to IVU and confirmation
of the diagnosis of renal colic.
There will always be concern for the urologist that
a referred renal colic may turn out to be a leaking
abdominal aortic aneurysm. Conversely, the general
surgeons can argue that an infected, obstructed kidney
or potential urinary neoplasm may be missed or
inappropriately treated, with similar consequences.
Conclusion
Given the accuracy of the local GPs at diagnosing a
urinary problem, and since only 7% of the referrals
had an operable surgical diagnosis, we suggest that all
patients with presumed renal colic are admitted under
the care of the urologists. The GPs should be able to
refer directly to the bed manager in order to provide a
more efficient and effective service for all involved.
However, a swift surgical review should be offered to
any patient of particular concern to the admitting
junior doctor. We are presenting these findings to
both the surgical and urology directorate in order to
encourage the above changes to be implemented.
Potential cases of distressing recurrent renal colic
could be avoided with early investigations. The audit
shows that specialists manage, investigate and follow
up their particular area of expertise more effectively
than other clinicians.
Across-cover system may reduce doctors’ hours but
the question remains, ‘Is this at the expense of the
patient?’.
References
- Scott R. Epidemiology of stone disease. British Journal of
Urology 1985;57:491–7.
- Scott R. Prevalence of calcified upper urinary tract stone
disease in a random population. British Journal of
Urology 1987;59:111–17.
- Ahlstrand C and Tiselius H. Renal stone disease in a
Swedish district during one year. Scandinavian Journal
of Nephrology 1981;15:143–6.
- Banks I. NHS Direct Healthcare Guide. London: NHS
Direct, 2000.
- Eskelinen M. Usefulness of history-taking, physical
examination and diagnostic scoring in acute renal colic.
European Journal of Urology 1998;34:467–73.
- Holdgate A and Pollock T. Systematic review of the
relative efficacy of non-steroidal anti-inflammatory
drugs and opioids in the treatment of acute renal colic.
British Medical Journal 2004;328:1401–4.
- Dawson C and Whitfield H. Urological emergencies in
general practice. British Medical Journal 1996;312:838–
40.
- Morris S, Hampson S, Gordon E, Shearer R and
Woodhouse C. Should all patients with ureteric colic1 Scott R. Epidemiology of stone disease. British Journal of
Urology 1985;57:491–7.
- Scott R. Prevalence of calcified upper urinary tract stone
disease in a random population. British Journal of
Urology 1987;59:111–17.
- Ahlstrand C and Tiselius H. Renal stone disease in a
Swedish district during one year. Scandinavian Journal
of Nephrology 1981;15:143–6.
- Banks I. NHS Direct Healthcare Guide. London: NHS
Direct, 2000.
- Eskelinen M. Usefulness of history-taking, physical
examination and diagnostic scoring in acute renal colic.
European Journal of Urology 1998;34:467–73.
- Holdgate A and Pollock T. Systematic review of the
relative efficacy of non-steroidal anti-inflammatory
drugs and opioids in the treatment of acute renal colic.
British Medical Journal 2004;328:1401–4.
- Dawson C and Whitfield H. Urological emergencies in
general practice. British Medical Journal 1996;312:838–
40.
- Morris S, Hampson S, Gordon E, Shearer R and
Woodhouse C. Should all patients with ureteric colic be admitted? Annals of the Royal College of Surgeons
1995;77:450–2.
- Mahon A and Harris C. The European Working Time
Directive and Doctors in Training: an early evaluation of
19 NHS pilot projects. London: Department of Health,
2003.
- Academy of the Medical Royal Colleges. Implementing
The European Working Time Directive: a position paper.
London: Academy of the Medical Royal Colleges, 2004.
- Bailey H and Love M. Short Practice of Surgery: the
kidneys and ureters (23 edn). London: Arnold Publishing,
p. 1188.
- Bailey H and Love M. Short Practice of Surgery: urinary
symptoms. Investigation of the urinary tract (23 edn).
London: Arnold Publishing, p. 1163.
- Tiselius H, Ackermann D, Alken P et al. Guidelines on
urolithiasis. European Journal of Urology 2001;40:362–
71.
- Feneley R, Gingell J, Abrams P and Frank J. Urology
Guidelines for GPs. Bristol: Bristol Urological Institute,
1999.
- BihlGand Meyers A. Recurrent stone disease – advances
in the pathogenesis and clinical management. Lancet
2001;358:651–6.
- Acheson A. Prospective study on factors delaying surgery
in ruptured abdominal aortic aneurysms. Journal of
the Royal College of Surgeons of Edinburgh 1998;43:182–4.
- Haddad M. Renal colic: diagnosis and outcome. Radiology
1996;184:83–8.
- Scottish Intercollegiate Guidelines Network. A National
Clinical Guideline Recommended for Use in Scotland.
Edinburgh: Scottish Intercollegiate Guidelines Network,
August 1997.
- Sultana S, Goodman C, Byrne D and Baxby K. Microscopic
haematuria: urological investigation using a standard
protocol. British Journal of Urology 1996;78:691.

