Keywords
Acquired Immunodeficiency Syndrome; Antiretroviral Therapy, Highly Active; Islets of Langerhans
Abbreviations
AIDS Acquired immunodeficiency syndrome; HIV Human immunodeficiency virus; HAART Antiretroviral Therapy, Highly Active
INTRODUCTION
Acquired Immunodeficiency Syndrome (AIDS) has become a pandemic disease since the very first cases were reported in 1981. Today there are around 35.3 million patients living with HIV (Human Immunodeficiency Virus), and 2.3 million new cases were reported in 2012, a number that represents a drop of 33% by comparison with the statistics data from 2001. Such a fact reflects a promising tendency of drop not only in number of new cases, but also in the mortality rate: 1.6 million death cases in 2012 vs. 2.3 million cases in 2001 [1].
This trend shows the probable success of the preventive methods applied as well as an improvement in the therapeutic approach to the disease and its consequences.
Among the therapeutic programs for the treatment of HIV we highlight the High Activity Antiretroviral Therapy (HAART), with the systematized use of potent antivirals, in effect since 1996. Many authors have devoted themselves to describing its manifestations in the many systems as a result of the employment of such drugs.An important change in the profile of diseases in the gastrointestinal tract could be observed before HAART was applied, a time when the prevalence of opportunistic infectious agents was a constant feature. In the post-HAART era researchers focus on the effects related to the immune reconstitution syndrome as well as on the collateral effects caused by the medication used both in the prevention and in the treatment of HIV [2].
Regarding the pancreas it could be noticed that the histological pattern in patients infected with HIV in the pre-HAART era was characterized by alterations which were compatible with a state of protein-calorie malnutrition (Kwashiorkor-like): acinus atrophy/ pancreatic parenchyma, a significant decrease in zymogen granules, nuclear abnormalities (dysplasia-like) and pancreatic steatosis. A severe histological impairment of the exocrine pancreas was seen; however, no histological alteration could be observed in the endocrine pancreas with little clinical repercussion [3]. On the other hand, in a pancreas study performed in the post-HAART era in autopsied patients who had died of AIDS, Barbosa et al showed some differences in the pancreatic histology, emphasizing the intense acinar/parenchymal atrophy and a more significant decrease in zymogen granules with important changes in the islets of Langerhans [3]. Such findings brought up issues like the real significance of these alterations of the islets and if they should be attributed to the effect of HAART or perhaps to the effect of a higher survival rate in those individuals with HIV infection. Furthermore, whether endocrine pancreas was affected or not, or the clinical significance of such histological alterations were still unanswered questions.
In the currently reviewed literature it has been questioned if the endocrine function is impaired owing to the use of antiretroviral therapy, which is clearly evidenced by the insulin resistance, dyslipidemia, diabetes and adrenal insufficiency [4].
The aim of this study is to evaluate the morphological aspect of the endocrine pancreas in AIDS patients with and without the use of HAART.
This is a transversal study that was carried out in 27 patients diagnosed with AIDS over the period of Jun 2006-Dec2009. They underwent HAART treatment and necropsies were performed at the Post Mortem Services of the city of São Paulo. The necropsies were certified by one and only experienced pathologist.
In order to meet the inclusion criteria requirements patients had to be 18 years of age or older and diagnosed with AIDS. Patients were divided into 2 groups: those who underwent HAART were included in group 1, and those who did not in group 2.
Patient´s demographic data were obtained from their medical records. The analyzed variables were age, sex, race, body mass index (BMI), alcoholism and cigarette smoking. For the sake of this study, alcoholism was established as the intake of more than 50g of alcohol per day in a period over 5 years. Smoking was established as the regular consumption of at least 10 cigarettes per day. The use of HAART included 1 of the group of protease inhibitors, 1 of the group non-nucleoside analogue reverse transcriptase inhibitors and 1 of the group nucleoside analogue reverse transcriptase inhibitors.
For the macroscopic analysis the pancreas were fully removed, and their weight and any sort of abnormality, like hemorrhage, necrosis, fibrosis or tumor, were registered. The analysis was performed with specimens transversely sectioned from the head, body and tail regions. The samples were fixed in 10% formalin and then dehydrated in alcohol for paraffin embedding. Next, histological sections of 4μm in thickness were stained in haematoxylin–eosin (HE) and placed on slides.
The histopathological analysis of the islets of Langerhans was carried out with a Nikon binocular microscope (Tokyo, Japan) with five achromatic lenses [5, 6].
Concerning the morphometric evaluation of the islets of Langerhans, the following aspects were taken into consideration: number of islets per microscopic visual field and islet areas. For the sake of comparative evaluation of acinar cells and islets, the slides were stained with periodic acid-Schiff reagent (PAS). A Zeiss trinocular microscope, with magnification level of 200X, was used for such analysis in 10 consecutive fields, and the images were captured using a digital camera attached to a computer by means of the morphometry software Image ToolM® (University of Texas Health Center, USA).
A total of 2 quantitative analyses were conducted: the counting of number of islets and their area calculation expressed in μ2.Each field was evaluated separately and all the data properly registered. The software converted the area of the islets from μ2 to pixels.
ETHICS
This study was performed with the aid of the Department of Pathology at the Faculdade de Medicina do ABC, and it was approved by the local Ethics Committee under the number 141/2006.
STATISTICS
Those fields without islets were disregarded when field areas were compared. Thus, there were variations in number of fields per studied area, and a mean comparison was performed on each field per group.
Kolmogorov-Smirnov test was used for normality analysis and Levene’s test for homogeneity of variances. As the variables (mean of areas) did not meet either test criteria satisfactorily, the non-parametric Mann-Whitney U test was applied. The significance level was set at p=0.05 and SPSS 17.0 for Windows was the statistical package of choice.
RESULTS
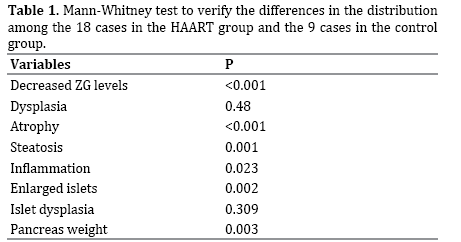
A total of 27 patients fulfilled the inclusion criteria during the study analysis. Among that number, 18 subjects used HAART and 9 did not. The HAART group was composed of 17 men (94.44%), and the control group, composed of 9 individuals, had 5 men (55.56%) out of that total. The mean pancreas weight was 98.75g (±31.92) in the HAART group and 144.4g (±22.22) in the control group. The mean age was 40.35 years (±8.87) in the HAART group and 53.9 years (±8.5) in the control group. None of them were diabetic or had the diagnostic of chronic pancreatitis. The main cause of the death in the groups was infectious diseases, opportunistic infections or septicemia. Table 1 shows the histological comparison of the groups: decreased zymogen granule, nuclear dispasia, parenchima atrophy, steatosis, inflammation, enlarged islets, islet nuclear dysplasia and pancreas weight.
For the morphometric evaluation the area of each microscopic field was analyzed and the total sum of all areas from each group was used since in some fields no islets could be found and in others more than one was detected.
Table 2 shows the evaluation of areas in each of the 10 studied fields during the morphometric evaluation. The general analysis of the mean islet areas showed a significant difference (p=0.015). They were prone to hypertrophy (Figure 1) in the HAART group and presented no alterations in the control group (Figure 2).
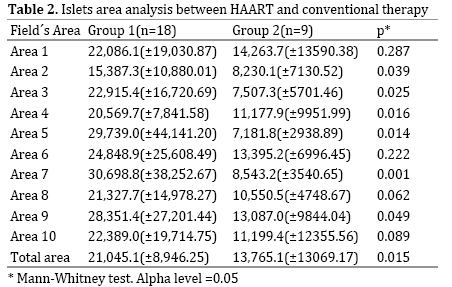
Figure 1. Islet areas showed a prone to hypertrophy in the HAART group.
Figure 2. Islet areas showed no alterations in the control group.
DISCUSSION
In the current study it was shown that the pancreas undergoes changes when infected with HIV. In the histology analysis of the pancreas without HAART the alterations in the exocrine pancreas was clear with maintenance of endocrine tissues. However, besides the intensification of the atrophic pattern, the decrease in zymogene granules, the detection of nuclear abnormalities and alterations in the histological pattern, hypertrophy of Langerhans islets could also be observed, which led us to speculate on its causes.
Such findings could firstly be attributed to a longer disease period, namely, having contact with HIV infection over the years might lead to those alterations. A second possible explanation for the histological alterations of the islets could be these patients' higher survival rate. Living a longer and better life, these individuals might end up developing other diseases like hypertension, dyslipidemia or diabetes. Our third hypothesis is that the use of HAART might affect the pancreas directly or by its collateral effects like dyslipidemia and obesity.
It is known that some medications used in HAART, such as didanosine (ddI), stavudine and pentamidine, may cause acute pancreatitis and therefore are gradually being discontinued from the treatment regimen. With the use of more recent drugs, very few proven cases of acute pancreatitis have been reported. Some of the risk factors for acute pancreatitis are HIV effects (high viral load, T-lymphocyte count CD4 (+) ≤ 200 cells/mm3 and the long-term seropositivity), advanced age, underweight female individuals (47-54kg), the combination of HAART with hydroxyurea, alcohol consumption, illicit drugs and previous pancreatitis history [7].
Besides pancreatitis, such drugs might produce a toxic lesion in the cells of the islets of Langerhans, bringing consequences like functional impairment of α- or β-cells and the resultant onset of diabetes or some other pathology.
More recently researchers have turned an eye to the disorders of glucose and lipid metabolism, which figure among the many adverse effects of HAART. These disorders are here represented as the peripheral resistance to insulin, impaired fasting and post-prandial glycemia, hyperinsulinemia, type 2 diabetes mellitus (DM), dyslipidemia and disorders related to body fat distribution like lipodystrophy [8, 9].
This broad spectrum of metabolic disorders is undoubtedly related to an increased risk of cardiovascular diseases [2], which has prompted researchers to investigate consistent associations between the use of combined antiretroviral drugs in patients with HIV and the onset of metabolic syndrome and type 2 diabetes in this population.
Prospective and retrospective studies on the theme estimate a prevalence of metabolic syndrome in HIV patients between 2 and 18%, numbers that are not so different from those found in the general population [8- 10]. However, when the prevalence of glucose metabolic alterations is isolatedly analyzed (fasting glycemia and glucose overload test), those numbers rise to 25-35%, especially in patients receiving combined antiretroviral therapy, which suggest a strong influence of these drugs on the glucose-insulin balance in those individuals [9, 10].
Therefore, the many studies that have been conducted to reveal the physiopathological mechanisms involved have concluded that glucose metabolic disorders in patients undergoing HAART are almost exclusively influenced by the peripheral resistance to insulin [8, 10, 11]. Furthermore, numberless evidences have pointed to biochemical factors, associated with the mitochondrial dysfunction, as the key for understanding the insensibility to insulin in these patients, especially those who receive protease inhibitors, or nucleoside reverse transcriptase inhibitors (NRTIs) as part of the therapy [12, 13].
However, very little has been reported on the role the endocrine pancreas actually plays in the genesis of glycemic alterations found in HAART patients. Some evidences show a reduction of 25-50% in insulin secretion and in the function of pancreatic β-cells in patients who started the use of protease inhibitors (PIs) or were on the use of NRTIs and started on PIs. Dysfunctions of pancreatic β-cells can be assessed in vivo through the significant decrease in the dosages of insulin, proinsulin and C-peptide after glucose overload. The in vitro analysis of insulin-producing cells could also register not only a reduced secretion of the hypoglycemic hormone but also a decreased sensibility of β-cells to glucose, probably owing to the reduced GLUT-2 expression in this cell lineage [8].
The reported histological alterations in the current study strengthen the hypothesis that the endocrine section of the pancreas is strongly affected by the combined antiretroviraltherapy, and it most likely powerfully influences the onset of glycemic alterations in this population.
The finding of abnormally increased pancreatic islets in HAART patients, when compared with non-HAART patients, allows us to infer that there is more than one peripheral component, like tissue insensitivity to insulin, determining a higher prevalence of type 2 DM or even altered fasting glycemia in those who receive the treatment.
In conclusion, the postmortem pancreatic examination in this cohort of AIDS patients who underwent HAART highlighted hypertrophy of the islets of Langerhans; nevertheless, further researches encompassing the endocrine pancreatic function are required to clarify this matter.
Conflicting Interest
The authors had no conflicts of interest
References
- UNAIDS: Report on Global AIDS epidemic.2013 [https://www.unaids.org/globalreport].
- Huppmann AR, Orenstein JM. Opportunistic disorders of the gastrointestinal tract in the age of highly active antiviral therapy. Hum Pathol 2010; 41:1777-87. [PMID: 21078437]
- Barbosa AG, Chehter EZ, Bacci MR, Mader AA, Fonseca FL. AIDS and the pancreas in the HAART era: a cross sectional study. Int Arch Med 2013; 6:28. [PMID: 23856035]
- Kibirige D, Ssekitoleko R. Endocrine and metabolic abnormalities among HIV-infected patients: A current review. Int J STD AIDS 2013; 24:603-11. [PMID: 23970578]
- Kerr JF, Wyllie AH, Currie AR. Apoptosis: a basic biological phenomenon with wide-ranging implications in tissue kinetics. BR J Cancer 1972; 26:239-57. [PMID: 4561027]
- Michalany J. Histhological technique in pathological anatomy: with instructions to surgeon, nurse and cytotechnique. Säo Paulo: Publisher Michalany 1998; 3.
- Oliveira NM, Ferreira FA, Yonamine RY, Chehter EZ. Antiretroviral drugs and acute pancreatitis in HIV/AIDS patients: is there any association? A literature review. Einstein 2014; 12:112-9. [PMID: 24728257]
- Samaras K. Prevalence and Pathogenesis of Diabetes Mellitus in HIV-1 Infection Treated With Combined Antiretroviral Therapy. J Acquir Immune Defic Syndr 2009; 50:499-505. [PMID: 19223782]
- Calza L, Masetti G, Piergentili B, Trapani F, Cascavilla A, Manfredi R, Colangeli V, Viale P. Prevalence of diabetes mellitus, hyperinsulinaemia and metabolic syndrome among 755 adult patients with HIV-1 infection. Int J STD AIDS 2011; 22:43-5. [PMID: 21364066]
- Samaras K, Wand H, Law M, Emery S, Cooper D, Carr A. Prevalence of Metabolic Syndrome in HIV- Infected Patients Receiving Highly Active Antiretroviral Therapy Using International Diabetes Foundation and Adult Treatment Panel III Criteria. Diabetes Care 2007; 30:113-9. [PMID: 17192343]
- Tebas P. Insulin Resistance and Diabetes Mellitus Associated With Antiretroviral Use in HIV-Infected Patients: Pathogenesis, Prevention, and Treatment Options. J Acquir Immune Defic Syndr 2008; 49:S86-92. [PMID: 18725817]
- Shikuma CM, Day LJ, Gerschenson M. Insulin Resistance in the HIVInfected Population: The Potential Role of Mitochondrial Dysfunction. Curr Drug Targets Infect Disord 2005; 5:255-62. [PMID: 16181144]
- Apostolova N, Blas-García A, Esplugues JV. Mitochondrial Toxicity in HAART: An Overview of In Vitro Evidence. Curr Pharm Des 2011; 17:2130-44. [PMID: 21718249]



