Satheesha Badagabettu Nayak, Naveen Kumar, Ashwini Aithal Padur, Srinivasa Rao Sirasanagandla and Surekha Devadasa Shetty
Department of Anatomy, Melaka Manipal Medical College (Manipal Campus), Manipal University, Manipal, Karnataka, India 576104
*Corresponding Author:
Ashwini Aithal P
Department of Anatomy,
Melaka Manipal Medical College(Manipal Campus)
Manipal University, Manipal
Karnataka, India 576104
Tel: +08095132879
E-mail: ashwini.anat@gmail.com
Received November 20th, 2015 - Accepted December 30th, 2015
Keywords
Epilepsy, Temporal Lobe; Mesenteric Artery, Superior; Mesenteric Veins; Pancreas
Abbreviations
IOUS intraoperative ultrasound
INTRODUCTION
The pancreas is a soft, fleshy, lobulated, mixed gland. It is about 6-8 inches long and weighs approximately 90 gm. It lies within the curve of the first, second and third parts of the duodenum. It extends upwards and to the left across the posterior abdominal wall from duodenum to the spleen, behind the lesser sac of peritoneum. The main portion of the gland is divided into four parts: head, neck, body and tail. The pancreas also possesses one accessory lobe known as the uncinate process which is anatomically and embryologically distinct. It extends to the left from the lower-lateral end of the head and lies behind the superior mesenteric vessels. The uncinate process lies in front of the aorta, and above the third part of the duodenum. Tumors of the uncinate process frequently compress the third part of the duodenum due to this close relationship [1]. Variations in the morphology of pancreas is unusual especially that involving the uncinate process is very rarely encountered. We report in here a unique presentation of the uncinate process in a cadaver which was extensive, very long and enclosed the origin of the superior mesenteric artery. We performed the histology study of this tissue to confirm whether it is a part of pancreatic parenchyma or a tumor. We believe that this elongated uncinate process can cause compression of neurovascular structures particularly the superior mesenteric artery and also cause compression of adjoining viscera. Basic anatomical knowledge regarding the pancreas and its variations is essential in treating any diseases of the pancreas. Since available literature regarding variations of the uncinate process is limited we performed the histomorphological study of this anomalous uncinate process found in an adult male cadaver.
MATERIALS AND METHODS
The current study was conducted in the department of Anatomy, Melaka Manipal Medical College, Manipal. The study was conducted on an unusually large uncinate process of pancreas which was found in an adult male cadaver aged 72 years approximately. The specimen was cleaned carefully to display the relations of pancreas. The pancreas was 14 cm long. Its head was fitting the curve of the duodenum. Its uncinate process was very long and measured 8 cm. It ascended upward and to the left in front of the abdominal aorta (Figure 1). It enclosed the origin of the superior mesenteric artery and further ascended upwards on the anterior surface of the left suprarenal gland, on the left side of the origin of coeliac trunk. The splenic artery crossed the uncinate process from right to left and the left gastric artery ascended very close to its upper part (Figure 2). We conducted a histological study to confirm if it is a pancreatic tissue and to rule out the possibility of a pancreatic tumour. The uncinate process was dissected out and preserved in 10% formalin. 3-4 pieces of the tissue were obtained from different areas of the uncinate process. These were processed, embedded in paraffin and sections were obtained on clean glass slides. The sections were stained with Haematoxylin & Eosin stains and examined under the microscope under different magnifications and photographs were taken (Figures 3,4)
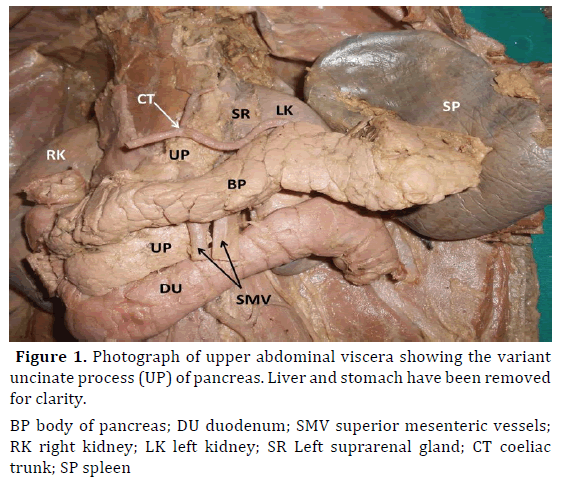
Figure 1. Photograph of upper abdominal viscera showing the variant uncinate process (UP) of pancreas. Liver and stomach have been removed for clarity.
BP body of pancreas; DU duodenum; SMV superior mesenteric vessels; RK right kidney; LK left kidney; SR Left suprarenal gland; CT coeliac trunk; SP spleen
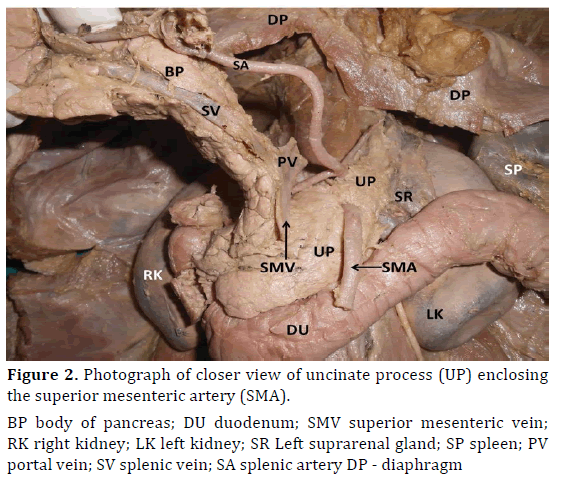
Figure 2. Photograph of closer view of uncinate process (UP) enclosing the superior mesenteric artery (SMA).
BP body of pancreas; DU duodenum; SMV superior mesenteric vein; RK right kidney; LK left kidney; SR Left suprarenal gland; SP spleen; PV portal vein; SV splenic vein; SA splenic artery DP - diaphragm

Figure 3. Photomicrograph (10x magnification) of the uncinate process showing the deeply stained (A.). exocrine part consisting of pancreatic acini. (I.). Endocrine part consisting of islets of Langerhans can be seen with pale-staining cells. (S.). Connective tissue septum is seen (H&E stain.). separating the lobules.
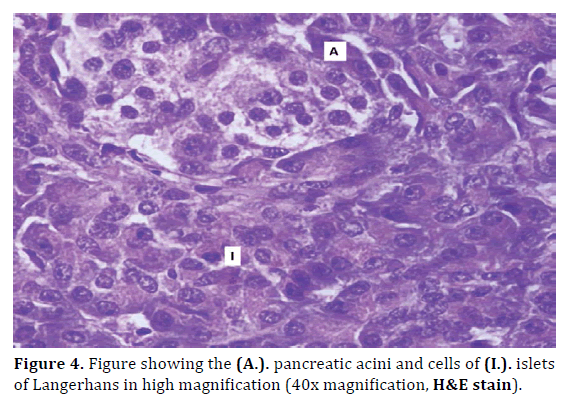
Figure 4. Figure showing the (A.). pancreatic acini and cells of (I.). islets of Langerhans in high magnification (40x magnification, H&E stain).
OBSERVATIONS AND RESULTS
The microscopic study of the H&E stained sections showed the presence of the exocrine and endocrine part of the pancreas which confirmed that the tissue found encircling the superior mesenteric artery was a normal pancreatic tissue and a part of the uncinate process. Exocrine part consisting of pancreatic acini was clearly seen, where the acinar cells were deeply stained basally, indicating the high ribosomal concentration. The endocrine part constituting the islet of Langerhans was also seen, with pale staining cells. But we observed the islets were very few and were surrounded by a network of capillaries. Connective tissue septa were seen separating the lobules of the gland.
DISCUSSION
Anomalies of the pancreas are usually associated with its embryological development, whereas its disorders can be classified as those affecting its ductal system and those associated with the parenchyma of the gland [2]. The pancreas develops from dorsal and ventral pancreatic buds, which are two endodermal buds arising from the caudal part of the foregut. Major part of the pancreas develops from the dorsal pancreatic bud which appears first during its development and is located cranial to the ventral pancreatic bud. The ventral pancreatic bud is smaller in size and develops close to the entry of the common bile duct into the duodenum. After the duodenal rotation to the right side, ventral pancreatic bud lies posterior to the dorsal bud and then fuses with it. The upper part of head, neck, body and tail of the pancreas are derived from the dorsal bud and the lower part of pancreatic head and uncinate process develop from the ventral bud [3]. One of the most interesting variation of the pancreas is the hypertrophied uncinate process which results due to excessive fusion between the ventral and dorsal buds during embryonic development [4]. During our literature review we found that most commonly reported variations of the uncinate process is the presence of annular pancreas, half annular pancreas, pancreas divisum, ectopic pancreas, pancreatic agenesis. Similarly, portal annular pancreas is another rare anatomical anomaly in which the pancreatic tissue surrounds the superior mesenteric vein and portal vein like a ring [5,6,7]. The incidence of portal annular pancreas is said to be 1.14% to 2.5% [8,9]. The authors have opined that although its prevalence is not extremely low but it is not readily recognized on preoperative imaging due to lack of adequate knowledge and awareness of this uncommon variant. But in the current case we found that the uncinate process encircled the superior mesenteric artery near its origin. This may lead to compression of the artery and since it is the main artery supplying the intestines it can result in fatal consequences also, if vascular supply to the intestine is affected. These types of cases have to be considered carefully during pancreatic resections. It may also result in clinical complications like obstruction of the duodenum or pancreatitis. The cause of pancreatic hypertrophy is usually congenital but occasionally it could be acquired also [10]. It is important for surgeons to acquaint with the anatomical relations of the uncinate process and its variations especially its relation with the superior mesenteric vessels to avoid any unwanted iatrogenic complications. We found just one case report in which the hypertrophic uncinate process of the pancreas wrapped the superior mesenteric vein and artery which was observed during surgery on a patient with nodular chronic pancreatitis [11]. It can be seen that while portal annular pancreas is encasement of superior mesenteric vein/portal vein by the uncinate process it might be rarely associated with concomitant encasement of the superior mesenteric artery and hence endoscopists, radiologists and surgeons should give utmost importance to such a rare pancreatic anomaly during diagnostic and therapeutic procedures [12]. Such anomalies should be borne in mind during differential diagnosis for abnormal conditions of pancreas and its associated structures. A study by Maker et al. has revealed that though despite having various diagnostic tools including endoscopic retrograde cholangiopancreatography, preoperative diagnosis is successfully reached in only 60% of patients because some variations remain unnoticed [13]. The normal histology of this pancreatic mass ruled out the possibility of a tumor of pancreas. Such congenital anomalies or normal variants of the pancreas can present a diagnostic challenge when encountered during surgery. Hence prior knowledge is essential to identify these entities and help differentiate them from pathologic conditions and for successful accomplishment of surgical, oncologic or interventional procedures.
CONCLUSION
This is a new and unusual presentation of the uncinate process of the pancreas which is quite different from that of previous reports. We believe that this will enhance the basic anatomic knowledge and requires special attention as it has immense surgical importance. Surgeons need to be aware regarding such rare pancreatic condition prior to any surgical interventions to avoid any undue complications.
Conflict of Interests
Authors declare no conflict of interests for this article.
References
- Standring S. Gray’s Anatomy. 40th edition. Churchill Livingstone 2008; 1147-1148.
- Adda G, Hannoun L, Loygue J. Development of the human pancreas: variations and pathology. A tentative classification. Anat Clin 1984;5:275-283. [PMID: 6372837]
- Moore KL, Persaud TV. The developing human: clinically oriented embryology. 8th ed. Philadelphia: Saunders 2008; 264-265.
- Sugiura Y, Shima S, Yonekawa H, Yoshizumi Y, Ohtsuka H, Ogata T. The hypertrophic uncinate process of the pancreas wrapping the superior mesenteric vein and artery: a case report. Jpn J Surg 1987;17:182-185. [PMID: 3626212]
- Joseph P, Raju RS, Vyas FL, Eapen A, Sitaram V. Portal annular pancreas: a rare variant and a new classification. JOP 2010;11:453-455. [PMID: 20818114]
- Nayak BS, Ooi MY. A Classic Case of Annular Pancreas and its Clinical Implications. Int J Morphol 2011;29:559-561.
- Nayak BS, Kumar N, Sirasanagandla SR, Swamy RS, Surendran S. Half annular pancreas - a cadaveric case report. EL Mednifico Journal 2014;2:411-412.
- Karasaki H, Mizukami Y, Ishizaki A, Goto J, Yoshikawa D, Kino S, Tokusashi Y, et al. Portal annular pancreas, a pancreatic malformation: Frequency, morphology, and implications for pancreatic surgery. Surgery 2009;146:515–518. [PMID: 19715809]
- Ishigami K, Tajima T, Nishie A, Asayama Y, Kakihara D, Nakayama T, Shirabe K, et al. The prevalence of circumportal pancreas as shown by multidetector-row computed tomography. Insights Imaging 2011; 2:409-414. [PMID: 22347962]
- Nayak S, Pamidi N, George BM, Guru A. A strange case of double annular pancreas. JOP 2013;14:96-98. [PMID: 23306345]
- Sugiura Y, Shima S, Yonekawa H, Yoshizumi Y, Ohtsuka H, Ogata T. The hypertrophic uncinate process of the pancreas wrapping the superior mesenteric vein and artery--a case report. Jpn J Surg 1987;17:182-185. [PMID: 3626212]
- Swati G, Mona S, Rohini P, Avinash T, Vandana M, Rajesh K et al. Unduly extensive uncinate process of pancreas in conjunction with pancreatico-duodenal fold. Anat Cell Biol 2015;48:81-83. [PMID: 25806126]
- Maker V, Gerzenshtein J, Lerner T. Annular pancreas in the adult: two case reports and review of more than a century of literature. Am Surg 2003;69:404-410. [PMID: 12769212]

