Saravanan Kokila Krishnamoorthy1, Morris Hayim2, Tyler Vestal1, Muhammad Wasif Saif3
1Department of Radiology, Columbia University. New York, NY, USA.
2Department of Radiology, University of Massachusetts Medical Center. Worcester, MA, USA.
3Department of Medicine and Cancer Center, Tufts Medical Center. Boston, MA, USA
- *Corresponding Author:
- Saravanan Kokila Krishnamoorthy
Department of Radiology. Columbia University
180 Fort Washington Avenue, 3rd Floor
Harkness Pavillion, Room 313
New York, NY 10032; USA
Tel: +1-212.305.9729
Fax: +1-212.305.5777
E-mail: sk3552@columbia.edu
Keywords
(18F)-1-alpha-D-(2-deoxy-2-fluoroarabinofuranosyl)- 2-nitroimidazole; Pancreatic Neoplasms; Positron- Emission Tomography; Predictive Value of Tests
Abbreviations
FAZA: 18F-fluoroazomycin arabinoside; FLT: 3’- deoxy-3’-(18F) fluorothymidine
What We Knew Before the 2013 American Society of Clinical Oncology (ASCO) Annual Meeting
Pancreatic cancer is the fourth leading cause of cancer deaths in men and women [1]. The five-year survival for all patients with pancreatic adenocarcinoma is less than 5% [2]. Metastatic pancreatic cancer remains a difficult disease to cure. Assessing response to treatment has been based primarily on the primitive Response Evaluation Criteria In Solid Tumors (RECIST) that has high variability [3, 4]. The usefulness of RECIST as an endpoint is suspect [5, 6]. Alternatives are needed that either: 1) assess the mechanism of the therapy; or 2) perform image feature analysis.
What We Learnt at the 2013 American Society of Clinical Oncology (ASCO) Annual Meeting
This paper summarizes the abstract presentations of pancreatic cancer imaging at recent ASCO Annual Meeting (Table 1).
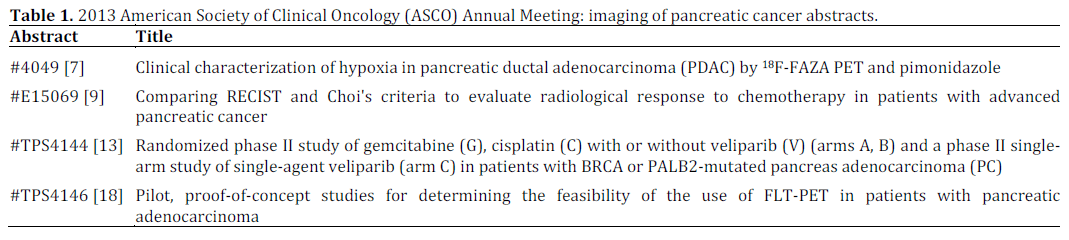
Clinical Characterization of Hypoxia in Pancreatic Ductal Adenocarcinoma (PDAC) by 18F-FAZA PET and Pimonidazole (Abstract #4049 [7])
Pimonidazole has been studied as a marker of hypoxia in malignancy for over a decade [8]. By administrating pimonidazole into tumors, immunohistochemistry can be performed of pathology specimens to assess for hypoxia. Since certain therapies attempt to treat pancreatic adenocarcinoma via hypoxia, imaging of hypoxia may allow us to non invasively assess treatment response without the randomness and risks of needle biopsy. In this study, 16 patients were imaged with PET using 18F-fluoroazomycin arabinoside (FAZA) as a functional tracer for hypoxia. The PET-CT images were registered with the immunohistochemistry slices to correlate the uptake on PET to histopathology of the surgically resected cancer. In this small sample of studies, a SUVmax of 1.27 defined the threshold for hypoxic percent of 0-60% with minimal hypoxia of less than 10%.
Comparing RECIST and Choi’s Criteria to Evaluate Radiological Response to Chemotherapy in Patients with Advanced Pancreatic Cancer (Abstract #e15069 [9])
Since there are significant limitations to assessing treatment response by single dimensional measurements, there has been intense interest in finding advanced imaging features that may perform with less variability and better accuracy.
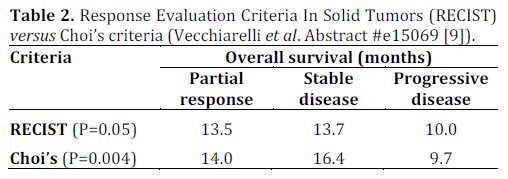
The mean density of malignant tissue on CT can decrease with response to treatment as the neoplastic cells become necrotic. Choi’s criteria has been studied in other tumors, such as gastrointestinal stromal tumors [10], melanoma [6], and colorectal metastases to the liver [11]. In this study, RECIST and the Choi’s criteria were used as biomarkers for overall survival in 66 patient with locally advanced adenocarcinoma (40 patients) and metastatic disease (26 patients). The patients received either gemcitabine or FOLFIRINOX (5- fluorouracil, oxaliplatin, irinotecan, leucovorin). Choi’s criteria had a significant difference between partial response, stable disease, and progressive disease (Table 2). Only the Choi’s criteria showed a significant difference between: 1) partial response plus stable disease; and 2) progressive disease with a P=0.02.
Discussion
Functional imaging or advanced image feature analysis offer the potential for improved assessment of treatment response in pancreatic adenocarcinoma as compared to RECIST. Hypoxia imaging is one method that is important since certain chemotherapy agents work via hypoxia. Nascente et al. showed the feasibility of correlating surgically resected specimens with PET imaging [7]. This pilot data can be used to perform a study with a larger number of patients in order to determine if hypoxia imaging with 18F-FAZA PET will correlate with overall survival. If such a study is positive, then 18F-FAZA PET may allow for selecting patients who will respond to hypoxia chemotherapy.
An alternative approach is to perform advanced image feature analysis. One such feature is the density of a mass on CT (Choi’s critera) rather than a single dimension, as with RECIST. Vecchiarelli et al. showed that the Choi’s criteria may be a better biomarker of overall survival than RECIST [9]. One reason for concern with monitoring changes in the imaging features of pancreatic adenocarcinoma on imaging is the ill-defined margins that are classic for this cancer (Figure 1). Therefore, differences in imaging parameters and difficulty in identifying the full volume of the mass may cause this technique to fail when applied in multiple centers.
Figure 1. Contrast enhanced MRI of pancreatic adenocarcinoma (arrows) with the characteristic ill defined margins that render this type of cancer difficult to delineate.
Given the positive result with other image features in other malignancies, such as lung, further work can be done using additional imaging features with existing research software [12]. By employing such techniques, we will better understand the robustness of these imaging features.
The remainder of the studies are in progress. Abstract #TPS4144 addressed the interesting category of BRCA or PALB2-mutated pancreas adenocarcinoma with phase II arms [13]. Since multicenter trials for the most part involve standard RECIST criteria, it is uncertain how robust the future data from this study will be if expanded to a larger population. Furthermore, drug dosing is typically capped by toxicity rather than response in imaging, which means some patients will not tolerate the chemotherapy. An alternative method is to determine the dosing needed to render a change on imaging, as has been shown using dynamic contrast enhancing MRI before and after antiangiogenesis drugs at various dosing levels [14].
In the realm of functional imaging, fluorinated thymidine analog, 3’-deoxy-3’-(18F) fluorothymidine (FLT) PET has shown promise in a variety of cancers [15, 16, 17] as a biomarker of tumor proliferating activity since FLT is phosphorylated by thymidine kinase-1. The research outlined in Abstract #TPS4146 is a proof of concept study to assess the feasibility of FLT-PET in pancreatic adenocarcinoma [18].
Conflict of interest
The authors have no potential conflict of interest
References
- Jemal A, Siegel R, Xu J, et al. Cancer statistics, 2010. CACancer J Clin 2010;60:277-300.
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CACancer J Clin 2012;62:10-29.
- Muenzel D, Engels HP, Bruegel M, et al. Intra- and interobservervariability in measurement of target lesions:implication on response evaluation according to RECIST 1.1.Radiol Oncol. 2012 Mar;46(1):8-18.
- Zhao B, Tan Y, Bell DJ, et al. Exploring intra- and inter-readervariability in uni-dimensional, bi-dimensional, and volumetricmeasurements of solid tumors on CT scans reconstructed atdifferent slice intervals. Eur J Radiol. 2013 Jun;82(6):959-68.
- Katz MH, Fleming JB, Bhosale P, et al. Response of borderlineresectable pancreatic cancer to neoadjuvant therapy is notreflected by radiographic indicators. Cancer. 2012 Dec1;118(23):5749-56.
- Uhrig M, Hassel JC, Schlemmer HP, et al. Therapy responseassessment in metastatic melanoma patients treated with a BRAFinhibitor: adapted Choi criteria can reflect early therapyresponse better than does RECIST. AcadRadiol. 2013Apr;20(4):423-9.
- Nascente CM, Dhani NC, Vines D, Yeung I, Metser U, Serra S,et al. Clinical characterization of hypoxia in pancreatic ductaladenocarcinoma (PDAC) by 18F-FAZA PET and pimonidazole. JClinOncol 31, 2013 (Suppl.): Abstract #4049.
- Varia MA, Calkins-Adams DP, Rinker LH, et al. Pimonidazole:a novel hypoxia marker for complementary study of tumorhypoxia and cell proliferation in cervical carcinoma. GynecolOncol. 1998 Nov;71(2):270-7.
- Vecchiarelli S, Macchini M, Grassi E, Ferroni F, CiccareseF,Calculli L, et al. Comparing RECIST and Choi’s criteria to evaluateradiological response to chemotherapy in patients with advancedpancreatic cancer. J ClinOncol 31, 2013 (Suppl.): Abstract#e15069.
- Schramm N, Englhart E, Schlemmer M, et al. Tumor responseand clinical outcome in metastatic gastrointestinal stromaltumors under sunitinib therapy: comparison of RECIST, Choi andvolumetric criteria. Eur J Radiol. 2013 Jun;82(6):951-8.
- Chung WS, Park MS, Shin SJ, et al. Response evaluation inpatients with colorectal liver metastases: RECIST version 1.1versus modified CT criteria. AJR Am J Roentgenol. 2012Oct;199(4):809-15.
- Lee HJ, Kim YT, Kang CH, et al. Epidermal Growth FactorReceptor Mutation in Lung Adenocarcinomas: Relationship withCT Characteristics and Histologic Subtypes. Radiology. 2013 Mar7. [Epub ahead of print].
- O'Reilly EM, Lowery MA, Yu KH, Capanu M, StadlerZK,Epstein AS, et al. Randomized phase II study of gemcitabine (G),cisplatin (C) with or without veliparib (V) (arms A, B) and aphase II single-arm study of single-agent veliparib (arm C) inpatients with BRCA or PALB2-mutated pancreas adenocarcinoma(PC). J ClinOncol 31, 2013 (Suppl.): Abstract #TPS4144.
- Yopp AC, Schwartz LH, Kemeny N, et al. Antiangiogenictherapy for primary liver cancer: correlation of changes indynamic contrast-enhanced magnetic resonance imaging withtissue hypoxia markers and clinical response. Ann Surg Oncol.2011 Aug;18(8):2192-9.
- McKinley ET, Smith RA, Zhao P, et al. 3'-Deoxy-3'-18FfluorothymidinePET predicts response to (V600E)BRAFtargetedtherapy in preclinical models of colorectal cancer. J NuclMed. 2013 Mar;54(3):424-30.
- Corroyer-Dulmont A, Peres EA, Petit E, et al. Detection ofglioblastoma response to temozolomide combined withbevacizumab based on μMRI and μPET imaging reveals (18F)-fluoro-L-thymidine as an early and robust predictive marker fortreatment efficacy. NeuroOncol. 2013 Jan;15(1):41-56.
- Contractor K, Challapalli A, Tomasi G, et al. Imaging ofcellular proliferation in liver metastasis by (18F)-fluorothymidine positron emission tomography: effect oftherapy. Phys Med Biol. 2012 Jun 7;57(11):3419-33.
- Lamarca A, Manoharan P, Asselin MC, Trigonis I, HindmarshP, Wood S, et al. Pilot, proof-of-concept studies for determiningthe feasibility of the use of FLT-PET in patients with pancreaticadenocarcinoma. J
- ClinOncol 31, 2013 (Suppl.): Abstract#TPS4146.


