Keywords
Pancreatitis, Chronic; Penetrance; PRSS1 protein, human
INTRODUCTION
Hereditary pancreatitis is an autosomal dominant inherited disease which was first described in 1952 by Confort and Steimberg who suggested a possible genetic abnormality as the cause [1]. Until 1996, the diagnosis of hereditary pancreatitis was based on the presence of recurrent episodes of acute pancreatitis or signs of chronic pancreatitis often beginning in the first two decades of life, a family history of at least two other affected members (more than 3 patients with pancreatitis in a family), equal sex distribution, frequent presence of intraductal calcified stones and the absence of known etiologic factors, such as alcohol or gallstones [2]. In 1996, a genetic defect was first identified by Whitcomb et al who demonstrated the association between mutations in the cationic trypsinogen gene (PRSS1), located in the short arm of chromosome 7, and chronic hereditary pancreatitis [3]. Since then, over 25 mutations in the PRSS1 gene have been identified (https://www.uni-leipzig.de/pancreasmutation/), although most of them have been sporadic family cases with a small number of family members. In consequence, the association between genotype and phenotype has not been well established for those mutations, except for the most frequent which are the N29I and R122H [4]. Nonetheless, the criteria for the diagnosis of hereditary pancreatitis have been revised and the diagnostic criteria have been updated, including in all cases, the study of mutations in the PRSS1 gene [5, 6].
Trypsin plays an important role at the beginning of the activation cascade of pancreatic enzymes. The acinar cells have a number of mechanisms to protect themselves from the autolysis secondary to a deregulation of trypsinogen activation. One of the main protective mechanisms is the existence of an arginine residue at position 122 (R122) in the PRSS1 gene which allows the autolysis of the trypsin which has been activated at the wrong moment and place, and thus pancreas autodigestion is avoided [7]. Genetic defects in such a position are frequently associated with classic hereditary pancreatitis and are thought to cause the enhanced activation of typsinogen to trypsin [8, 9], or to prevent prematurely activated trypsin from being inactivated by autolysis, resulting in autodigestion and inflammation of the pancreas [10, 11].
The c.346C>T (p.R122C) mutation in the PRSS1 gene was first identified in 2001 by Le Marechal et al. from a DNA analysis of patients with chronic pancreatitis [12]. One year later, Simon et al. [13] also described two members of two generations from the same family who carried the R122C mutation and suffered from chronic pancreatitis. Thereafter, such a mutation has only been described in two other families in separate studies [4, 14].
A characteristic feature of hereditary pancreatitis is a notably increased risk of pancreatic cancer, which is estimated to be 53-fold higher after the age of 50 years in comparison to the general population [15]. A cohort study of 246 patients with hereditary pancreatitis from ten countries with a mean follow-up period of more than 14 years identified 8 patients with pancreatic adenocarcinoma, yielding a standardized incidence ratio (i.e., the ratio of observed to expected pancreatic cancers) of 53.3%. The estimated cumulative risk of pancreatic cancer at age 70 in patients with hereditary pancreatitis approaches 40% [16, 17].
We herein present the largest series of family carriers of the R122C mutation in the PRSS1 gene and describe for the first time, its penetrance and natural history in a northern region of Spain.
PATIENTS AND METHODS
Inclusion Criteria
We included all hereditary pancreatitis patients and their relatives carrying the R122C mutation who were studied at our Gastroenterology Service. Only those relatives of patients with hereditary pancreatitis in whom the R122C mutation was found were subsequently followed up as outpatients and were included in the study. There were 5 relatives having a pancreatic pathology who could not be examined or tested for the R122C mutation and were therefore not included. In total, the study consisted of 41 members of six families from whom DNA samples were available. The R122C mutation in the PRSS1 gene was detected in 22 of the 41 members studied. All members but one of families in which the R122C mutation was detected, compiled a medical history with emphasis on symptoms suggestive of pancreas disease, together with morphological studies and pancreatic functional tests. In one member (the first woman from the second generation in family A, Figure 1), the mutation was found in DNA extracted from the autoptic sample because she died at 63 years of age from pancreatic cancer before undergoing any of the studies carried out in the remaining 21 patients. The morphological studies carried out included transcutaneous abdominal ultrasound, endoscopic retrograde cholangiopancreatography (ERCP), computerized tomography (CT), magnetic resonance imaging (MRI) and endoscopic ultrasonography (EUS). The exocrine functional tests used were pancreatic indirect evidence (Bz-Ty-PABA test, pancreolauryl test and/or fecal chymotrypsin and/or determination of steatorrhea, the Van de Kamer test and, more recently, a triolein breath test marked with 13C). Acute pancreatitis was diagnosed on the basis of an episode of acute abdominal pain together with a three-fold increase of serum amylase above the upper normal range and the “restitutio ad integrum” of the pancreas by morphological and functional pancreatic tests. Chronic pancreatitis was diagnosed when at least one of the following symptoms or signs was present with or without abdominal pain: pancreatic calcification, altered morphology of the main pancreatic duct and/or pathological findings characteristic of chronic pancreatitis in surgical samples.
Figure 1. Genealogic trees for families A, B and C.
In addition to the date of birth, the age at which the patient had the first symptom suggesting pancreas disease, the age at which the diagnosis of chronic pancreatitis was made, the age at which calcification or morphological alteration of the Wirsung conduct or diabetes were first detected, the age at which steatorrhea was detected and the age at which surgery was necessary because of complications from chronic pancreatitis were recorded.
Survey of Carriers and Patients
The recruitment of individuals was conducted in the following manner. When an R122C mutation was detected in a patient, genetic counseling was offered to all first-degree relatives of that patient, and then all first-degree relatives of those who were carriers of the mutation and who consented to the study. Genetic counseling was performed in all subjects after informed consent.
Patients diagnosed with chronic pancreatitis were followed prospectively to the collection of data for the present study or exitus. A visit was carried out annually up to date, or more frequently, if clinical evolution demanded it. In asymptomatic individuals carrying the R122C mutation, a complete clinical history, morphological studies of the pancreas (CT) and tests for assessing the exocrine pancreatic function were carried out, and an annual review was conducted.
Genotyping Studies
DNA was extracted from whole blood samples collected in EDTA tubes, by using the QIAamp DNA blood kit (Qiagen, Hilden, Germany), and exon 3 of the cationic trypsinogen (GenBank accession number M22612; https://www.ncbi.nlm.nih.gov/Genbank/) was amplified by polymerase chain reaction using specific primers 5´-GGTCCTGGGTCTCATACCTT-3´ and 5´- GGGTAGGAGGCTTCACACTT-3´. Rapid screening for the R122C mutation was carried out by AflIII and BstUI restriction endonucleases (New England Biolabs, Ipswich, MA, USA) as previously described [13]. We verified the authenticity of the mutation by sequencing with the same primers used for amplification (CEQ 8000 Genetic Analysis System, Perkin Elmer, Boston, MA, U.S.A.).
Patients
Family A (Figure 1).
Patient A1. A 70-year-old woman, heterozygous for the R122C mutation without toxic habits. Her father was diagnosed with chronic pancreatitis, died from pancreatic cancer, but was not tested for the mutation. Her mother, without pancreatic disease, was not tested. Two brothers and one sister died of pancreatic cancer. The two brothers could not be tested, and the sister was heterozygous for the R122C mutation. Among her four children (all of them male), one son (Patient A2 described below) was diagnosed with chronic pancreatitis and discovered to be heterozygous for the R122C mutation.
Our patient started with abdominal pain at 35 years of age and was diagnosed two years later with chronic pancreatitis following the discovery of pancreatic calcification. At 43 years of age, she developed diabetes. In subsequent years, changes in the main pancreatic duct and steatorrhea were noticed. Thereafter, she suffered from portal hypertension, choledochal stenosis, and renal failure secondary to chronic diabetic nephropathy. She developed pancreas cancer at the age of 69 years
A sister of this patient was a carrier of the R122C mutation as detected from a DNA sample obtained from an autoptic sample since she died from pancreas cancer before having the suspicion of hereditary pancreatitis. She died at 63 years of age but no clinical records were available.
Patient A2. A 22-year-old man, carrier of the heterozygous mutation R122C, without toxic habits. Since 8 years of age, he had had episodes of pain in the left hypochondrium but led a normal life. At 12 years of age, he was admitted to hospital with increased frequency of the painful episodes and the discovery of a cyst on the tail of the pancreas. Based on indirect evidence of alteration of the exocrine pancreatic function (fecal chymotrypsin and PABA test), dilatation of the Wirsung duct and elevated serum amylase (1,270 U/L, reference range: 0-100 U/L), he was diagnosed with an acute inflammatory outbreak of probable chronic pancreatitis. At 14 years of age, pancreatic calcifications were detected for the first time. At 22 years of age, he was suffering from persistent hyperglycemia and episodes of pain. He has not returned to revision since then.
Family B (Figure 1).
Patient B1. A 47-year-old man, homozygous for the R122C mutation, and a smoker of 20 cigarettes per day for 36 to 39 years. He denied alcoholic habits. His mother and a maternal uncle suffered from chronic pancreatitis and died from pancreatic cancer, but were not genotyped. There was consanguinity between his parents (first cousins) but they could not be tested. At 15 years of age, he began with episodes of abdominal pain and was diagnosed with acute pancreatitis together with an isolated pancreatic calcification at 20 years of age. At 36 years of age, episodes of abdominal pain, evident pancreatic calcification, alteration of indirect functional tests and steatorrhea persisted. At 38 years of age, abnormalities of the pancreatic ducts and diabetes were detected. He is the father of two daughters and one son, all three carriers of R122C in heterozygosity, but asymptomatic until now.
Family C (Figure 1).
Patient C1. A 62-year-old man, carrier of the heterozygous R122C mutation, without toxic habits. One brother (Patient C2) was diagnosed with chronic pancreatitis. No additional family history of pancreatic disease was observed. He remained asymptomatic until 32 years of age when he was diagnosed with chronic pancreatitis by the casual finding of pancreatic calcification. At 56 years of age, he was admitted because of pain, jaundice and dilatation of the main bile duct. He died at 62 years of age from pancreatic cancer, as demonstrated in the autoptic exam.
Patient C2. A 71-year-old man, brother of C1, carrier of the heterozygous R122C mutation, and a smoker of 10 cigarettes per day without alcohol intake. He was asymptomatic until 51 years of age when he began with abdominal pain. The study demonstrated a duodenal ulcer, but also pancreas calcifications, changes in the pancreatic ducts and abnormal functioning of the pancreas without steatorrhea. Two years later, he developed mild diabetes mellitus remaining clinically stable to the present, except for worsening diabetes at 66 years of age.
Family D (Figure 2).
Figure 2. Genealogic trees for families D, E and F.
Patient D1. An 8-year-old male, carrier of the heterozygous R122C mutation.
His paternal great-aunt died from pancreatic cancer at 65 years of age but she was not tested. At 4 years old, he started with an episode of idiopathic acute pancreatitis. At 7 years of old, he presented a new episode of severe acute pancreatitis. At this time, morphological and functional pancreatic tests were conducted and no finding suggestive of chronic pancreatitis was observed.
Family E (Figure 2).
Patient E1. A 26-year-old man, without family history of pancreatic disease or personal history of toxic habits. At 10 years of age, he visited his physician because of epigastric pain but no diagnosis was reached. At the age of 19, he suffered an episode of acute pancreatitis and a pancreas divisum was found. After a new episode of acute pancreatitis at 23 years of age, a papillotomy of the papilla minor was undertaken; however, he continued to have occasional episodes of pain. An additional genetic study demonstrated then genetic R122C mutation of the PRSS1 gene in heterozygosis. Morphological studies (including EUS) and functional data carried out until the present have not been suggestive of chronic pancreatitis.
Family F (Figure 2).
Patient F1. A 31-year-old man, carrier of the heterozygous R122C mutation. At 4 years of age, he started with abdominal pain. Ten years later, he was admitted to hospital due to an episode of abdominal pain and a three-fold increase in serum amylase, being diagnosed with acute pancreatitis. At 22 years of age, he had pancreatic calcifications and underwent pancreatic-jejunostomy for pain. Since then, he has been asymptomatic.
STATISTICS
Mean±standard deviation (SD), median range and frequencies were used as descriptive statistics. Continuous and categorical variables were compared using the Mann-Whitney rank sum test. A Kaplan Meier curve and a log rank test were used to evaluate differences in disease-free survival between genders. All statistical tests were carried out using SPSS software (version 13.0). Two-tailed P values less than 0.05 were considered statistically significant.
ETHICS
Informed consent was obtained from each patient included in the study and the study was approved by the Ethical Committee at our centre. The study protocol conforms to the ethical guidelines of the "World Medical Association Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects" adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964, as revised in Tokyo 2004.
RESULTS
Twenty-two (53.7%; 13 males and 9 females) out of the 41 family members who underwent genetic study were carriers of the R122C mutation, and nine of them had developed pancreatic disease. These numbers conferred a penetrance of 40.9% for this mutation.
Two families (A and B) met the clinical criteria consistent with hereditary pancreatitis based on the Gross clinical and epidemiological criteria [2] and were considered to have hereditary pancreatitis before genetic studies were carried out. In the other four families, a diagnosis of hereditary pancreatitis was made when the R122C mutation was detected during the study of a pancreatic disease of unclear etiology, and had no family history which would allow diagnosing hereditary pancreatitis. Seven out of the 13 male carriers (53.8%) of the R122C mutation developed pancreatic disease, but only two out of the nine female carriers (22.2%) suffered from pancreatic disease. The female in family A died before the mutation was detected and she was excluded from the analysis. Therefore, this study deals with 8 carriers of the mutation who developed pancreatic disease.
No significant difference in the cumulative disease-free survival was observed between the 13 men and the 8 women (P=0.104 Figure 3).
Figure 3. Comparison of the cumulative disease-free survival
between men and women analyzed by the Kaplan-Meier and the logrank
tests (P=0.104).
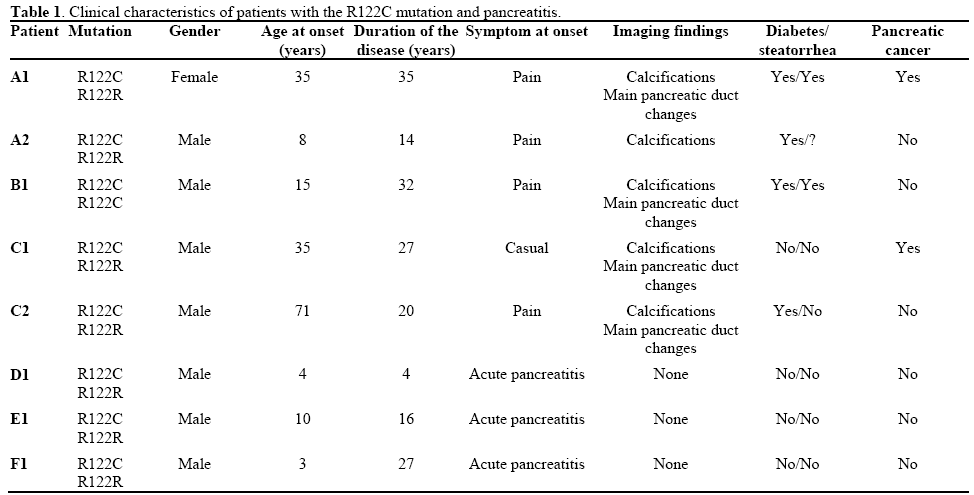
The median age of the last visit of the 8 patients with pancreatitis (43.4 years, range 8-70 years) was similar to that of the 13 individuals with the mutation who were asymptomatic (45.7 years, range: 10-84 years; P=0.812). Globally, the age at symptom onset in the 8 symptomatic carriers was 23.5±16.4 years of age (median: 19 years; range 4-51 years) whereas the age of the 13 carriers of the mutation without disease is now 45.7±24.3 years old (median: 45 years; range: 10- 84 years; P=0.057). However, the age of disease presentation was bimodal: 5 out of 8 symptomatic patients (62.5%) had the first symptoms at 12.0±7.6 years of age (median: 14 years; range: 4-19 years) and the remaining 3 (37.5%) at 40.0±9.8 years of age (median: 37 years; range: 32-51 years). Differences were observed in the form of clinical onset in both groups. Those showing disease symptoms at an earlier age had acute pancreatic inflammation, and those who showed disease symptoms at a more advanced age presented signs of established chronic pancreatitis. Abdominal pain was the most common symptom since 6 (75.0%) out of the 8 symptomatic patients referred to it as the initial symptom. Calcifications developed in 5 (62.5%) out of the 8 symptomatic patients at a mean age of 35.8 years of age (range: 14-56 years), far superior to those without calcification (mean age: 17 years of age; range: 8-26, P=0.245). Five out of the 8 patients (62.5%) developed changes in the pancreatic ducts at a mean age of 44.2 years of age (range: 19-65 years) while the 3 who did not develop them were 17 years of age (range: 8-26 years; P=0.121). Two patients (25.0%) developed steatorrhea during follow-up at 26 and 35 years of disease progression (from the onset of symptoms), respectively; four (50.0%) had not developed steatorrhea at 4, 16, 20 and 27 years of follow-up, respectively, from the onset of symptoms; and in two, data are missing because of not having conducted a functional study. Diabetes developed in five patients (62.5%) at a mean age of 41.4 years (range: 22-53 years). Two patients (25.0%) developed pancreatic cancer at 59 years and 70 years of age, respectively (Table 1). In addition, the patient from family A who died from pancreatic cancer and carried the mutation was not included in Table 1 because of the lack of clinical records.
DISCUSSION
To date, over 25 mutations have been considered to be responsible for hereditary pancreatitis. Most of them have been identified in the PRSS1 gene, with the most common being the R122H and N29I mutations (https://www.uni-leipzig.de/pancreasmutation/). The remaining mutations (A16V, R116C, R122C, N29T, etc.) have been sporadically associated, and clinical studies have not been conducted to establish their penetrance and phenotype. Thus, information about the behavior of these less frequent mutations is lacking. The R122C mutation in the PRSS1 gene has been described in very rare cases and, up to now, only in isolated families. We herein present the largest familial description of the R122C mutation in the PRSS1 gene associated with chronic pancreatitis.
Hereditary pancreatitis is an autosomal dominant disease with incomplete penetrance. This means that this disorder follows Mendelian inheritance of a singlegene mutation, and the knowledge of the penetrance is very important to genetic counseling [18].
In order to minimize ascertainment bias, this study is focused only on those individuals in whom DNA analysis was carried out. With only one exception, where the authors follow up his clinical situation through his relatives, asymptomatic and symptomatic carriers of the mutation are regularly checked as outpatients in our Gastroenterology Unit. The described rate of penetrance of hereditary pancreatitis in carriers for the most frequent R122H and N29I mutations is approximately 80% [18]. However, in our study, only 9 individuals of the 22 who are carriers of the R122C mutation have developed pancreatitis. Thus, the penetrance for the R122C mutation of PRSS1 is 40.9%, which is clearly lower than those previously described.
To our knowledge, our study contains the largest number of patients with the R122C mutation and the lack of a sufficiently large series of individuals with this mutation does not allow us to compare our rate penetrance. However, Carbonell et al. described a family with the R122C mutation in the PRSS1 gene in which the mutation was identified in 3 family members (the father and a brother in addition to the index case) who were asymptomatic carriers which resulted in a penetrance of 33%, similar to that observed in our study [14]. Simon et al. described another family with hereditary pancreatitis, finding the R122C mutation in 4 of the 5 members tested in the two generations studied [13]. Two of them were symptomatic and the other two were not. Thus, penetrance was 50%, slightly higher than ours, but still lower than that found for other mutations in the PRSS1 gene. However, Pfüzer et al. found 2 patients with pancreatitis from 3 in whom the genetic study could be performed, resulting in a penetrance of 67% [4].
We do not know the reason for the difference in the penetrance between the R122H, N29I, and R122C mutations, but several explanations are possible. First, hereditary pancreatitis is a chronic disease and, therefore, penetrance is age-dependent and young asymptomatic individuals can develop the disease later on, increasing the penetrance as time goes by. However, we found that the mean age of disease onset in the symptomatic subjects was significantly lower than that of asymptomatic carriers in the last revision. Furthermore, only 3 people in the first two decades of their life were asymptomatic. Hence, although all three would have developed pancreatitis later on, the prevalence of 50% would continue to be lower than that described for other mutations. Second, the possibility that exogenous factors might have had some influence was not possible in our patients because there was no difference in life habits among carriers with and without pancreatitis. Third, the R122C mutation can induce a less severe alteration in trypsin than other mutations. Fourth, finally, the penetrance of the R122H and N29I mutations was calculated in patients with the disease, but it was not possible to know how many family members were healthy carriers of the mutation and, therefore, the penetrance could be overestimated because of ascertainment bias.
Curiously enough, Archer et al. [19], in a mouse model of hereditary pancreatitis generated by transgenic expression of R122H trypsinogen, demonstrated advanced lesions at 1 year of age in up to 40% transgenic mice, which is a frequency similar to the penetrance in our series.
Moreover, such a low penetrance found for the R122C mutation suggests that this mutation is a necessary, but not sufficient factor to induce pancreatitis. Other factors may influence the pathogenesis of hereditary pancreatitis. Among them, gender seems to be the most relevant from our data, as depicted in Figure 3. Although the sex distribution of the R122C mutation in our study can be considered as normal, all but one of the carriers developing pancreatitis were men. Accordingly, in the other three previous studies commented on above [4, 13, 14], all but two of the carriers of the R122C mutation who developed pancreatitis were men. However, in a series of 153 patients with hereditary pancreatitis in which 82 were men and 71 women, twenty of the 153 had the R122H mutation and 5 had the mutation N29I mutation [5]. There does not seem to be gender susceptibility in the production of hereditary pancreatitis secondary to the R122H and N29I mutations, or in those patients defined as suffering from hereditary pancreatitis by clinical criteria [20, 21]. In the present study, 77.8% of individuals who developed pancreatitis and carried the R122C mutation were male, although there was no gender predominance in subjects with the R122C mutation, neither symptomatic nor asymptomatic. The predominance of males in the development of pancreatitis with the R122C mutation has not previously been established but it is necessary to confirm our findings with a larger series of patients. The onset of pancreatic disease showed a bimodal distribution, and the clinical manifestations were also different depending on the age of onset. In patients in whom the disease manifested itself at an earlier age, clinical manifestations of acute pancreatitis without morphologic or functional alterations suggestive of chronic pancreatitis dominated. However, when the disease manifested itself at a more advanced age, chronic pancreatitis had already been established. This was previously suggested by Sibert et al. [22] and suggests that this mutation is capable of provoking subclinical changes in a significant percentage of patients with the R122C mutation (37.5%) reaching advanced stages of pancreatic disease, including cancer, as occurred in one of our patients. The study of Keim et al. conducted on patients with the R122H and N29I mutations also suggests that the age of disease onset shows a bimodal distribution while the second peak (18-24 years) is earlier than that found by us for the R122C mutation [23]. On the other hand, Otsuki et al [5] also described a bimodal distribution in symptom onset (the first peak between 11 and 15 years old, and the second between 26 and 40 years old, respectively) in 25 patients with the R122H and N29I mutations, in agreement with data observed in our patients. Sibert et al. suggest that the second peak of age could be related to toxic habits, such as alcohol or smoking [22], but this does not seem to be our case because there was no difference in toxic habits between early or late-onset patients.
Finally, we found three cases of pancreatic cancer in the 22 individuals, carriers of the R122C mutation from the 6 families studied. The probability of developing pancreatic cancer among R122C carriers is 757.6 times higher than in the general population. Curiously, Lowenfels et al. observed that, in patients with hereditary pancreatitis with a paternal inheritance pattern, the cumulative risk of pancreatic cancer was higher than in those with a maternal inheritance pattern [15].
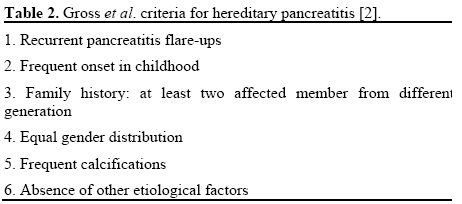
In addition, our data indicate the lack of appropriateness of the criteria established by Gross et al. for the diagnosis of hereditary pancreatitis [2]. Thus, four of the families included in our analysis did not meet criterion 3 and none of them met criterion 4 (Table 2). Furthermore, one of the patients affected (patient E1), together with the R122C mutation, had the 5T variable of CFTR and pancreas divisum, and, as a consequence, he did not meet the criterion 6. However, our results are in agreement with the criteria suggested by Otsuki et al. [5], adding, however, the R122C mutation to criterion 1 as another possible mutation to be described in the future.
In summary, in this paper, we described the prevalence of the R122C mutation in the PRSS1 gene and analyzed the relationship of genotype-phenotype in six unrelated families. The two most important conclusions from this study were clearly the lower prevalence of pancreatic disease associated with this mutation as compared to those described in other mutations of the same gene, and the predominance of males with the R122C mutation who developed the phenotype of pancreatitis.
Conflict of interest
The authors have no potential conflicts of interest
References
- Comfort MW, Steinberg AG. Pedigree of a family with hereditary chronic relapsing pancreatitis. Gastroenterology 1952; 21:54-63. [PMID 14926813]
- Gross JB, Gambil EE, Ulrich JA. Hereditary pancreatitis. Description of a fifth kindred and summary of clinical features. Am J Med 1962; 33:358-64. [PMID 13902224]
- Whitcomb DC, Gorry MC, Preston RA, Furey W, SossenheimerMJ, Ulrich CD, et al Hereditary pancreatitis is caused by a mutation in the cationic trypsinogen gene. Nat Genet 1996; 14:141-5. [PMID 8841182]
- Pfützer R, Myers E, Applebaum-Shapiro S, Finch R, Ellis I, Neoptolemos J, et al. Novel cationic trypsinogen (PRSS1) N29T and R122C mutations cause autosomal dominant hereditary pancreatitis. Gut 2002; 50:271-2. [PMID 11788572]
- Otsuki M, Nishimori I, Hayakawa T, Hirota M, Ogawa M, Shimosegawa T; Research Committee on Intractable Disease of the Pancreas. Hereditary pancreatitis: clinical characteristics and diagnostic criteria in Japan. Pancreas 2004; 28:200-6. [PMID 15028953]
- Applebaum-Shapiro SE, Finch R, Pfützer RH, Hepp LA, Gates L, Amann S, et al. Hereditary pancreatitis in North America: the Pittsburgh-Midwest Multi-Center Pancreatic Study Group Study. Pancreatology 2001; 1:439-43. [PMID 12120221]
- Chen JM, Montier T, Férec C. Molecular pathology and evolutionary and physiological implications of pancreatitisassociatedcationic trypsinogen mutations. Hum Genet 2001; 109:245-52. [PMID 11702203]
- Witt H, Luck W, Becker M. A signal peptide cleavage site mutation in the cationic trypsinogen gene is strongly associated with chronic pancreatitis. Gastroenterology 1999; 117:7-10. [PMID 10381903]
- Sahin-Tóth M. Hereditary pancreatitis-associated mutation asn(21) -->ile stabilizes rat trypsinogen in vitro. J BiolChem 1999; 274:29699-704. [PMID 10514442]
- Rinderknecht H, Adham NF, Renner IG, Carmack C. A possible zymogen self-destruct mechanism preventing pancreatic autodigestion. Int J Pancreatol 1988; 3:33-44. [PMID 3162506]
- Várallyay E, Pál G, Patthy A, Szilágyi L, Gráf L. Two mutations in rat trypsin confer resistance against autolysis. BiochemByophysRes Commun 1998; 243:56-60. [PMID 9473479]
- Le Maréchal C, Chen JM, Quéré I, Raguénès O, Férec C, Auroux J. Discrimination of three mutational events that result in a disruption of the R122 primary autolysis site of the human cationic trypsinogen (PRSS1) by denaturing high performance liquid chromatography. BMC Genet 2001; 2:19. [PMID 11734061]
- Simon P, Weiss FU, Sahin-Toth M, Parry M, Nayler O, LenfersB, Schnekenburger J, et al. Hereditary pancreatitis caused by a novel PRSS1 mutation (Arg-122 -->Cys) that alters autoactivation and autodegradation of cationic trypsinogen. J BiolChem 2002;277:5404-10. [PMID 11719509]
- Carbonell P, Glover G, Fernández JA, Ramírez M, Marín C, Castellanos G, Parrilla P. Hereditary pancreatitis caused by a new mutation in the trypsinogen gene. Report of a family. Cir Esp 2006, 79:252-4. [PMID 16753108]
- Lowenfels AB, Maisonneuve P, Cavallini G, Ammann RW, Lankisch PG, Andersen JR, et al. Pancreatitis and the risk of pancreatic cancer. International Pancreatitis Study Group. N Eng J Med 1993; 328:1433-7. [PMID 8479461]
- Lowenfels AB, MaisonneuveP, DiMagno EP, Elitsur Y, Gates LK Jr, Perrault J, et al. Hereditary pancreatitis and the risk of pancreatic cancer. International Hereditary Pancreatitis Study Group. J Natl Cancer Inst 1997; 89:442-6. [PMID 9091646]
- Lowenfels AB, Maisonneuve P, Whitcomb DC. Risk factors for cancer in hereditary pancreatitis. International Hereditary Pancreatitis Study Group. Med ClinNorth Am 2000; 84:565-73. [PMID 10872414]
- Rosendahl J, Bödeker H, Mössner J, Teich N. Hereditary chronic pancreatitis. Orphanet J Rare Dis 2007; 2:1. [PMID 17204147]
- Archer H, Jura N, Keller J, Jacobson M, Bar-Sagi D. A mouse model of hereditary pancreatitis generated by transgenic expressionof R122H trypsinogen. Gastroenterology 2006; 131:1844-55. [PMID 17087933]
- Amann ST, Gates LK, Aston CE, Pandya A, Whitcomb DC. Expression and penetrance of the hereditary pancreatitis phenotype in monozygotic twins. Gut 2001; 48:542-7. [PMID 11247900]
- Creighton JE, Lyall R, Wilson DI, Curtis A, Charnley RM. Mutations of the cationic trypsinogen gene in patients with hereditary pancreatitis. Br J Surg 2000, 87:170-5. [PMID 10671922]
- Sibert JR. Hereditary pancreatitis in England and Wales. J Med Genet 1978; 15:189-201. [PMID 671483]
- Keim V, Bauer N, Teich N, Simon P, Lerch MM, Mössner J. Clinical characterization of patients with hereditary pancreatitis and mutations in the cationic trypsinogen gene. Am J Med 2001; 111:622-6. [PMID 11755505]




