Keywords
Chemotherapy, Cancer, Regional Perfusion; Pancreatic Neoplasms
Abbreviations
CR complete remission; DDP cisplatin; FOLFIRINOX folinic acid(leucovorin)(LV), 5-fluorouracil (5-FU), irinotecan, and oxaliplatin combination chemotherapy regimen; GEM gemcitabine; GCSF granulocyte colony stimulating factor; LV leucovorin (folinic acid); LV-FUDR leucovorin and floxuridine 5-day chemotherapy regimen; MIC mitomycin C; OS Overall Survival (Mean±SD); PD progressive disease; PR partial remission; SD standard deviation
INTRODUCTION
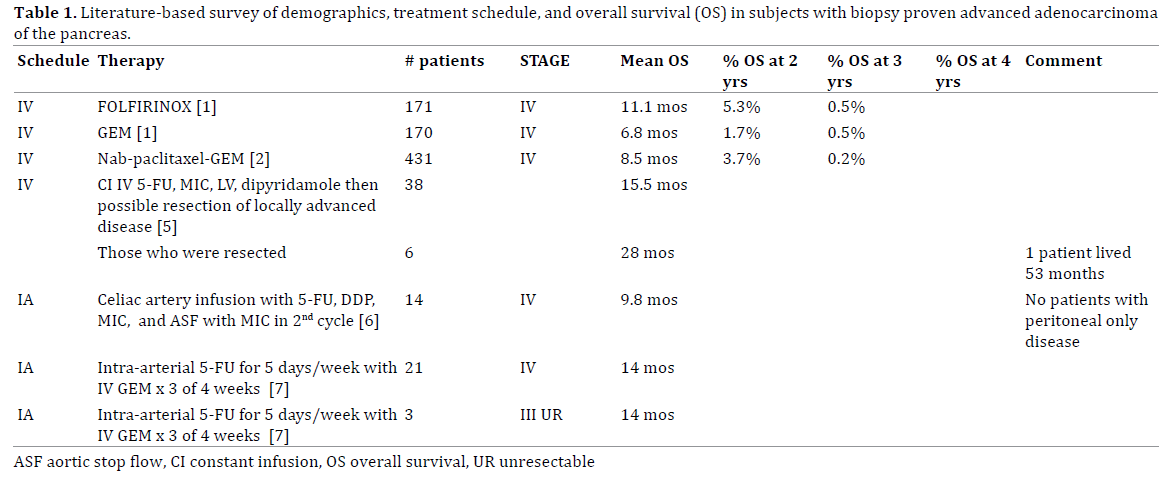
The prognosis of patients with advanced adenocarcinoma of the pancreas is very poor, for the SEER data indicates that only 2.4% survive 5 years. Most patients with newly diagnosed metastatic pancreatic cancer receive either IV FOLFIRINOX [1] or GEM / nabpaclitaxel chemotherapy [2]. The use of drugs directly into the hepatic artery however increases the intensity of the chemotherapy drug during its first flow through the body’s circulation; unusual toxicities occur whenever cytotoxic drugs are given intra-arterially as compared to the toxicities expected for the traditional intravenous routes. When a drug is given intra-arterially to the liver which metabolizes it, a first-pass effect is present, in which very high drug levels are seen initially. This perfusion results in high, although short duration, drug concentrations in the liver tumors. This perfusion using MIC was first utilized by YZ Patt et al. [3] in colon cancer patients based upon reported MIC levels in dogs measured by Hashimoto [4] who measured MIC levels in tumors and in the liver. There are some previously published articles where perfusion chemotherapy was used in pancreatic cancer. These are presented in Table 1 which presents results of both IV therapies as well as perfusion therapy.
FUDR is a metabolite of 5-FU that is a substrate for intracellular thymidine kinase. Following the administration of FUDR, the cells can by a single enzymatic step produce the inhibitor of thymidylate synthetase 2'-Deoxy-5-fluorouridine 5'-Monophosphate (FdUMP). Prior studies using LV-FUDR by intravenous administration suggested a lower incidence of toxic reactions [8] compared to that after LV-5FU given according to the regimen of Doroshow et al. [9]; Greater clinical efficacy [10] was also demonstrated as patients who had tumor progression during previously given LV-5FU therapy, could have clinical responses with LV-FUDR therapy.
PATIENTS REPORTED
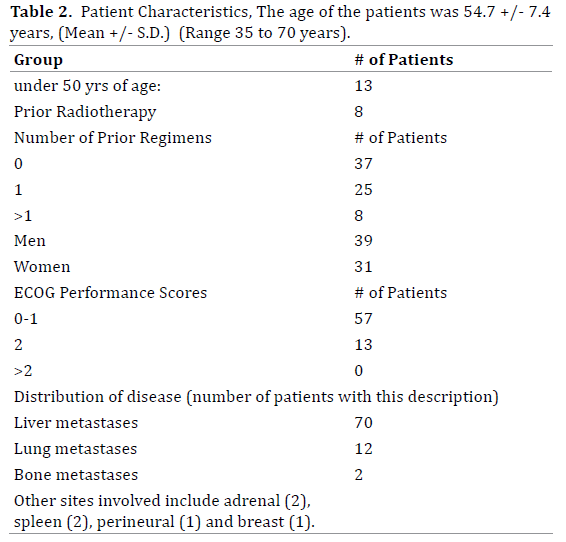
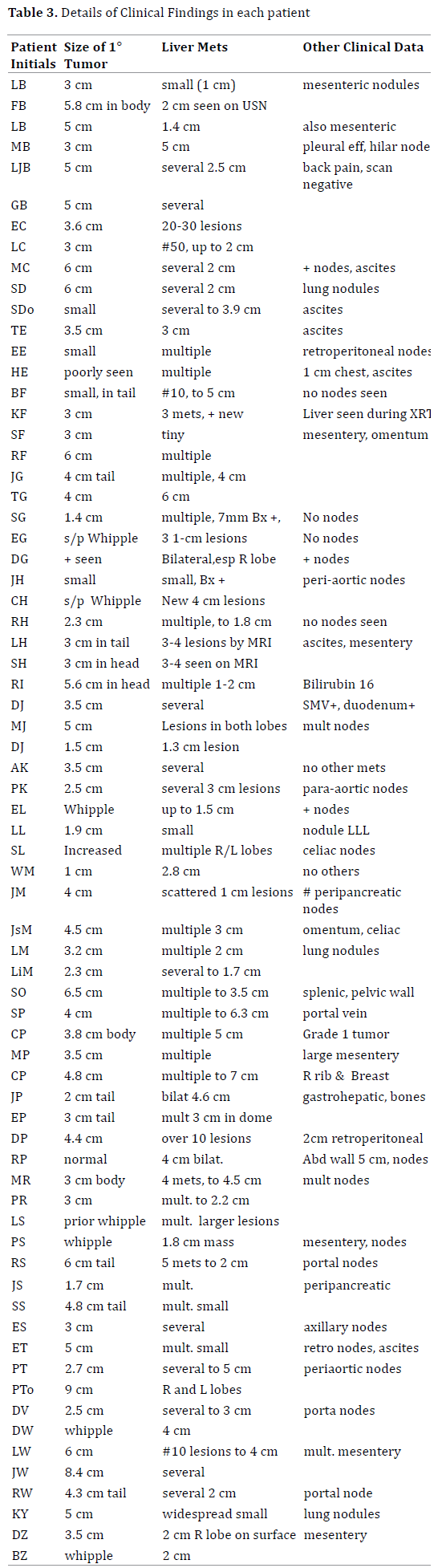
All patients had adenocarcinoma of the pancreas with pathologically- confirmed liver metastases. Overall patient characteristics are shown in Table 2, and specific data of each patient is shown in Table 3. Thirty-seven patients had newly diagnosed advanced disease with liver metastases while 33 had a lesser stage previously but who then developed liver metastases after prior chemotherapy or radiotherapy; All patients had a performance status 0-2, serum creatinine <1.5 mg/dL, and total bilirubin <1.5 mg/ dL; No patient had known pleural disease however seven had duodenal invasion, eight had mesenteric disease, and twelve had other sites of metastatic disease.
METHODS
All patients were treated with monthly MIC and DDP via the hepatic artery, with five daily infusions of 4-hour IV LV-FUDR injections. FUDR injection iv push were given one hour before the completion of each day’s LV infusion. The hepatic artery catheter was placed via the Seldinger technique with the insertion of a catheter percutaneously into the femoral artery and advanced in a retrograde direction. An arteriogram was initially done to identify the best approach to perfuse the pancreatic tumor and its metastases. Usually, the catheter was then advanced super-selectively into the right or left hepatic artery with the goal of treating both the pancreatic primary and the liver metastases. Some catheters were placed into the splenic artery for those tumors originating in the tail of the pancreas. The percutaneous site was then bandaged and compressed with a sand bag to prevent bleeding; the patient was then transferred to the medical floor where the intraarterial infusions were administered over a 5-hour period. At the end of the infusions, the radiologist came to bedside, removed the catheter, and applied compressive dressings and sandbags, which were removed 5 hours later by the nursing staff. All patients were restricted to a maximum of 6 monthly doses of MIC as cumulative marrow intolerance is commonly seen and other investigators have reported extreme toxicities when cumulative lifetime MIC doses have approached 100 mg/m2 [11]. Monthly DDP doses were always 40-50 mg/m2. Dexamethasone and serotonin antagonist (5-HT3 receptor antagonist) were given on the day of hepatic artery therapy. Injections of GCSF began on the 5th day of each cycle, and continued daily generally for 10 days unless improvement in the WBC was evident before that time. To minimize toxicities, each patient was instructed in pain control and in the use supportive care measures for nutrition support and stomatitis control. Allopurinol mouthwash helped in stomatitis prevention, and was utilized hourly × 3 times daily, beginning at the time of the FUDR dose.
The initial dose of IV FUDR was 800 mg/m2/day. The initial dose of hepatic artery MIC was 8 mg/m2. When marrow involvement was expected or if the patient had previously received chemotherapy or radiotherapy, poor marrow tolerance was expected and smaller doses MIC were started. With a serum bilirubin elevation up to 1.5 mg/ml, 20% less MIC was used, and MIC was avoided when the initial bilirubin exceeded 2 mg/mL. Therapy is escalated to the largest dose of MIC and of FUDR that was tolerated, as determined by each patient’s side effects in the prior chemotherapy cycle. MIC therapy was increased to a dosage of at least 10 mg/m2 or higher whenever possible, however no patient tolerated a dosage higher than 13 mg/m2. The usual toxic side effect of MIC is leucopenia and thrombocytopenia, usually at its worst 14 days after therapy; the dose of subsequent MIC was increased whenever the preceding nadir platelet level exceeded 50,000.
Monthly DDP doses were always 40-50 mg/m2. Patients were treated with monthly combination therapy, but the intra-arterial portion of the therapy was stopped after a maximum of 6 cycles and LV-FUDR continued monthly until relapse was seen or otherwise stopped.
Follow–up Studies
All patients had weekly CBC and chemistry studies. Radiographic studies were done at three-month intervals. The primary end points of this retrospective study were evidence of tumor response, overall survival, and the prevalence and grade of treatment related CTCAE graded side effects. Overall survival was measured from the date of the first cycle of therapy to patient death. Tumor progression was determined if there was radiological evidence of more than 25% increase in the product of cross diameter of any measurable tumor site. Date of last followup was July 1, 2014, and living patients were censored at this date for survival. Tumor responses were graded as being a complete response if all measurable signs of tumor were no longer seen. Partial remission was determined when the product of cross diameters measured on radiological studies had shrunken 50%.
Progressive disease was declared if any site of tumor increased its product of cross diameters by 25%. Treatment-related toxicities were graded using the National Cancer Institute Common Toxicity Criteria, version 3 (2003)(CTCAE).
ETHICS
Review of the patient’s data was approved by the IRB which is an exempted study since only retrospective data is presented. This report of therapy was approved by the Midwestern Institutional Review Board and complied with the International Ethical Guidelines for Biomedical Research involving Human Subjects. All patients provided written informed consent with a MRMC hospital consent for intra-arterial chemotherapy to which was appended an information sheet of the specific therapies and expected toxicities of this regimen.
STATISTICS
Statistics of these results followed a distinctly nonnormal distribution; we include the median, mean, and S.D. to more accurately describe the result. Survival was estimated using the Kaplan Meier Method.
RESULTS
Table 4 shows the mean survival (OS) of various groups. All 70 patients had metastatic pancreatic cancer with liver metastases. The 37 without prior therapy had an OS of 25.0±39.6 months, median 10.5 months, while 33 patients with tumor progression after prior chemotherapy did not do as well, an OS of 8.6±7.4 months, median 6.3 months.
There was no statistical difference in the survival of men and women. As shown in Table 5, the OS of the 18 women who had no prior chemotherapy was 29.5±45 months with a median of 11.3 months. The 13 women who had prior chemotherapy had an OS of 11.6±9.9 months with a median of 8.9 months.
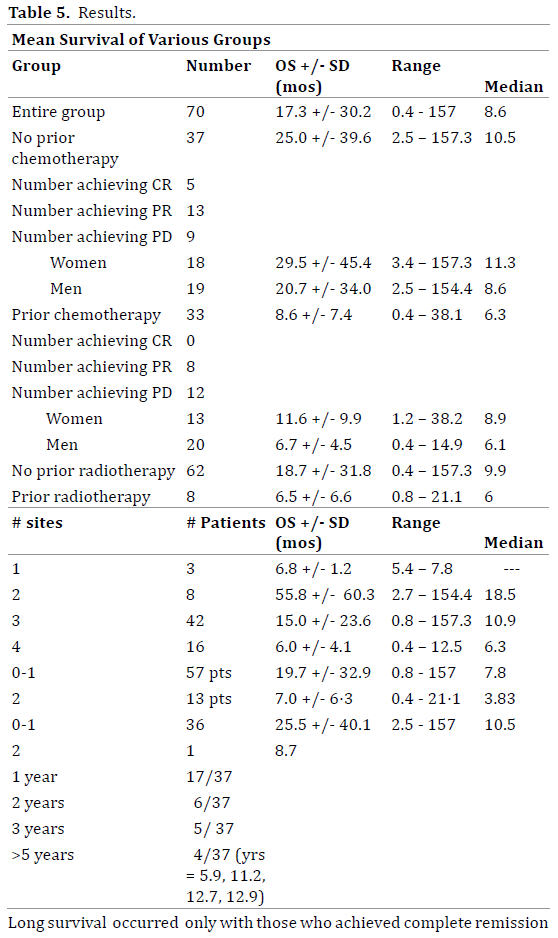
The 19 men without prior chemotherapy had an OS of 20.7±34 months, with a median of 8.6 months. The 20 men with prior therapy had an OS of 6.7±4.5 months with a median of 6.1 months.
Of the 37 patients without prior chemotherapy, 5 achieved a CR, 13 achieved a PR, while 9 had directly progressive disease. Of the 33 patients who had previously received therapy in general did worse for none achieved a complete remission, 8 achieved partial remissions, and 12 had directly progressive disease; There was worse survival in those with more extensive tumor spread with a higher number of metastatic sites and in those with ECOG status of 2 (Figure 1).
Figure 1. Patients without prior chemotherapy had a statistically significant survival advantage –Logrank Two Tailed P = 0.0049, where patients with prior
chemotherapy had a mean survival of 8.6 months, with a 2-year and 5 year cumulative survival rate of 6% and 0% which compares to newly treated patients
with a mean survival of 25.0 months, and a 2 and 5 year cumulative survival rate of 37.8 % and 10.8 %.
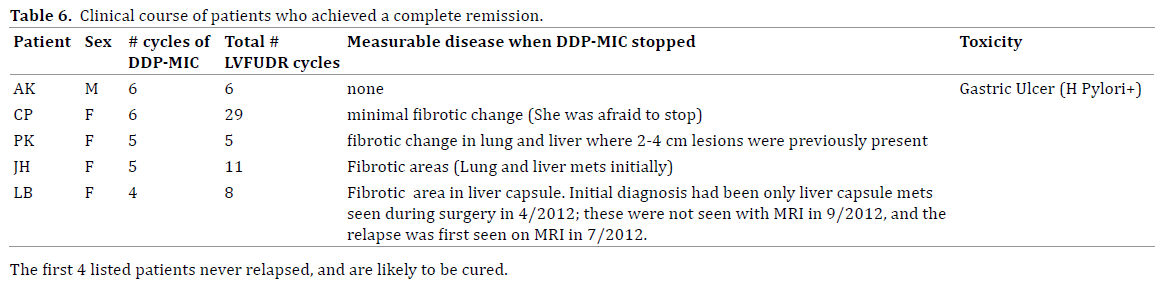
Of the entire group of 70 patients, five achieved a complete remission, four are yet in remission as of July 1, 2014 ranging from 72-157 months after initiating therapy. These are shown in Table 6. Once the hepatic artery therapy was stopped, there was a significant risk that tumor would relapse. One example of this was the patient who tolerated only 3 cycles of hepatic artery therapy before thrombocytopenia became excessive.
LV-FUDR was given, and the 2 cm pancreatic mass kept shrinking so that she achieved a complete remission with normal CT scans for 4 months. Unfortunately, multiple 1 cm liver metastases were then seen and she lived only 1 month further.
Ten patients received only one cycle of chemotherapy and did not return for a variety of reasons: Three patients had too advanced disease and died within 2 months without interim chemotherapy. Three patients died with a drug related death as leucopenia and thrombocytopenia were present at the time of sepsis due to cholangitis which occurred 2 weeks after intra-arterial therapy. Two patients had hematemesis related to the hepatic artery infusion, in whom gastroscopy noted excess perfusion or necrosis of the gastric mucosa, apparently due to local gastric flow through a tiny artery which is thought to extend from the hepatic artery which brought MIC directly onto the mucosa; Further hepatic artery infusions to these patients were not given. Two patients were dissatisfied with the severity of stomatitis associated their first cycle, and refused to continue therapy.
Eight patients with prior radiotherapy had an OS of 6.5±6.6 months. This contrasts markedly with the results of the 65 patients without prior radiotherapy, who had a mean OS of 18.7±31.7 months. All patients who survived five or more years had no prior radiotherapy.
Safety and Toxicity
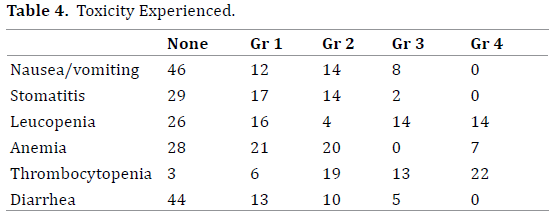
There were significant treatment related morbidities associated with this regimen, including potentially severe leucopenia and thrombocytopenia with recovery within the month; Marrow support with GCSF was routinely utilized, however there was minimal evidence of amelioration of leucopenia; thrombocytopenia thus became a dose-limiting toxicity. Each month, the dose of FUDR was increased grade 2 stomatitis occurred, however stomatitis could generally be minimized with the use of daily allopurinol mouthwash hourly × 3; patients who elected to avoid a mouthwash cycle rarely repeated their avoidance. Nausea and vomiting, hand-foot syndrome, renal proteinuria, and other toxicities were unusual.
One patient was responding after 3 cycles of therapy but then died in an automobile accident. All other deaths were associated with multiple organ failure due to the disease process and occurred after recovery from myelosuppression and other early therapy- related gastrointestinal symptoms.
DISCUSSION
Previously published chemotherapy regimens for adenocarcinoma of the pancreas with liver metastases are limited. The intravenous regimens such as FOLFIRINOX and GEM/nab-paclitaxel have not reported any patient yet surviving more than 4 years. The intra-arterial regimens are reported in much more limited studies, and may have a higher OS. The approach of chemotherapy followed by possible resection has limited applicability, but nevertheless provided a mean survival of 28 months while one patient survived 53 months.
The terms of complete response or partial response are primarily of interest to the treating physician during a course of therapy, for therapy is usually stopped or changed at the time of tumor progression. The elimination of tumor minimizes weight loss and usually provides relief from back pains which are referred pains from the retroperitoneal tumors or from the liver, and thus quality of life is improved. The goal of the patients and of the doctors of course is a true cure, which has not previously been reported.
The greatest benefit in most chemotherapy regimens is usually seen in patients with no prior therapy, and the results here are not different.
There are unique problems with this therapy. Patients with large bilateral liver metastases may have shrinkage on the side which is well perfused by an available hepatic artery while if an artery for the other side cannot be easily, those tumors may grow. Additionally, liver metastases may shrink while mesenteric metastases were growing.
One particular benefit however is that the plan of 6 cycles of hepatic artery therapy and IV therapy, followed by monthly intravenous therapy alone allows the identification of those patients whose tumors were sensitive to the LV-FUDR monthly therapy, for these tumors continue to shrink after the hepatic artery therapy is stopped in whom myelosuppression is no longer a problem.
This regimen provides a small but measurable probability of prolonged survival in patients, and markedly prolonged survival and possibly even a cure in those patients who were able to achieve a complete remission.
Conflict of Interest
The authors have no conflict of interest to declare
References
- Conroy T, Desseigne F, Ychou M, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. NEJM 2011; 364:1817-25. [PMID: 21561347]
- Von Hoff D, Ervin T, Arena F, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. NEJM 2013; 369:1691-703. [PMID: 24131140]
- Patt YZ, Wallace S, Freireich EJ, Chuang VP, Hersh EM, Mavligit GM. The palliative role of hepatic arterial infusion and arterial occlusion in colorectal carcinoma metastatic to the liver. TheLancet, 1981;317:349-351. [PMID: 17024393]
- Hashimoto Y. Fundamental investigations on local chemotherapy for liver cancer. Arch Jap Chir 1978;47:302-318. [PMID: 677999]
- Todd KE, Gloor B, Lane JS, Isacoff WH, Reber HA. Resection of locally advanced pancreatic cancer after downstaging with continuous-infusion 5-fluorouracil, Mitomycin C, leucovorin, and dipyridamole. Journal of GastrointestSurg 1998; 2:159-166. [PMID: 9834413]
- Aigner KR. Regional chemotherapy-editorial review article. Regional Cancer Treatment 1994; 2:55-66. [PMID: 415961]
- Takamori H, Kanemitsu K, Tsuji T, et al. 5-Fluorouracil intra-arterial infusion combined with systemic gemcitabine for unresectable pancreatic cancer. Pancreas 2005; 30: 223-226. [PMID: 17582098]
- Levin RD, Gordon JH, Simonich W, Mellijor A, Sanchez R, Williams RM.Phase I clinical trial with fluoxuridine and high-dose continuous infusion of leucovorin calcium. Journal of Clinical Oncology 1991; 9:94-99. [PMID: 1824639]
- Doroshow JH, Leong L, Margolin K, et al. Refractory metastatic breast cancer: Salvage therapy with fluorouracil and high-dose continuous infusion leucovorin calcium. Journal of Clinical Oncology 1989; 7:439-444. [PMID: 2784492]
- Levin RD, Gordon JH. Fluorodeoxyuridine with continuous leucovorin infusion. A phase II clinical trial in patients with metastatic colorectal cancer. Cancer 1993;72:2895-2901. [PMID: 8221555]
- Wu DC, Liu JM, Chen YM, et al. Mitomycin C induced hemolytic uremic syndrome: a case report and literature review. Jpn J ClinOncol 1997; 27:115-118. [PMID:9152802]


