Gurudath Gundurao Sreekantamurthy1, Mohammad Juned Khan1, Thangavelu Sethuraman Ramesh Kumar1, Palanisamy Senthilnathan2, Chinnasamy Palanivelu3, Sreekanth Basavaraju4, Sharath Kote Gowdra Shivamurthy1, Santhosh Palve1, Suganya Dhinakaran1, Nityanand Sharma1,Piyush Pradeeprao Marudwar1
Departments of 1Medical Gastroenterology, 2Hepato-Pancreatico-Biliary Surgery, 3Surgical Gastroenterology, and 4Radiodiagnosis and Interventional Radiology, GEM Hospital and research centre Pvt. Ltd, Coimbatore, India
- *Corresponding Author:
- Gurudath GS
Department of Medical Gastroenterology
GEM Hopsital and research centre pvt Ltd.
45A Pankaja Mill road
Ramanathapuram
Coimbatore-641045
Tel + 91-9500935498
E-mail gurudathsdumc@gmail.com
Received December 05th, 2016 - Accepted January 06th, 2017
Keywords
Ampulla of Vater; Pancreas; Pancreatitis; Chronic
Abbreviations
CT computed tomography; GI gastro-intestinal;
HP hemosuccus pancreaticus
INTRODUCTION
Hemosuccus pancreaticus (HP) is a rare and potentially
life threatening upper gastrointestinal (GI) bleed, defined
as bleeding from ampulla of Vater through pancreatic
duct. It was first described in 1931 by Lower and Farrel
who reported a primary spleenic aneurysm rupture into
the main pancreatic duct while the name hemosuccus
pancreaticus was given by Sandblom in 1970. It is usually
occurs due to the rupture of a visceral aneurysm into the
main pancreatic duct; splenic artery pseudoaneurysm
associated with chronic pancreatitis represents the leading
cause of this condition [1, 2]. HP has been estimated to
occur in about one in 1,500 cases of GI bleeding [3].
CASE REPORT
A Fifteen-year-old-male patient who is a known case
of chronic pancreatitis without endocrine and exocrine
insufficiency, admitted for melena with upper abdominal
pain since 2 days. Patient had melena 2 weeks back also for
which he was hospitalised in our institution and evaluated with upper GI endoscopy, colonoscopy and CT angiogram
which were normal and considered it as obscured overt
GI bleed. There was no history of NSAID intake. Clinical
examination revealed pallor, tachycardia and severe
epigastric tenderness. Other systemic examination
nothing contributory. Blood investigations showed
haemoglobin of 7 gms/dL, normal leucocyte and platelet
count, significantly elevated serum amylase (657 U/L)
and lipase (786 U/L), normal liver and renal function test.
Peripheral smear showed microcytic and hypochromic
anemia. Transabdominal ultrasonography revealed acute
on chronic pancreatitis with pancreatic calcifications.
Etiological workup done for chronic pancreatitis
showed normal triglycerides levels, normal calcium and
parathyroid harmone levels. There was no pancreatic
divisum on MRCP and IgG4 levels were normal. Upper GI
endoscopy (Figure 1) revealed altered blood in stomach
with adherent clot in the ampulla. After thorough saline
wash, ampulla showed blood stained bile and hemosuccus
pancreaticus was suspected. CT abdomen showed
evidence of chronic pancreatitis with pseudo-aneurysm
(7x6 mm) in the ventral division of inferior pancreaticoduodenal
artery (Figure 2). Later patient underwent
angiography through right femoral approach, superior
mesenteric artery was cannulated with 5F Sim 1 catheter
and selective angiography confirmed a pseudoaneurysm in
the ventral branch of inferior pancreaticoduodenal artery
supplying mid body of pancrease (Figure 3). Selective
angioembolization done at neck of pseudoaneurysm
(Figure 4). Check angiogram revealed no filling of
pseudoaneurysm.
Figure 1. Retroflexion view of upper GI scopy in D2 showing adherent
clot over ampulla.
Figure 2. Showing small pseudoaneurysm involving ventral division of
inferior pancreatico-duodenal artery with diffuse pancreatic parenchymal
calcifications.
Figure 3. Angiography showing pseudoaneurysm in the ventral division
of inferior pancreaticoduodenal artery.
Figure 4. Post coil embolization at the neck of pseudoaneurysm. No filling
of pseudoaneurysm seen in check angiography.
DISCUSSION
This Fifteen-year-old boy, known case of chronic
pancreatitis who was previously admitted for evaluation
of melena and considered it as obscure overt GI bleed.
Subsequently at present admission he was diagnosed
as HP due to psuedoanuerysm in inferior pancreaticoduodenal
artery. Upper GI endoscopy revealing adherent
clot over the ampulla of Vater and blood stained bile
flow gave us clue towards the diagnosis. This clinical
scenario emphasises the intermittent nature of bleed
and importance of examining the ampulla for upper GI
bleed evaluation in pancreatitis patients. During a bout
of pancreatitis, pancreatic proteolytic enzymes digest the
arterial wall causing pseudoaneurysm which may bleed
into pancreatic duct of Wirsung, raising the intraductal
pressure causing to severe abdominal pain. As the duct is
decompressed through ampulla, patient will have upper
GI bleed and relief in pain which explains the crescendodecrescendo
type of abdominal pain. Ductal blockage also causes increase in serum amylase and lipase levels.
This logical analysis of pathogenesis explains the triad
of abdominal pain (crescendo-decrescendo nature),
elevated serum pancreatic enzymes and GI bleed which
is seen in HP patients [4, 5]. The most common cause for
pseudoaneurysm is acute or chronic pancreatitis [6]. Other
frequent causes are trauma [7], rupture of true aneurysm
[8], pancreatic tumors [9], arteriovenous malformations
[10]. The splenic artery is the most common artery involved
(60-65%) followed in decreasing order of frequency by
gastroduodenal (20-25%), pancreaticoduodenal (10-
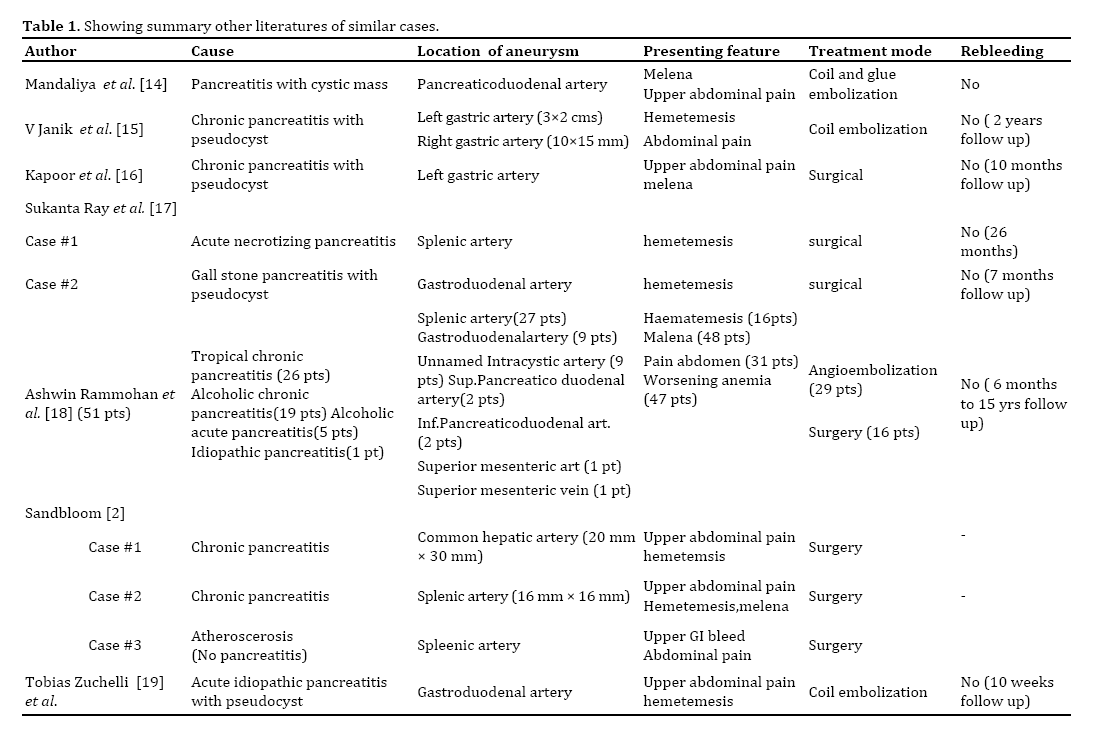
15%), hepatic (5-10%) and left gastric arteries (2-5%) [11, 12, 13, 14, 15, 16]. Table 1 gives details about other similar
cases . These data highlights the fact that inferior pancreaticoduodenal
artery is less commonly involved which is involved in the present case. Ultimately, angiography is
the diagnostic reference standard, identifies the causative
artery, delineates the anatomy and allows for therapeutic
intervention. The sensitivity of angiography is usually
greater than 90% [8, 13, 15, 17].There are two potential
therapeutic approaches: interventional radiological
procedures and surgery. If the source of hemorrhage is
found by angiography then interventional radiographic
procedures are the first choice for initial management
with immediate good results in 79-100% of the cases
and an overall success rate of 67%. The techniques for
intervention include embolization via prosthetic material,
balloon tamponade and stent placement. Coil embolization
is the most frequently described technique which is done
our patient also. It stimulates thrombus formation in the
pseudoaneurysm [17, 18]. Surgical treatment is indicated
when there is uncontrolled bleeding, persistent shock,
failure of embolization, rebleeding after embolization, or
when initial angiography shows no abnormal findings. The
various surgical procedures include distal pancreatectomy
and splenectomy, central pancreatectomy, intracystic
ligation of the blood vessel, aneurysm ligation and bypass
graft. Most surgical procedures have shown success rates
of 70-85%, at the same time operative mortality rates of
10-50% have been reported in the literature. The rate of
rebleeding after surgery is 0-5% [17, 19, 20, 21].
Conclusion
HP is an arterial bleed, often life threatening if
diagnosis is delayed. This case highlights the importance of
examining major papilla for evidence of bleed in patients
of pancreatitis presenting with upper GI bleed, which gives
us clue for early diagnosis and intervention.
Conflict of Interest
Authors declare no conflict of interests for this
article.
References
- Lower WE, Farrell JI. Aneurysm of the splenic artery: Report of a case and review of the literature. Arch Surg 1931; 23:182-190. [PMCID: PMC1250840]
- Sandblom P. Gastrointestinal hemorrhage through the pancreatic duct. Ann Surg 1970; 171:61-66. [PMID: 5308032]
- Suter M, Doenz F, Chapuis G, Gillet M, Sandblom P. Haemorrhage into the pancreatic duct (Hemosuccus pancreaticus): recognition and management. Eur J Surg 1995; 161:887-892. [PMID: 8775630]
- Traverso LW, Damus PS, Longmire WP Jr. Pancreatitis of unusual origin. Surg Gynecol Obstet 1975; 141:383-386. [PMID: 1162566]
- Sakorafas GH, Sarr MG, Farley DR, Que FG, Andrews JC, Farnell MB. Hemosuccus pancreaticus complicating chronic pancreatitis: an obscure cause of upper gastrointestinal bleeding. Langenbecks Arch Surg 2000; 385:124-128. [PMID: 10796050]
- Maus TP. Pseudoaneurysm hemorrhage as a complication of pancreatitis. Mayo Clin Proc 1993; 68:895-6.
- Kim SS, Roberts RR, Nagy KK, Joseph K, Bokhari F, An G, Barrett J. Hemosuccus pancreaticus after penetrating trauma to the abdomen. J Trauma 2000; 49:948-50. [PMID: 11086791]
- Etienne S, Pessaux P, Tuech JJ, Lada P, Lermite E, Brehant O, Arnaud JP. Hemosuccus pancreaticus: a rare cause of gastrointestinal bleeding. Gastroenterol Clin Biol 2005; 29:237-42. [PMID: 15864172]
- Shinzeki M, Hori Y, Fujino Y, Matsumoto I, Toyama H, Tsujimura T, Sakai T, et al. Mucinous cystic neoplasm of the pancreas presenting with hemosuccus pancreaticus: report of a case. Surg Today 2010; 40:470-3. [PMID: 20425553]
- Williams DM, Shetzline MA, Guarisco SA, Branch MS. Presumed arteriovenous malformation mimicking hemosuccus pancreaticus of Santorini's duct with normal pancreatic anatomy. Gastrointest Endosc 1996; 44:348-50. [PMID 8885362]
- Heath DI, Reid AW, Murray WR. Bleeding pseudocysts and pseudoaneurysms in chronic pancreatitis. Br J Surg 1992; 79:281. [PMID: 1637385]
- Woods MS, Traverso LW, Kozarek RA, Brandabur J, Hauptmann E. Successful treatment of bleeding pseudoaneurysms of chronic pancreatitis. Pancreas 1995; 10:22-30. [PMID: 7899456]
- Yeh TS, Jan YY, Jeng LB, Hwang TL, Wang CS, Chen MF. Massive extra-enteric gastrointestinal hemorrhage secondary to splanchnic artery aneurysms. Hepatogastroenterology 1997; 44:1152-1156. [PMID: 9261616]
- Mandaliya R, Krevsky B, Sankineni A, Walp K, Chen O. Hemosuccus Pancreaticus: A Mysterious Cause of Gastrointestinal Bleeding. Gastroenterology Res 2014; 7:32-37. [PMID: 27785267]
- Janík V, Pádr R, Keil R, Lischke R, Pafko P. Hemosuccus pancreaticus - endovascular treatment by transcatheter embolization of both gastric arteries. Cas Lek Cesk 2008; 147:538-41. [PMID: 19177737]
- Kapoor S , Rao P, Pal S, Chattopadhyay TK. Hemosuccus pancreaticus: an uncommon cause of gastrointestinal hemorrhage. A case report. J Pancrease (online) 2004; 5:373-6 [PMID: 15365206]
- Ray S, Das K, Ray S, Khamrui S, Ahammed M, Deka U. Hemosuccus Pancreaticus Associated with Severe Acute Pancreatitis and Pseudoaneurysms: A Report of Two Cases. J Pancreas (Online) 2011; 12:469-472. [PMID: 21904073]
- Rammohan A, Palaniappan R, Ramaswami S, Perumal SK, Lakshmanan A, Srinivasan UP, Ramasamy R, et al. Hemosuccus Pancreaticus: 15-Year Experience from a Tertiary Care GI Bleed Centre. ISRN Radiol 2013; 191794:6. [PMID: 24959558]
- Zuchelli T, Alsheik E, Bhandari B, Ringold D. A Unique Case of Hematemesis in a 17-Year-Old Female. ACG Case Rep J 2014; 1:151–53. [PMCID: PMC4435304]
- Han B, Song ZF, Sun B. Hemosuccus pancreaticus: a rare cause of gastrointestinal bleeding. Hepatobiliary Pancreat Dis Int 2012; 11:479-488. [PMID: 23060392]
- Zyromski NJ, Vieira C, Stecker M, Nakeeb A, Pitt HA, Lillemoe KD et al. Improved outcomes in postoperative and pancreatitis-related visceral pseudoaneurysms. J Gastrointest Surg 2007; 11:50-55. [PMCID: PMC3341460]





