Keywords
Health systems strengthening; Township health system; Primary health care; Hard-to-reach villages; Global alliance for vaccines and immunizations; Myanmar
Background
Myanmar, a lower middle-income country with Gross National Income (GNI) per capita of US$ 1,280 in 2014 [1], is in the midst of vibrant political and economic transformation. In 2011, General Government Expenditure on health was as low as 1% of general government expenditure resulting in high out-of-pocket health payments by households, equaling 79% of total health expenditure [2]. Inadequate investment in the health system in the last few decades resulted in weak health infrastructure, particularly primary health facilities, in hard-to-reach villages, hampering access to health services.
As a result, by 2011, Myanmar had high level of Under Five and Infant Mortality rates (62.4 and 49.3 per 1000 live births). Health status also varied across geographic, economic and social settings [2,3], worse health status was noted among the disadvantage States and Regions.
Inequity in access to primary health care (PHC) is observed in developing countries including Myanmar [4]. Likewise, Myanmar’s multiple indicator cluster survey 2009-2010 [5] indicates higher coverage of antenatal care in urban (98.3%) than rural villages (91%). Prevalence of skilled birth attendance (SBA) rate is higher among the richest quintiles in urban communities and mothers with secondary or higher education, than those who are less educated, poor and live in rural areas. Institutional delivery rate is also highest in urban areas with 68.9% in Yangon. However, a smaller inequity gap is noted on DPT3 coverage across wealth quintiles, rural and urban areas [5], due to its high coverage as a result from “reaching every community” initiatives.
While geographical and financial barriers are common factors restricting poor and rural populations from accessing health services [6], supply side capacity gaps in providing essential health services play a larger role. Supply side capacity gaps differ at different levels of the health system; experiences from Timor Leste, South Africa and Myanmar demonstrate weakest supply side capacity at primary health care level [7-9].
Currently under the political leadership of National League of Democracy (NLD), Myanmar has expressed strong commitment to improve the health of its population by accelerating progress towards universal health coverage in a phased manner with initial efforts to strengthen primary healthcare.
Strengthening country’s national health system with supply side system readiness to provide decent quality services at the township level and below, with pro-poor policy interventions is the central highlight of Myanmar’s National Health Plan (NHP) 2017-2020 [10]. The country is gearing towards phase wise expansion of Basic Essential Package of Health Services (EPHS); prioritizing its reach to the neediest townships defined by their geographic location, economic and social profiles.
Such reform agenda demands strengthening of primary health system with adequate investment in cadres of front line health workforce, financing, infrastructure, medical supplies, to enable supply-side readiness and deliver quality health services at the township level. Therefore, evidence from real life experiences on primary health system strengthening will contribute to the current design of PHC reform.
In 2011, a health systems strengthening programme was piloted in 20 hard-to-reach townships of Myanmar with support from the Vaccine Alliance. Program reached the hard-to-reach population with outreach health services, and introduced a Hospital Equity Fund to provide free hospital-based MCH services for poor mothers and children. Prior to the programme implementation, a baseline assessment was conducted in 2010 and early 2011, and programme performance was assessed after two years, in 2013.
This paper reviews the baseline health system situation of 20 hard-to-reach townships in 2010, and assesses the outputs and outcomes of programme implementation in 2013. Further, it draws key lessons from implementing interim strategy of Primary health care strengthening by this programme, to inform current primary health care reform in Myanmar.
The Program Objective and Design
In 2011, in order to fast track Millennium Development Goal (MDG) commitments, the Ministry of Health (MOH) aimed to increase DPT3 coverage and SBA in hard-to-reach townships, to 90% and 80%, respectively by 2015. A four year health system-strengthening programme (GAVI HSS) supported by GAVI the Vaccine Alliance, was implemented to realize this vision.
Selection of townships
There were 180 hard-to-reach townships having DPT 3 coverage and Skilled Birth Attendances (SBA) rate below 80% and 60%. The programme was implemented in a phased manner responding to the resource constraints and prioritization needs. In 2011, the MOH implemented the programme in 20 out of 180 townships, where there were capacities to implement the program.
Assessments: Baseline in 2010, and two years after pilot in 2013
Prior to the program implementation, a team from ministry of health reviewed the situation of health systems in 20 hard-to-reach townships and generated the baseline data. This baseline data guided the design of health system strengthening programme activities to reach the hard-to-reach population in these 20 townships.
Township health team in all 20 townships identified and mapped hard-to-reach villages in their locality, using geographical, economic and social criteria to support programme implementation. This exercise was done through a consultative process, engaging MOH, the World Health Organization (WHO) and other relevant stakeholders. Accordingly, programme activities including outreach service delivery and HEF were designed and implemented. Volunteer health workers were recruited and trained to support basic health staff (BHS) in outreach service delivery (Box 1).
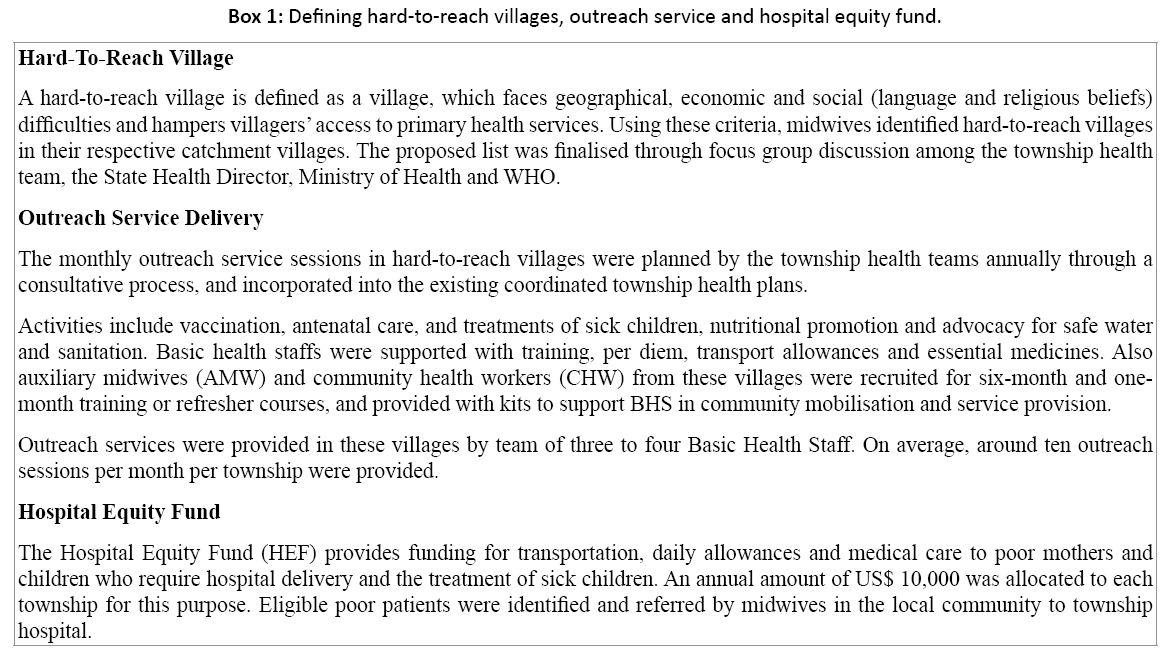
Box 1: Defining hard-to-reach villages, outreach service and hospital equity fund.
After two years of program implementation, in 2013, a Performance Assessment was conducted to review the program progress. Routine data collected for outreach service delivery and the hospital equity fund in the 19 hard-reach townships were analysed (program implementation disrupted in one township due to civil unrest). Focus group discussions were conducted at two sample townships out of the 20, to understand program performance on the ground. Further, key primary health care data maintained at the Health management and Information system unit (HMIS) of ministry of Health and Sports were analysed to review program output.
Study Methods
Findings from baseline assessment of 20 hard-to-reach townships in 2010-2011 were reviewed to understand township health system situation. Programme outputs after 2 years, in 2013, are assessed particularly based on the routine monitoring data for the coverage of outreach health activities, contributions by hospital equity fund, and the data maintained by health information management system (HMIS) of the ministry of health for key PHC indicators.
In-depth interviews were conducted with 26 and 22 key informants of two selected townships, namely Nyaungshwe township in Taunggyi district of the Shan state and Yedashe township in Taungoo district of Bago region of Myanmar. The key informants were township medical officers and basic health staffs working at the township hospitals, rural health centers and sub-centers [11]. The authors also made field observations in these two townships, to witness on the ground programme performance.
Results
Hard-to-reach areas in 20 townships: Baseline status in 2010
For several decades, government expenditure on health was 1% of total government spending; budget allocation for infrastructure development and health workforce distributions favored tertiary care [2]. One third of rural health centers and sub-centers did not have one health worker trained to provide pre-natal care and there were vaccine shortages. Limited capacities to detect anemia in pregnancy and urine protein were common in Rural Health Centres (RHCs) and sub-RHCs [9].
Findings from baseline assessment highlight high out-ofpocket payments, equally 80% of total health spending, which prevented most people and the poor from accessing health care. Primary health care facilities lacked adequate supply of essential medicines and equipment. Only 8 (7%) out of 108 RHCs met the thirteen-health workers standard. In almost 50% of RHCs, each midwife was responsible for a 4,000-10,000-catchment population. Static health facility coverage was low and 19% of sub centres had no sheltered premises for service provision, forcing the midwives to provide services from the village administrative office or the house of village leaders.
Midwives had neither adequate kits nor transport facilities for outreach services; although there were a few projectfunded but non-functioning motorbikes. The government did not subsidise maintenance and petrol for the self-purchased motorcycles serving the communities.
These PHC service gaps, described in Box 2, along with high-level poverty, illiteracy, ethnicity and geographical remoteness, calls for urgent PHC strengthening.
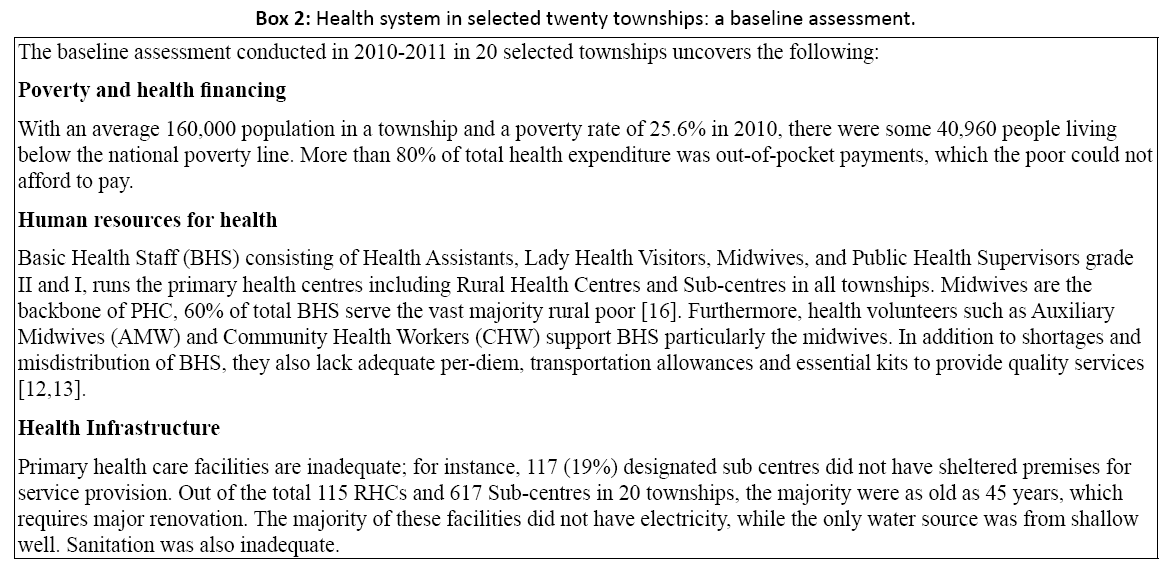
Box 2: Health system in selected twenty townships: a baseline assessment.
Hard-to-reach areas in 20 townships: Relevant changes after two years of program implementation
Performance assessment in 19 townships (excluding programme disruption in one township due to civil unrest) in 2013 highlights several positive changes.
Outreach service delivery
Providing frontline health workers with basic equipment, medical supplies and allowances motivates them to perform well in these hard-to-reach villages. In 2012, each township delivered an average of 123 sessions of outreach services per annum or 10 sessions per month.
These outreach services to hard-to-reach communities, boosted coverage of prenatal care, SBA and immunization for pregnant women and children. All 19 townships demonstrated increased coverage of antenatal care, 15 demonstrated increased skilled birth attendance and 11 demonstrated increased 2nd dose of tetanus toxoid in pregnancy and Bacillus Calmette-Guérin (BCG) in newborns.
Recruitment, training and contribution by AMWs and CHWs
Recruitment and training of volunteers such as Auxiliary Midwives (AMWs) and Community Health Workers (CHWs) from the hard-to-reach villages addresses the health workforce gaps. They assisted midwives in deliveries and mobilised the community for health education, immunisation and MCH services. Older health volunteers living in their own village and speaking the local languages had higher probability to serve the communities longer [12,13]. Nonetheless, adequate supply of outreach kits, support of transportation allowance, supervision and training are critical to retain them and maximize their contributions.
Financial risk protection
In 2013, HEF supported 1,327 poor pregnant women in these twenty townships with delivery difficulties and obstetric emergencies that could have otherwise led to maternal deaths.
However, utilisation rates varied across hospitals in these townships, despite equal distribution of US$ 10,000 per township. By the end of June 2013, 14 out of 20 township hospitals utilised more than 95% of the allocated fund. Supply side factors such as hospital size, staff strength, attitude and skills of hospital staff, and demand side factors such as geographical distance between villages and township hospital, and public awareness influenced uptake of HEF by the poor women and children.
Programme outputs
Overall Programme outputs are described in Table 1.
Table 1: Change of coverage rate between 2013 and 2010, percentage points.
| |
ANC |
TT2 |
SBA |
DTP3 |
BCG |
ORT |
Sanitation |
| Of total 20 townships |
| Townships demonstrated increased coverage |
19 |
11 |
15 |
7 |
11 |
4 |
9 |
| Townships demonstrated decreased coverage |
1 |
8 |
5 |
12 |
6 |
6 |
11 |
| No changes |
0 |
1 |
0 |
1 |
3 |
10 |
0 |
| Average changes, percentage points between 2013 and 2010 |
| Townships with increased coverage |
19 |
10 |
18 |
9 |
16 |
4 |
7 |
| Townships with decreased coverage |
-37 |
-11 |
-11 |
-17 |
-16 |
-3 |
-8 |
Source: Performance Assessment of GAVI-HSS Interventions in 20 townships, 2014 [10]
Trend analysis of MCH service coverage, comparing prior to the GAVI HSS programme (2008 to 2010) and after the GAVI HSS Programme (2011 to 2013) indicated a significant coverage increase in prenatal care. The coverage is over 80% in 2013 in all townships.
In 2013, a high coverage of 2nd dose of Tetanus Toxoid, ranging from 70% to 90% was noted in many townships; most townships showed increased SBA coverage between 50% and 70%. DPT3 coverage was also high (80-90%) in many townships. BCG coverage was mostly higher than 80% and homogenous across 19 townships. Oral rehydration therapy (ORT) coverage among children under five years was very high and homogeneous across townships, between 90% and 100%
Notably two townships (Htilin and Hsipaw), where 62% and 51% of their total villages were hard-to-reach had demonstrated significant improvement in antenatal care (ANC) coverage. On the other hand, all indicators in Maungdaw Township decreased drastically, due to unexpected civil unrest and security challenges, which hindered effective programme implementation.
Improvement of these service coverage indicators was the result of a small investment by the GAVI HSS Program of USD 1.8 per capita in the hard-to-reach villages of these townships.
Discussion
A functioning PHC system is an essential platform for achieving health-related sustainable development goals [14,15]. Yet in reality, lack of infrastructure, equipment and medicines on the supply side and geographical remoteness and poverty on the demand side are significant barriers for the poor to access the needed health services, as revealed by these townships
Primary health strengthening in low resource setting can ensure equitable access to vital health services for the hard-to reach population. Experience from the GAVI HSS programme implementation in Myanmar suggests that outreach services offer a strategic interim option to deliver essential health services in hard-to reach communities on a regular basis. Although favorable outcomes emerged from the outreach service programme, the government’s long-term vision and commitment towards establishing static PHC services are critically needed. This will ensure sustainable access to health services in these communities. Basic health staffs, CHW and AMW volunteers perform better even in these difficult circumstances when they are well equipped and motivated.
HEF prevented the deaths of a thousand poor women and children who would have died due to life-threatening obstetric conditions. The Fund could be considered an entry point for scaling up the government budget for health, and making progressive realization towards universal health coverage. However, a policy on providing financial risk protection alone may not work; parallel policies are needed to focus on geographical extension of functional PHC facilities operating with adequate numbers of committed front-line health workers, medical supplies, equipment and supportive health volunteers.
Conclusion
Despite these favorable outcomes, a donor-funded program is not sustainable, unless the government significantly commits to invest more in PHC system strengthening and financial risk protection in Myanmar (Box 3).
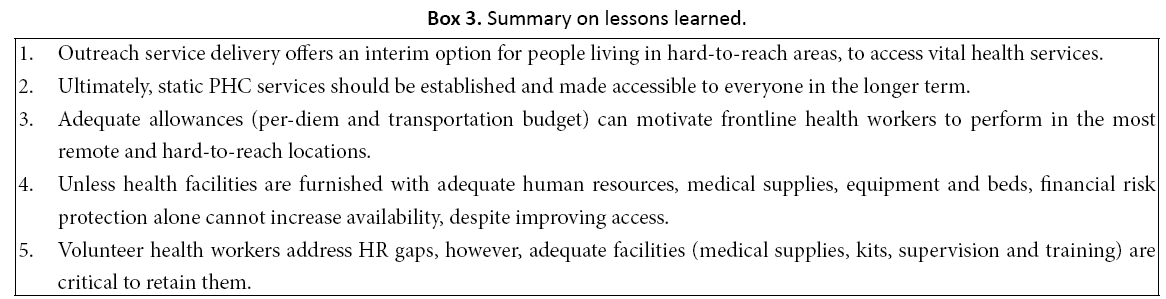
Box 3: Summary on lessons learned.
Acknowledgement
The authors thank the MOH, the Republic of the Union of Myanmar, and WHO Country Office Myanmar, for organising this assessment. We thank all the Township Medical Officers, basic health workers and health system strengthening officers, of 20 sample townships in Myanmar for their kind contribution and support. Appreciation also goes to the GAVI HSS and HMIS team at the MOH, for kindly providing us with the data on PHC indictors in these townships.
Funding Support
GAVI Health System Strengthening support to Myanmar to improve the functions of primary health care; mid term assessment was conducted in 2013 for which manuscript has drawn on.
Authors' Contributions
SW, WP and VT contributed significantly in the assessment design. SW and WP did literature review and prepared the first draft; VT reviewed the draft; MLN provided inputs to the draft; all authors involved in the assessment and field visit. Manuscript was read and agreed by all authors.
Ethics Approval
The study was conducted as a part of routine program monitoring. Hence, the Ministry of Heath, the Republic of the Union of Myanmar waived the ethical clearance. Waiver letter is shared as “the additional file 1 waiver letter”. Informed consents were sought and protection of confidentiality was strictly followed.
References
- https://data.worldbank.org/country/myanmar?view=chart
- https://www.wpro.who.int/asia_pacific_observatory/hits/series/mmr/en/
- Tin N, Lwin S, Kyaing NN, Htay TT, Grundy J, et al. An approach to health strengthening in the Union of Myanmar. Health Policy 2010; 95: 95-102.
- Rule J, Ngo DA, Oanh TTM, Asante A, Doyle J, et al. Strengthening primary health care in low-income countries and middle-generating evidence through evaluation. Asia Pac J Public Health 2014; 26: 339-348.
- https://www.unicef.org/myanmar/MICS_Report_2009-2010.pdf
- Mills A, Ataguba JE, Akazili J, Borghi J, Garshong B, et al. Equity in financing and use of health care in Ghana, South Africa, and Tanzania: Implications for paths to universal coverage. Lancet 2012; 380: 126-133.
- Alonso A, Brugha R. Rehabilitating the health system in east Timor after conflict: A shift from NGO to government leadership. Health Policy Plan 2006; 21: 206-216.
- Lehmann U. Strengthening human resources for primary health care: Primary Health Care, systems support. South African Health Review 2008: 163-177.
- MOH. Nationwide service availability and readiness assessment (SARA). Ministry of Health and Sports. The Republic of the Union of Myanmar 2015.
- https://mohs.gov.mm/Main/content/publication/national-health-plan-2011-2016-english-version
- https://www.searo.who.int/myanmar/documents/performanceassessmentreport_part1.pdf?ua=1
- Sangay W. Auxiliary midwives in hard to reach rural areas of Myanmar: Filling MCH gaps. BMC Public Health 2016; 16.1: 914.
- Angkana S. Community health worker in hard-to-reach rural areas of Myanmar: Filling primary health care service gaps. Hum Resour Health 2016; 14: 64
- Buse K, Hawkes S. Health in the sustainable development goals: Ready for a paradigm shift? Global Health 2015; 11: 1.
- World Health Organization. WHO global strategy on people-centred and integrated health services: Interim report 2015.
- https://mohs.gov.mm/content/publication/list?category=Annual%20Public%20Health%20Statistics&pagenumber=1&pagesize=40

