Mahesh Kumar Goenka, Ashish Kumar Jha, Nisha Kapoor, Usha Goenka
Institute of Gastro Sciences, Apollo Gleneagles Hospital. Kolkata, India
- *Corresponding Author:
- Mahesh K Goenka
Institute of Gastro Sciences; Apollo Gleneagles Hospital; Kolkata,
700054; India
Phone: +91-332.320.3040
Fax: +91-332.320.5218
E-mail: mkgkolkata@gmail.com
Received January 5th, 2012 - Accepted February 20th, 2012
Keywords
Adhesives; Cyanoacrylates; Enbucrilate; Liver Cirrhosis; Pancreatic Fistula; Pancreatitis, Chronic
INTRODUCTION
Pancreatic fistulae are uncommon but grave complication of acute or chronic pancreatitis. They may also occur following abdominal surgery or trauma. Internal pancreatic fistulae are most commonly seen with alcohol related chronic pancreatitis and can involve any part of the pancreatic duct [1]. Reported incidence of pancreatic fistula varies widely because of the use of different definition/criteria in these studies. Bragg et al. reported an incidence of pancreatic fistula in 2% of patients with acute pancreatitis [2]. Chebli et al. found that an internal pancreatic fistula occurs in 7.3% of patients having chronic pancreatitis [3]. The reported incidence of pancreatic fistula formation following partial pancreaticoduodenectomy, left pancreatectomy and pancreatic trauma are 12.9%, 13.0% and 11.9% respectively [4]. We present a relatively new modality of endoscopic therapy for internal pancreatic fistula.
CASE REPORT
A 59-year-old male presented with painless progressive distension of abdomen of three months duration. He had been consuming 30 g of alcohol daily for the last 20 years. Clinically he was anicteric, afebrile and had tense ascites. The hematological and biochemical investigations revealed hemoglobin of 14.4 g/dL (reference range: 13.0-17.0 g/dL), white blood cell count of 10,500 cells/mm3 (reference range: 4,000- 10,000 cells/mm3) (70% polymorphonuclear cells), bilirubin of 0.9 mg/dL (reference range: 0-1 mg/dL), AST of 60 IU/L (reference range: 10-42 IU/L) and ALT of 53 IU/L (reference range: 10-40 IU/L); rest of the blood parameters were normal. Abdominal computed tomography (CT) revealed enlarged caudate and left lobes of liver with relatively smaller right lobe, heterogeneous pancreatic parenchyma, collaterals and marked ascites (Figure 1). Ascites was drained and fluid analysis revealed total leukocyte count of 3,360 cells/mm3 (60% polymorphonuclear cells), protein of 1.0 g/L, albumin of 0.2 g/L, amylase of 116,963 IU/L and adenosine deaminase of 7 U/L. Ascitic fluid cultures were negative. Esophagogastroduodenoscopy showed grade II esophageal varices, small gastric fundal varix and mild portal hypertensive gastropathy. Endoscopic ultrasound (EUS) revealed evidence of chronic pancreatitis and ascites. Diagnosis of internal pancreatic fistula was made and the patient was taken up for endoscopic retrograde cholangiopancreatography (ERCP). Magnetic resonance cholangiopancreatography (MRCP) could have delineated the pancreatic ductal anatomy but not done because of a definite diagnosis of pancreatic ascites due to high fluid amylase in presence of CT scan and EUS evidence of chronic pancreatitis. Pancreatogram revealed a leak from distal part of pancreatic duct (Figure 2). Pancreatic sphincterotomy was done. A cannula was placed next to the fistula, flushed with normal saline and one mL of N-butyl-2- cyanoacrylate glue (Histoacryl®, B. Braun, Tuttlingen, Germany) was injected at the fistula site. Immediately after injection of glue, there was a bit of resistance noted on attempt to withdraw the cannula which was removed with a sharp tug. The check pancreatogram revealed sealed leak (Figure 3). A 7 Fr x 9 cm plastic pancreatic stent was placed in the pancreatic duct. The repeat ascitic fluid amylase was found to be 229 IU/L. He subsequently received low dose of diuretics as well and over the next one week ascites has resolved. His pancreatic stent was removed after 3 weeks and check pancreatogram was normal.
Figure 1. CT scan at the level of uncinate process of pancreas
showing free fluid, localized fluid collection on left side (arrow) and
collaterals around the collection.
Figure 2. Pancreatogram showing leak (red arrow) from distal
pancreatic duct. Note: guide wire (purple arrow).
Figure 3. Check pancreatogram showing main pancreatic duct with
sealed leak.
DISCUSSION
The management of internal pancreatic fistula conventionally included giving complete rest to the pancreas by keeping the patient nil by mouth, parenteral nutrition and external drainage of fluid, if a large collection is present. Subsequently octreotide was added to the above regimen. This therapy requires prolonged hospital stay of up to 4-6 weeks, is expensive and still shows suboptimum success rate [5].
Endoscopic therapy has added a new armamentarium for managing pancreatic fistulas. The aim of endotherapy is to reduce the intrapancreatic duct pressures. The extensively used endoscopic modalities include sphincterotomy, sphincterotomy with stenting, and nasopancreatic drain placement. Successful resolution of fistula has been noted in approximately 90% cases managed by endotherapy [6, 7, 8, 9, 10]. The idea during stent placement is to generally bridge the fistula site which is however not possible in case of leaks from pancreatic tail area. Moreover, dilatation of ductal strictures and removal of calculi can be performed during endotherapy. Endotherapy may be coupled with external drain for large fluid collection. Endotherapy has also been effective in lowering the morbidity and in-hospital stay. However, endoscopic therapy is less effective in leaks from pancreatic tail and excluded pancreatic duct syndrome.
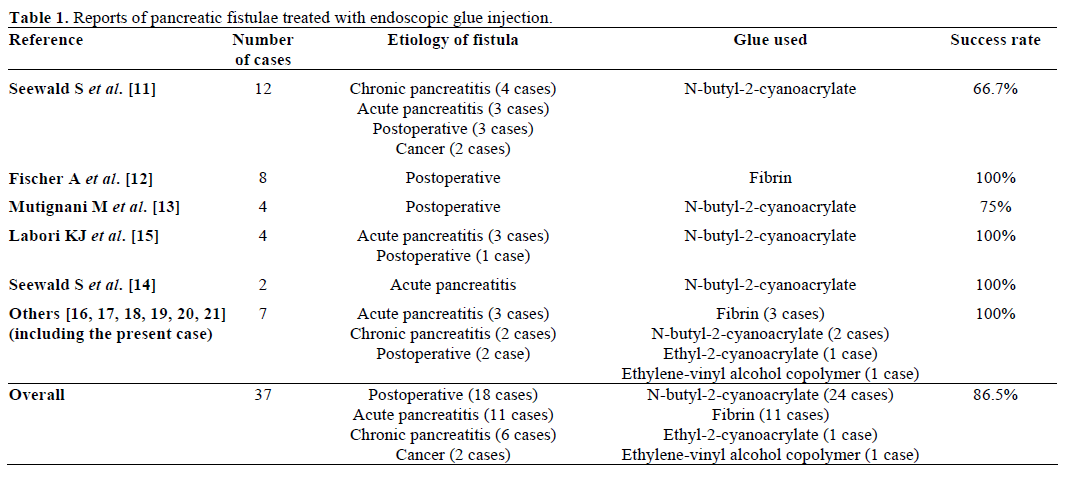
Seewald et al. reported a case series of 12 patients wherein N-butyl-2-cyanoacrylate was injected into the fistulous tract using a catheter during ERCP. The closure of fistula was seen in 8 out of 12 patients (66.7%). Though one person died, it was unrelated to the procedure [11]. Fischer et al. have shown successful closure of 8 out of 8 patients of postoperative pancreatic fistula with the use of fibrin glue [12]. Advantages of N-butyl-2-cyanoacrylate are that we can monitor the injection by mixing with lipiodol and it is more stable than fibrin glue [11]. Mutignani et al. reported 4 patients in whom Glubran® 2 (General Enterprise Marketing, Viareggio, Lucca, Italy) (N-butyl-2-cyanoacrylate with methacryloxysulpholane) was used as the sealant. Closure of fistula was seen in 3 out of 4 cases [13]. In another report, Seewald et al. have shown the closure of pancreatic fistula in 2 patients of acute pancreatitis with the endoscopic application of N-butyl-2-cyanoacrylate [14]. In a recent report, 4 patients with pancreatic fistulas that failed to respond to conservative treatment were successfully treated with N-butyl-2-cyanoacrylate [15]. Overall, approximately 36 similar cases have been described in which endoscopic treatment with fibrin sealants (n=11) or cyanoacrylate (n=25) was used to close the fistulas (Table 1) [11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21]. The potential fears are of pancreatitis, pulmonary embolism, fever and abscess formation. However, vascular embolization is less likely when being used for fistula closure. There is no fear that glue will stick to catheter or stent as it hardens immediately. Because of underlying liver cirrhosis, any surgical intervention including tail of pancreas resection with splenectomy would have been difficult in our patient. Therefore, glue injection possibly was good way out. This modality of treatment definitely warrants larger controlled trial to determine its safety and effectiveness.
Source of support
None
Conflict of interest
None
References
- Morgan KA, Adams DB. Management of internal and externalpancreatic fistulas. SurgClin N Am 2007; 87:1503-13.
- Bragg LE, Thompson JS, Burnett DA, Hodgson PE, Rikkers LF.Increased incidence of pancreas-related complications in patientswith postoperative pancreatitis. Am J Surg 1985; 150:694-7.
- Chebli JM, Gaburri PD, de Souza AF, Ornellas AT, MartinsJunior EV, Chebli LA, et al. Internal pancreatic fistulas: proposal of amanagement algorithm based on a case series analysis. J ClinGastroenterol 2004; 38:795-800.
- Alexakis N, Sutton R, Neoptolemos JP. Surgical treatment ofpancreatic fistula. Dig Surg 2004; 21:262-74.
- Cameron JL, Kiefer RS, Anderson WJ, Zuidema GD. Internalpancreatic Fistulas: Pancreatic ascites and pleural effusions. AnnSurg 1976; 184:587-93.
- Bhasin DK, Rana SS, Siyad I, Poddar U, Thapa BR, Sinha SK,et al. Endoscopic transpapillary drainage alone to treat pancreaticascites and pleural effusion. J GastroenterolHepatol 2006; 21:1059-64.
- Pai CG, Suvarna D, Bhat G. Endoscopic treatment as a first linetherapy for pancreatic ascites and pleural effusion. J GastroentrolHepatol 2009; 24:1198-202.
- Kozarek RA, Ball TJ, Patterson DJ, Freeny PC, Ryan JA,Traverso LW. Endoscopic transpapillary therapy for disruptedpancreatic duct and peripancreatic fluid collections. Gastroenterology1991; 100:1362-70.
- Saeed ZA, Ramirez FC, Hepps KS. Endoscopic stent placementfor internal and external pancreatic fistulas. Gastroenterology 1993;105:1213-7.
- Cicek B, Parlak E, Oguz D, Disibeyaz S, Koksal AS, Sahin B.Endoscopic treatment of pancreatic fistulas. SurgEndosc 2006;20:1706-12.
- Seewald S, Brand B, Groth S, Omar S, Mendoza G, Seitz U, etal. Endoscopic sealing of pancreatic fistula by using N-butyl-2-cyanoacrylate. GastrointestEndosc 2004; 59:463-70.
- Fischer A, Benz S, Baier P, Hopt UT. Endoscopic managementof pancreatic fistulas secondary to intraabdominal operation. SurgEndosc 2004; 18:706-8.
- Mutignani M, Tringali A, Khodadadian E, Petruziello L, SpadaC, Spera G, et al. External pancreatic fistulas resistant toconventional endoscopic therapy: Endoscopic closure with N-butyl-2-cyanoacrylate (Glubran 2). Endoscopy 2004; 36:738-42.
- Seewald S, Groth S, Omar S, Imazu H, Seitz U, de Weerth A, etal. Aggressive endoscopic therapy for pancreatic necrosis andpancreatic abscess: a new safe and effective treatment algorithm(videos). GastrointestEndosc 2005; 62:92-100.
- Labori KJ, Trondsen E, Buanes T, Hauge T. Endoscopic sealingof pancreatic fistulas: four case reports and review of the literature.Scand J Gastroenterol 2009; 44:1491-6.
- Brückner M, Grimm H, Nam VC, Soehendra N. Endoscopictreatment of a pancreatic abscess originating from biliarypancreatitis. SurgEndosc 1990; 4:227-9.
- Engler S, Dorlars D, Riemann JF. Endoscopic fibrin gluing of apancreatic duct fistula following acute pancreatitis. Dtsch MedWochenschr 1996; 121:1396-400.
- Sofuni A, Itoi T, Tsuchiya T, Itokawa F, Kurihara T, MoriyasuF, et al. Endoscopic sealing of a pancreatic fistula using ethyl-2-cyanoacrylate. Endoscopy 2006; 38 Suppl 2:E71-2.
- Zuber-Jerger I, Herold T, Kullmann F. Transpapillary sealing ofa pancreatic fistula with Onyx. GastrointestEndosc 2006; 63:1068-9.
- Romano A, Spaggiari M, Masetti M, Sassatelli R, Di BenedettoF, De Ruvo N, et al. A new endoscopic treatment for pancreaticfistula after distal pancreatectomy: case report and review of theliterature. GastrointestEndosc 2008; 68:798-01.
- Trudzinski FC, Rädle J, Treiber G, Kramm T, Sybrecht GW.Massive pleural effusion complicating chronic pancreatitis.Treatment by endoscopic closure of a pancreatic-mediastinal fistula.Dtsch Med Wochenschr 2008; 133:2507-9.




