Keywords
Endocrine Gland Neoplasms; Erythema; Glucagonoma; Pancreatic Neoplasms
Abbreviations
DTPA: diethylenetriaminepentaacetic acid; MOFS: multiorgan failure syndrome; NME: necrolythic migratory erythema; PET: positron emission tomography
INTRODUCTION
First described by Becker et al. in 1942 [1], glucagonoma syndrome is a very infrequent, although well-known, disease. It is characterized by the existence of a glucagonssecreting neoplasm associated with hyperglucagonemia, necrolytic migratory erythema (NME), diabetes mellitus, hypoaminoacidemia, cheilitis, normocytic anemia, vein thrombosis, loss of weight and neuropsychiatric manifestations [2]. The existence of NME used to be considered pathognomonic. Pseudoglucagonoma syndrome refers to the existence of NME in the absence of a neoplasm which secretes glucagon. Slightly more than 300 cases of glucagonoma have been published so far. Its annual incidence has been estimated at 1/20,000,000. It is being described more frequently, and the real prevalence may be greater than estimated [3]. Pseudoglucagonoma syndrome has been described in an even smaller group of patients although data on its real incidence is not conclusive.
MATERIALS AND METHODS
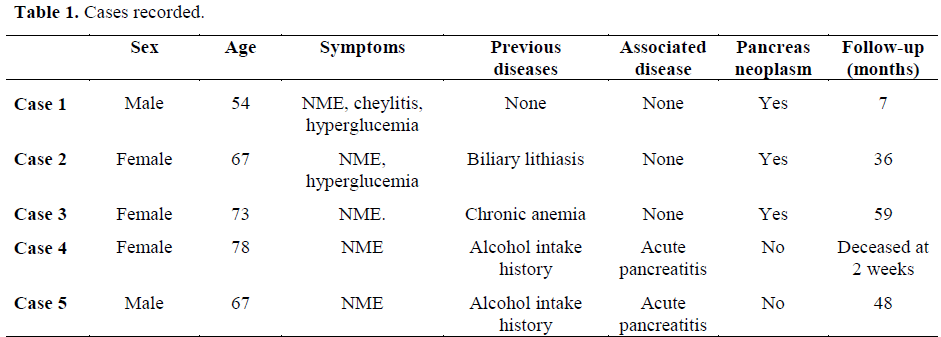
A retrospective review of the cases of glucagonoma and pseudoglucagonoma registered in a sanitary area covering a population of 950,000 persons has been done. From January 1998 to December 2003, 5 cases were treated for glucagonoma syndrome: 3 with a demonstrable pancreatic neoplasm (true glucagonoma syndrome) and 2 cases without a pancreatic neoplasm (pseudoglucagonoma syndrome). We collected the available data on a retrospective basis in each case, including age, sex, first diagnosis and associated symptoms, associated diseases observed, diagnostic procedure, imaging studies, laboratory data, therapeutic procedures employed, surgery and follow-up (Table 1).
ETHICS
No approval by an ethical committee was obtained due to the retrospective nature of the study.
STATISTICS
Frequencies were used as descriptive statistics.
RESULTS
Of the 5 cases studied, 3 were males (60%) and 2 were females (40%). The main clinical manifestation at the moment of diagnosis was the existence of an NME in all of them (Figure 1). Glossitis and cheilitis were observed in 3 cases (Figure 2). In 2 cases, confirmation of NME was done by skin biopsy.
Figure 1. NME: necrolytic migratory erythema. (a. Case 1. b. Case 2. c.: Case 5).
Figure 2. Glossitis. (Case 1).
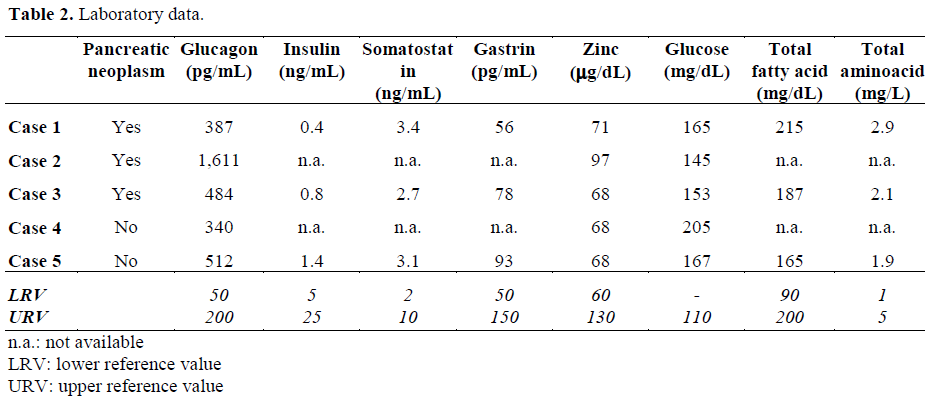
Laboratory data showed an elevation of the plasma glucose in all cases (Table 2). It was more evident in true glucagonoma than in pseudoglucagonoma and was associated with the elevation of plasma glucagon levels. In 3 cases, hypoaminoacidemia was present together with a descrease in free fatty acid levels. No alteration of plasma zinc levels was observed.
Abdominal ultrasound did not offer conclusive results, except in the two cases of pancreatitis, and the CT scan demonstrated a pancreatic neoplasm in 3 cases, situated in the tail, the body/tail, and the body (Figure 3a, 3b, 3c, respectively). An 111I- TPA- (diethylenetriaminepentaacetic acid)-Nterminal D-fenil-alanine octreotide enhanced radio nuclide scan was not done preoperatively.
Figure 3. Computed tomography: glucagonoma in the
pancreas. a. Tail. (Case 3). b. Body and tail. (Case 1). c. Body (Case 2).
The 3 patients presenting with pancreatic neoplasms were operated on and the tumor was resectable in all three cases (Figure 4), through a distal pancreatectomy associated with a splenectomy. No regional disease could be demonstrated on gross and pathology studies (Figure 5). A cutaneous rash cleared up between 7 and 15 days after surgery. The follow-up was 8, 37 and 57 months and the patients are disease-free so far. An 111I-DTPA-N-terminal D-fenil-alanine octreotide enhanced radio nuclide scan was performed postoperatively in two patients without evidence of disease spread.
Figure 4. Operative field: glucagonoma in the pancreas
body. (Case 2).
Figure 5. a. Surgical specimen. b. Pathology (H&E
x200). (Case 2).
The two cases of pseudo-glucagonoma had a history of alcohol dependence and previous episodes of mild acute pancreatitis. One of these patients died from multiorgan failure syndrome (MOFS) as a result of severe acute pancreatitis after two weeks from admission and the other remained free of symptoms 49 months later. This latter patient had a skin rash cleared up by the 10th day, he had not further episodes of pancreatitis, but we have not been able to show tumor growth in successive controls.
DISCUSSION
Glucagonoma syndrome is a paraneoplastic phenomenon characterized by the existence of a glucagons-secreting neoplasm associated with hyperglucagonemia, NME, diabetes mellitus, hypo-aminoacidemia, cheilitis, normocytic anemia, vein thrombosis, loss of weight and neuropsychiatric manifestations [2]. The existence of these symptoms, hyperglycemia and a demonstrable pancreatic neoplasm are useful in establishing a diagnosis [4, 5]. Glucagon is responsible for the clinical picture, and the existence of hypoaminoacidemia, hyperglycemia and lipolisis seem to be responsible for the skin changes, generally described as associated with zinc deficiency and favored by the existence of a previous alteration of the liver function. Patients do not generally present with specific manifestations, such as weight loss, diabetes, diarrhea, and stomatitis [6].
Cutaneous eruption which may go undiagnosed for years before a correct diagnosis is made is not infrequent. NME can be found in any part of the body being most frequently located at the perineum, buttocks, inguinal area, lower abdomen and extremities, namely in areas holding greater pressure and friction. A rash appears and disappears in a 10 day cycle and cure with residual skin hyperpigmentation. Other associated changes may include atrophic glossitis, cheilitis, and inflammation of oral mucosa [7].
Males and females are affected similarly, with the sixth and seventh decades of the life being those of greater frequency of presentation. Although the majority of glucagonomas seem to be sporadic, they can occur in the course of multiple endocrine neoplasm syndromes, and insulin, gastrin, VIP and somatostatin must be evaluated. A glucose tolerance test can help in the delineation of the degree of the alimentary profile in relationship to the secretion of insulin and the functional excess of glucagon. Amino acids, zinc and the essential fatty acids must be evaluated because NME can respond to a correction of its alterations. Nevertheless, high levels of glucagon do not necessarily produce diabetes mellitus, NME [8] or hypoaminoacidemia [9]. Since the liver is responsible for the metabolization of glucagon, cirrhosis can prolong the active period of glucagon expression and contribute to the abnormally high levels in serum. NME with normal levels of glucagon has been described in the sprue and in pancreatitis as well as similar alterations of the skin which can be found in cystic fibrosis [10].
In the presence of NME, the epidermis shows moderate acanthosis, spongiosis, parakeratosis and loss of the granular layer. Dyskeratosis and necrosis in the superficial layers give rise to a characteristic separation of the deepest epidermis [11]. Quick resolutions of NME have been described after surgical resection of a glucagonoma [12] or with a powerful glucagon secretion-inhibiting drug, as happens with somatostatin. Supplements of zinc and the essential fatty acids have been shown to be capable of resolving NME in some patients [13, 14]. The catabolic effects of glucagon at the protein level and fat metabolism are the main factors leading to weight loss, cachexia and anemia [15, 16].
Glucagonomas are slow-growing neoplasms with non-specific symptoms at the beginning. At least 50% of the described cases were metastatic at the moment of the diagnosis and have therefore had a bad outcome. A fiveyear survival rate cannot be estimated because of its rarity, but a study has shown that tumorrelated death occurred in 9 out of 21 patients at an average of 4.9 years after diagnosis, and the remaining 12 patients were alive after an average interval of 3.7 years [17]. The mortality rate associated with the pseudoglucagonoma syndrome is that of the underlying disease. Some cases secondary to celiac sprue are completely cured by diet modification. Others, such as those observed in liver cirrhosis or other neoplasms, generally have a poor prognosis.
Localization of the primary pancreatic neoplasm and spread evaluation is carried out nowadays fundamentally by CT scan, MRI and ultrasound. Positron emission tomography (PET) has recently been employed with positive results [18]. An abdominal angiogram is adequate for locating the primary neoplasm in complex situations because glucagonomas tend to be hypervascularized. The actual identification of the degree of tumor spread is very important because therapeutic interventions may change when metastatic disease exists. Glucagonomas contain somatostatin receptors in more than 80% of cases. Nevertheless, sensitivity and specificity of imaging with somatostatin analogue (111I-DTPA-N-terminal D-fenil-alanine octeotride) has been successfully employed in demonstrating a primary neoplasm and its spread when this exists. It may be utilized as a therapeutic complement due to emission of beta radiation of the marker [19].
These tumors usually present in the tail of the pancreas. They are generally solid, circumscribed and well vascularized [20]. Immunostaining can be positive for glucagon, although the intensity of the dye cannot be correlated with glucagon serum levels. If this method does not detect the production of glucagon, in situ hybridization of mRNA can be conclusive. Electron microscopy may show neurosecretory bodies and a complex endoplasmic reticulum.
Chemotherapy is not effective in the management of glucagonomas probably because the tumor is indolent by nature [21]. Not a single case cured in this way has been recorded [22], but some cases of induced regression and remission of symptomatic NME have been reported. Streptozocin, associated or not with 5-fluorouracil, has offered some response. Dacarbazin has produced remission of NME, reducing levels of titred glucagon. In some patients, octreotide, lanreotide and a long duration analogue of somatostatin have produced rapid clearing of NME, although they have been shown to be ineffective in the pseudoglucagonoma syndrome, where a correct management of the underlying illness often resolves the NME [23, 24, 25].
Surgical resection is the only potentially curative procedure [26]. It is possible when the tumor is still localized. Laparoscopy has recently been employed in a few selected cases [27]. Because tumor growth is slow and tends to be capsulated, resection can be carried out successfully in the early stages [28]. Since NME is the main symptom of the glucagonoma syndrome, palliative therapies can be attempted to diminish skin rash [29]. Tumor mass reduction has been seen to be effective and efficient in healing the cutaneous symptoms [30]; embolization of the liver may also induce selective necrosis of metastasis when present. At present, a liver transplant associated with a pancreatectomy can be considered in the case of rare liver involvement.
References
- Becker SW, Kahn D, Rothman S. Cutaneous manifestations of internal malignant tumors. Arch Dermatol Syphilol 1942; 45:1069-80.
- Buscombe JR, Caplin ME, Hilson AJ. Long-term efficacy of high-activity 111in-pentetreotide therapy in patients with disseminated neuroendocrine tumors. J Nucl Med 2003; 44:1-6. [PMID 12515868]
- Mullans EA, Cohen PR. Iatrogenic migratoty erythema: a case report and review of nonglucagonoma-associated necrolytic migratory erythema. J Am Acad Dermatol 1998; 38:866-73. [PMID 9591806]
- Bonaventure C, Merle P, Grezard P, Ruiz JM, Chevallier M, Scoazec JY, Trepo C. Glucagonoma revealed by necrolytic migratory erythema. Gastroenterol Clin Biol 2003; 27:230-2. [PMID 12658134]
- Koike N, Hatori T, Imaizumi T, Harada N, Fukuda A, Takasaki K, Iwamoto Y. Malignant glucagonoma of the pancreas diagnoses through anemia and diabetes mellitus. J Hepatobiliary Pancreat Surg 2003; 10:101- 5. [PMID 12918465]
- Echenique-Elizondo M, Elorza JL, De Delas JS. Migratory necrolytic erythema and glucagonoma. Surgery 2003; 133:449-50. [PMID 12717367]
- El Rassi Z, Partensky C, Valette PJ, Berger F, Chayvialle JA. Necrolytic migratory erythema, first symptom of a malignant glucagonoma: treatment by long-acting somatostatin and surgical resection. Report of three cases. Eur J Surg Oncol 1998; 24:562-7. [PMID 9870735]
- Davies JP, Billings PJ, Aubrey DA. A glucagonoma without necrolytic migratory erythema. Pancreas 1992; 7:398-400. [PMID 1594565]
- Case CC, Vassilopoulou-Sellin R. Reproduction of features of the glucagonoma syndrome with continuous intravenous glucagon infusion as therapy for tumorinduced hypoglycemia. Endocr Pract 2003; 9:22-5. [PMID 12917088]
- Bencini PL, Vigo GP, Caputo R. Necrolytic migratory erythema without glucagonoma in a heroindependent patient. Dermatology 1994; 189:72-4. [PMID 8003793]
- Huang W, Williams CM, McNeely MC. A persistent periorificial eruption. Necrolytic migratory erythema (NME) (glucagonoma). Arch Dermatol 1997; 133:909-12. [PMID 9236532]
- Smith AP, Doolas A, Staren ED. Rapid resolution of necrolytic migratory erythema after glucagonoma resection. J Surg Oncol 1996; 61:306-9. [PMID 8628004]
- Alexander EK, Robinson M, Staniec M, Dluhy RG. Peripheral amino acid and fatty acid infusion for the treatment of necrolytic migratory erythema in the glucagonoma syndrome. Clin Endocrinol (Oxf) 2002; 57:827-31. [PMID 12460334]
- Sinclair SA, Reynolds NJ. Necrolytic migratory erythema and zinc deficiency. Br J Dermatol 1997; 136:783-5. [PMID 9205519]
- Bernstein M, Jahoor F, Townsend CM Jr, Klein S. Amino acid, glucose, and lipid kinetics after palliative resection in a patient with glucagonoma syndrome. Metabolism 2001; 50:720-2. [PMID 11398151]
- Chastain MA. The glucagonoma syndrome: a review of its features and discussion of new perspectives. Am J Med Sci 2001; 321:306-20. [PMID 11370794]
- Wermers RA, Fatourechi V, Wynne AG, Kvols LK, Lloyd RV. The glucagonoma syndrome. Clinical and pathologic features in 21 patients. Medicine (Baltimore) 1996;75:53-63. [PMID 8606627]
- Fernandez-Represa JA, Fernandez Rodriguez D, Perez Contin MJ, Pena ML, Martinez-Sarmiento J, Carreras JL, Mayol Martinez J. Pancreatic glucagonoma: detection by positron emission tomography. Eur J Surg 2000; 166:175-6. [PMID 10724498]
- Lipp RW, Schnedl WJ, Stauber R, Ranner G, Leb G, Krejs GJ. Scintigraphic long-term follow-up of a patient with metastatic glucagonoma. Am J Gastroenterol 2000; 95:1818-20. [PMID 10925991]
- Johnson SM, Smoller BR, Lamps LW, Horn TD. Necrolytic migratory erythema as the only presenting sign of a glucagonoma. J Am Acad Dermatol 2003; 49:325-8. [PMID 12894090]
- Chu Q, Al-Kasspooles M, Smith J, Nava H, Douglass H, Driscoll D, Gibbs J. Is glucagonoma of the pancreas a curable disease? Int J Gastrointest Cancer 2001; 29:155-62. [PMID 12754386]
- Fjallskog ML, Sundin A, Westlin JE, Oberg K, Janson ET, Eriksson B. Treatment of malignant endocrine pancreatic tumors with a combination of alpha-interferon and somatostatin analogs. Med Oncol 2002; 19:35-42. [PMID 12025889]
- Bouin M, Aoust LD. Clinical response of an atypical glucagonoma treated with a long-acting somatostatin analog. Gastroenterol Clin Biol 2002; 26:926-9. [PMID 12434103]
- Arnold R, Wied M, Behr TH. Somatostatin analogues in the treatment of endocrine tumors of the gastrointestinal tract. Expert Opin Pharmacother 2002; 3:643-56. [PMID 12472080]
- Carvajal C, Azabache V, Lobos P, Ibarra A. Glucagonoma: evolution and treatment. Rev Med Chil 2002; 130:671-6. [PMID 12194691]
- Hellman P, Andersson M, Rastad J, Juhlin C, Karacagil S, Eriksson B, et al. Surgical strategy for large or malignant endocrine pancreatic tumors. World J Surg 2000; 24:1353-60. [PMID 11038206]
- Yada K, Hirano S, Himeno Y, Shibata K, Matsumoto T, Aramaki M, et al. Laparoscopic resection for nonfunctioning small glucagon-producing tumor: report of a case and review of the literature. J Hepatobiliary Pancreat Surg 2003; 10:382-5. [PMID 14598140]
- Matthews BD, Smith TI, Kercher KW, Holder WD Jr, Heniford BT. Surgical experience with functioning pancreatic neuroendocrine tumors. Am Surg 2002; 68:660-5. [PMID 12206598]
- Hellman P, Ladjevardi S, Skogseid B, Akerstrom G, Elvin A. Radiofrequency tissue ablation using cooled tip for liver metastases of endocrine tumors. World J Surg 2002; 26:1052-6. [PMID 12016482]
- Sarmiento,JM, Que FG, Grant CS, Thompson GB, Farnell MB, Nagorney DM. Concurrent resections of pancreatic islet cell cancers with synchronous hepatic metastases: outcomes of an aggressive approach. Surgery 2002; 132:976-82. [PMID 12490844]






