Key words
access to health and social care services,
lesbian, gay, bisexual and transgender people, policy
and legislation
Introduction
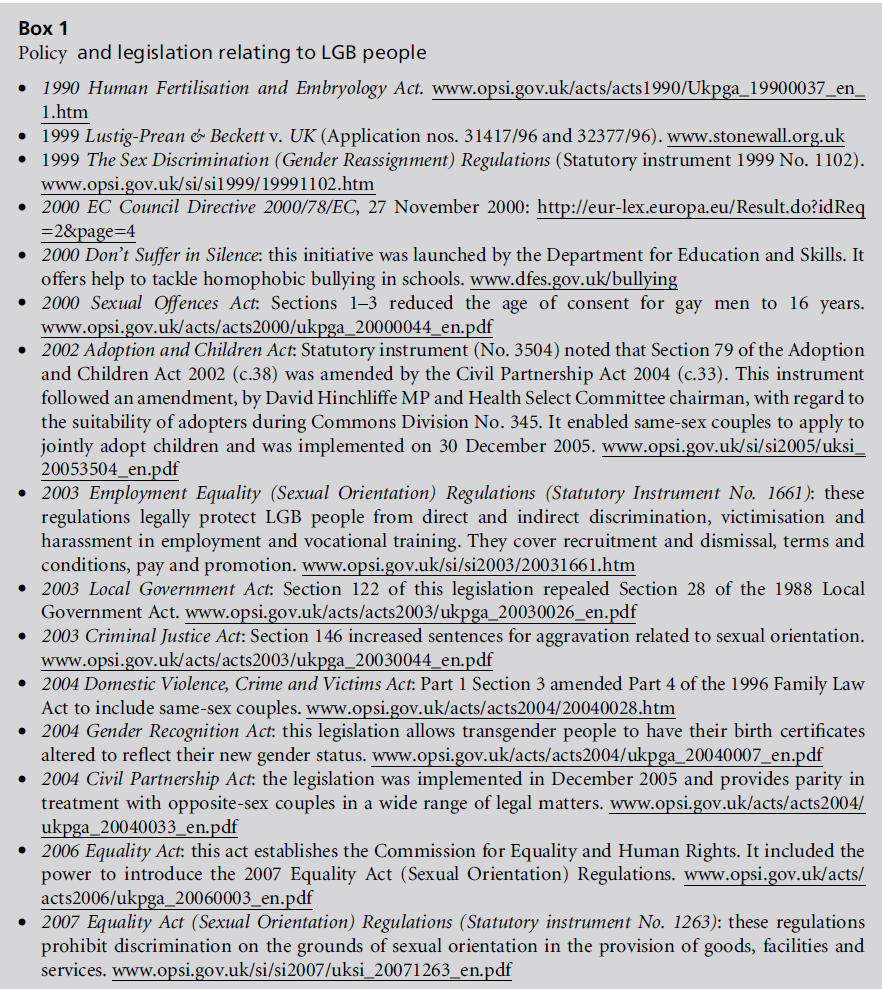
The Equality Act, introduced in England, Scotland
and Wales on 30 April 2007, makes it illegal for
providers of goods, facilities and services, including
health and social care, to discriminate on the grounds
of sexual orientation. The statutory provision for
making these regulations was included in Section 81
of the Equality Act 2006 (see Box1). Discrimination
on the grounds of gender, race and disability has been
prohibited since 1975, 1976 and 1995 respectively; last
year, Part 2 of the Equality Act 2006 extended this
protection to religion and belief. Illustrative examples of sexual orientation discrimination which the legislation
aims to tackle include the denial of health care
to lesbians and the refusal by a hotel to provide a
double room to a gay male couple (Women and
Equality Unit (WEU), 2006). This article first examines
the context, that is to say the background,
legislative transformations and the establishment of
the Commission for Equality and Human Rights, in
which the regulations were introduced. It argues that
recent legislation marks a watershed in lesbian, gay and
bisexual people’s access to services, and it considers the implications of these changes for health and social
care professionals (see Box2). In conclusion, the
article argues that publicly visible lesbian, gay and
bisexual identities may have implications for the
delivery of services and also for conceptions ofwelfare.
Background
Until 1967, homosexuality was illegal in England and
Wales (see Box3). The 1967 Sexual Offences Act
decriminalised gay male activities in private for adults
over the age of 21 years (Weeks, 1979). There were a number of limitations to decriminalisation: the Act
excluded members of the armed forces and merchant
navy. In addition, the age of consent for gay men was
set at 21 years, in comparison to that of 16 years for
heterosexual people. The legislation was thus said to
confer ‘upon homosexuality a ‘‘less than’’ rather than
‘‘equal to’’ status so long as privacy ... [was] preserved’
(Evans, 1990, p.76). Moreover, the act maintained
legal provisions that did not apply to heterosexuality
on the grounds that homosexual behaviour in public
might cause offence to others (Richardson, 1996). The
meaning of privacy was tightly circumscribed: a hotel
room was not private, nor was a house with a third
person in it, if the bedroom door was not locked. Two
decades later, privacy framed political discourses surrounding
the introduction of Section 28 (see below)
and the repeal of the age of consent (Johnson, 2002;
Waites, 2003). The concept of privacy is an important
one because sexual orientation has often been defined
as something which is intimate, personal and private;
by contrast, social policy is concerned with the provision
of public welfare. In thisway, sexual orientation
has been marginalised within social policy as an analytic
category and, until now, has not been ‘considered as
a real concern of welfare’ (Carabine, 1996, p.37 –
emphasis in original) (see Box4). Recent research of
local authority policy supports this suggestion: sexual
orientation was overwhelmingly ranked the lowest of
the sixequa lity strands (Fyfe et al, 2006). Most local
authorities did not refer to sexual orientation in their
strategies or key plans; in strategies where sexual
orientation was included, councils did not monitor
their effectiveness.
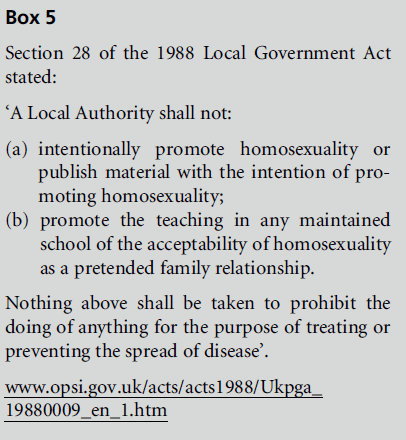
Legislation introduced two decades subsequently
(Section 28 of the 1988 Local Government Act) made
the promotion of homosexuality by local authorities
illegal (see Box5). One writer described Section 28 as a
‘symbolic manifestation of the discrimination against
lesbians and gay men’ (Rahman, 2004, p.151). According
to Carabine and Munro (2004, p.316), ‘Section
28 created a climate of fear and stifled the
development of lesbian and gay work in many local
authorities’. Until 1988, a number of councils had
provided welfare in the form of helplines and other
initiatives, e.g. the London LGB centre in Cowcross Street, financially supported by the Greater London
Council (GLC), was one of the largest in Europe.
Section 28 put many of these services at risk (Evans,
1990; Carabine and Munro, 2004). Furthermore,
because local authorities make grants to local voluntary
sector organisations to deliver welfare, the reach
of Section 28 extended beyond the work of local
councils. For example, the funding body of the
London-based Women’s Health organisation inserted
a clause into the organisation’s contract that ‘prevented’
them from engaging in lesbian health promotion
(James, 1992, p.45).
At the time of Section 28’s introduction, David
Waddington, Home Office Minister, rejected appeals
that discrimination on the grounds of sexual orientation
should be prevented by law, stating that thiswas
a ‘crankish notion’ (quoted in Evans, 1990. p.76).
Such views were held across the political spectrum:
many Labour politicians were also unaware of the
discrimination experienced by LGB people (Carabine,
1995). By contrast, Anya Palmer (of Stonewall – the
UK LGB lobbying organisation) concluded in her
agenda setting for LGB rights campaigning that the
UK had perhaps ‘the most oppressive legislation in
Europe’ (Palmer, 1995, p.49). In comparison, other
European countries introduced an equal age of consent
much earlier than the UK: in 1976 in Denmark
and in 1985 in Belgium. Homosexuality was decriminalised
in Belgium in 1792 (Butt and Maclellan, 2007).
Other legislation curtailed LGBT people’s access to
health and social care services. Section 23 of the 1990
Human Fertilisation and Embryology Act (HFEA)
stated that:
a woman shall not be provided with treatment services
unless account has been taken of the welfare of any child
who may be born as a result of the treatment (including the need of that child for a father), and of any other child
who may be affected by the birth.
Lesbian and single heterosexual women found that
they had limited access to fertility services through the
NHS and some private clinics. Heteronormative assumptions
about what constitutes a family have meant
that lesbians and gay men were not deemed in government
guidance to provide a ‘suitable environment for
the care and nurture of a child’ (cited in Hicks, 2005,
p.45): provisions in the HFEA 1990 Act and guidance
on placing children in foster placements assumed that
the ideal family was provided by a couple composed of
a man and a woman. Heteronormativity constitutes
heterosexuality as ideal and universal: heterosexuality
can thus be said to have been institutionalised in
our social institutions and social practices (Carabine,
2004).
This, then, was the legislative context at the turn
of the 21st century. Concepts of privacy and heteronormativity,
which underpinned the legislation, served
to exclude LGB people from welfare. Moreover, social
and political discourses assumed that LGB people did
not experience discrimination. Because of this context,
many LGB people have been reluctant to disclose
their sexual orientation to professionals and are invisible
users of health and social care services.
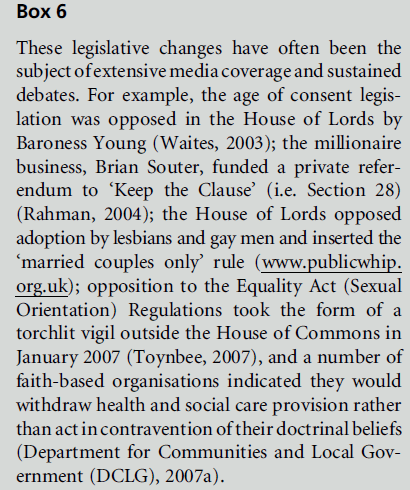
Legislative transformations
The early 21st century has seen a transformation in the
legislative landscape in theUK(see Box6). Following a
Stonewall-led campaign, initiated in the early 1990s to
equalise the age of consent with heterosexual young
people, the 2000 Sexual Offences Act lowered the age
of consent for gay men to 16 years. In respect of the
original legislation, the European Commission of
Human Rights concluded that the UK was in violation
of the European Convention on Human Rights
(Waites, 2003). One of Stonewall’s first and longest
campaigns was to lift the ban on LGB people serving in
the armed forces. Following a 1999 judgement of the
European Court of Human Rights in Lustig-Prean &
Beckett v. UK, the court held that dismissal of a gay
man on the grounds of his sexual orientation constituted
discrimination and contravened Article 8 (respect
for private life) of the European Convention on
Human Rights (for the text of the judgements see www.stonewall.org.uk).
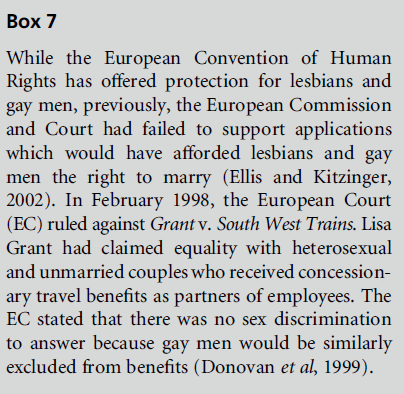
Further pressure for change has come from Europe
(see Box7). Under Article 13 of the 1997 Treaty of
Amsterdam, the European Council (EC) can take
action to combat discrimination based on sexual
orientation. In 2000 the EC issued an Employment
Framework Directive (EC Council Directive 2000) that requires member states to introduce measures
to combat discrimination in employment and training.
This directive was the impetus for bringing sexual
orientation within the scope of employment discrimination
law through the 2003 Employment Equality
(Sexual Orientation) Regulations.
Although there has never been a law that prevented
LGB single people from adopting children, they were
often considered a ‘last resort’ (Hicks, 2005, p.47). An
amendment to the 2002 Adoption and Children Act,
proposed by David Hinchliffe MP, allowed same-sex
couples to apply to adopt jointly for the first time.
Section 122 of the 2003 Local Government Act
(LGA) repealed the prohibition on the promotion of
homosexuality contained within Section 28 of the
1988 LGA.
Section 146 of the 2003 Criminal Justice Act
introduced an increase in sentences for aggravation
relating to sexual orientation. This parallels similar
(so-called) hate crime legislation for ‘race’ and disability;
the latter was also introduced by Section 146
following the bombing of the Admiral Duncan pub in
1999, in which three people died and many more were
seriously injured.
The 2004 Gender Recognition Act (GRA) makes
clear that transgender people must be treated in their
new sexfor all legal purposes including health and
social care. The act allows new birth certificates for
transgender people which recognise their new gender
and the right to marry. The act imposes new responsibilities
to maintain client confidentiality. Section 22 of
the 2004 GRA makes it a crime for any individual who
has obtained information, for example, in health and
social care settings, ‘to divulge that a person has a
gender recognition certificate or do anything that
would make such a disclosure’ (Whittle, 2005, p.39).
The 2004 Civil Partnership Act enables same-sex
couples to gain access to a number of legal rights.
These include pension rights and recognition of next
of kin for hospital visits. The 2004 Domestic Violence,
Crime and Victims Act affords the same legal protection
for victims of domestic violence to same-sex
couples as that extended to heterosexual couples.
Taken together, these (and other) legislative
changes have established the principle that in ‘a
modern and diverse society, it is not acceptable for
someone to be discriminated against because of their
sexual orientation’ (Joint Committee on Human
Rights, 2007, p.10). Sexual orientation has now joined
other equality strands (e.g. ‘race’, gender and disability)
as being a protected ground for different
treatment. The changes are reflective of a social
climate that is more accepting of LGB people, and it
is, therefore, more likely that they will ‘come out’ to
health and social care professionals.
Commission for Equality and
Human Rights
The Equality Act 2006 will implement the most
significant change in equality institutions in 25 years
by establishing a single Commission for Equality and
Human Rights (CEHR) in the autumn of 2007. The
new Commission will replace the three existing
equality institutions: the Equal Opportunities Commission,
the Commission for Racial Equality and the
Disability Rights Commission, and introduce three
new equality strands: age, religion and belief, and
sexual orientation. The stated vision for the single
equality body is to promote a common culture of shared values that underpin citizenship and embed an
ethos of human rights in workplaces, public services
and communities in the UK. The Equalities Review is
the transitional body for the CEHR.
The Equality Act (Sexual
Orientation) Regulations 2007
The regulations establish a clear ‘benchmark for the
sort of fair treatment that everyone should rightfully
expect when accessing services in their everyday lives’
(WEU, 2006, p.8) and provide a ‘legal remedy for
individuals discriminated against on the grounds of
their sexual orientation’ (DCLG, 2007a, p.5). The
regulations, which cover England, Scotland and Wales
(see Box8), prohibit direct discrimination, indirect
discrimination and victimisation on the grounds of a
person’s sexual orientation. Harassment, that is, unwanted
conduct which takes place with the purpose
or effect of violating the dignity of a person and of
creating an intimidating, hostile, degrading, humiliating
or offensive environment, is also deemed to be
discrimination, but has been excluded from the provisions.
The government has deferred a decision upon
this until the outcome of the Discrimination Law
Review (www.womenandequalityunit.gov.uk).
Existing and proposed equalities
legislation
There are similarities and differences in antidiscrimination
legislation between the equality strands.
Protection from discrimination in goods, facilities
and services is afforded to gender, ‘race’, disability,
religion and belief, and sexual orientation, but not age
or transgender. Provisions will be inserted into the
SexDis crimination Act in December 2007 to address
discrimination on grounds of gender reassignment
(Equalities Review, 2007). Protection from discrimination
in employment and training is afforded on the
grounds of gender, ‘race’, disability, religion and belief
and sexual orientation. Protection was afforded to
transgender (by The SexDiscriminati on (Gender
Reassignment) Regulations 1999) and age (by The
Employment Equality (Age) Regulations 2006).
Recent legislation has placed a statutory duty on
public authorities to eliminate discrimination and promote
equality in all aspects of services, and includes
employees and service users. It marks a change in antidiscrimination
legislation because it transfers responsibility
from individuals complaining of unfair treatment
and instead puts a positive duty on organisations
to promote equality on the designated grounds. It is a
proactive approach, supported by enforcement mechanisms
such as race equality schemes, which measures
outcomes. Positive duties have been introduced for
‘race’ (by the Race Relations Amendment Act 2000);
disability (by the Disability Discrimination Act 2005);
and gender (by Statutory Instrument 2006 No 2930),
but not for age, religion and belief, sexual orientation
or transgender. The proposed Single Equality Act is
intended to streamline existing equality legislation.
User perspectives in health and
social care
In a speech marking LGBT history month (www.
dh.gov.uk), Liam Donaldson, the ChiefMedical Officer,
acknowledged the health inequalities experienced by
LGBT communities, and cited UK health and social
care needs assessments which reveal evidence of need
(available from: www.dh.gov.uk/en/Policyandguidance/
Equalityandhumanrights/Sexualorientationandgender
identity/index.htm; see, for example, Spectrum, 2003;
Sanderson and Buckley, 2006; SexualityMatters, 2006).
Recent research suggests that experiences of discrimination
have a negative impact on the health of LGB
people, in terms of lifestyles, mental health and other
health risks. They are more likely to misuse substances,
including cigarettes, alcohol and drugs, making them
vulnerable to unhealthy lifestyles (Fish, 2006).
Gay men and lesbians report increased levels of
psychological distress. Research for the mental health
charity, Mind, has found that they are greater users of
mental health services than heterosexual men and
women (King et al, 2003). Despite this, lesbians, gay
men and bisexual people report mixed experiences
of services: up to 40% of lesbian women recounted
negative or mixed reactions from mental health professionals.
Among young people, homophobic bullying is an
increasing concern (Ellis and High, 2004). In primary
and secondary school playgrounds, the epithet ‘gay’
is a frequent term of abuse (Plummer, 2001) which has
come to mean anything rubbish or second rate.
ChildLine (2006) estimates that 2725 young people
access their services each year to talk about sexual
orientation, homophobia and homophobic bullying;
these issues appear to be of particular concern for boys. Experiences of homophobic bullying mean that
young gay men are much more likely than other young
people to attempt suicide. Young lesbians have an
increased risk of self-harm (Bagley and D’Augelli,
2000). Despite anti-bullying strategies introduced by
the Department for Education and Skills, e.g. Don’t
Suffer in Silence (Department for Education and Skills,
2000), only 6% of schools have policies that specifically
tackle homophobic bullying (Stonewall, 2006).
Recent studies have highlighted the needs of disabled
LGB people (National Disability Authority, 2005;
Abbott and Howarth, 2005). Findings suggest that
health and social care services have made little effort to
take account of their life experiences (Brothers, 2003).
One study of people with learning disabilities found
that, in most instances, they had known from an early
age that they might be LGB but had waited until they
found a member of staff that they felt safe being open
with (Abbott and Howarth, 2005). In comparison to
their heterosexual peers, learning-disabled LGB people
encountered difficulties in meeting other LGB people;
they faced a lack of validation for same-sexrelati onships
and a lack of acknowledgement of LGB people.
Moreover, there are few policies, so that social care
staff do not feel supported to do proactive work
(Abbott and Howarth, 2005).
These studies suggest that health and social care
services do not always take account of LGB people’s
self-esteem and other needs. The new regulations may
contribute towards improving LGB people’s experiences
of health and social care services.
Action in the NHS
The Department of Health is currently working on a
strategy to eliminate discrimination for LGBT people
as both service users and employees in health and
social care. A Sexual Orientation and Gender Identity
Advisory Group (SOGIAG) was established in 2005 to
deliver a programme of activities through four workstreams:
better employment, inclusive services, transgender
and reducing health inequalities. SOGIAG
has commissioned a range of work including a DVD
resource to support health professionals: Real Stories,
Real Lives, LGBTpeop le and the NHS (available, free of
charge, as a download from: www.dh.gov.uk/en/Policy
andguidance/Equalityandhumanrights). In addition
there are briefing papers to support health and social
care professionals in working with LGBT people, core
training standards for health employees on sexual
orientation, and evidence about reducing health inequalities
for LGBpeople (www.dh.gov.uk). In Scotland,
the NHS Inclusion Project (2006) has produced guidelines
to develop knowledge, awareness and attitudes of LGB issues and address the barriers that LGB people
face in their access to health services.
Developments in social care
In the voluntary sector, social care organisations have
been innovative in making social care more accessible
and sensitive to the needs of older LGB people. Age
Concern launched its Opening Doors strategy in 2001,
providing resources and good practice guidance for
home care providers and commissioners of services to
help them to respond to the needs of older LGB people
(Age Concern, 2001; Knocker, 2006). In many ways,
older LGB people share similar concerns to those of
older heterosexual people. But there are also a number
of differences: research suggests that they may be more
likely to live alone, are less likely to have children to
call on, and there is little specialised provision – in the
form of housing, residential care and social groups –
to meet their needs (Heaphy et al, 2003).
Other examples of innovative practice include the
Lesbian and Gay Alzheimer’s Society Carer’s Network
which provides support for lesbian and gay carers. Its
website gives advice on choosing residential accommodation
and examples of good practice in social care
(www.alzheimers.org.uk/Gay_Carers/residentialcare.
htm).
Conclusion
The Department for Communities and Local Government
(DCLG), which is the government department
with responsibility for introducing the regulations,
suggests that LGB people are ‘more likely than heterosexual
people to experience sexual orientation discrimination
in the provision of goods, facilities and services’
(DCLG, 2007a, p.7). Discrimination may occur when
LGB professionals suffer abuse from employers, colleagues,
clients or patients: one report found that
more than two-thirds of LGB health professionals
had experienced problems at work relating to their
sexual orientation (British Medical Association, 2005).
In addition, discrimination may also occur when LGB
patients or service users suffer in the provision of
health and social services. The DCLG expects that the
introduction of the regulations will give LGB people
increased confidence in accessing mainstream services,
have a positive impact on health, and result in
‘an improvement in the level of healthcare’ (DCLG,
2007b, p.9). In order to claim these rights to equal
treatment, Richardson (2000, p.120) argues that LGBT
people will, of necessity, be ‘out’. Over the past three
decades, LGBT politics has been concerned about claims for the right not to have to be private. Publicly
visible LGBT identities may have implications not
only for the delivery of services, but also for conceptions
of welfare. The regulations may begin to pave the
way towards the benefits of full and equal citizenship
for LGB people.
References
- Abbott D and Howarth J (2005) Secret Loves, Hidden Lives: exploring issues for people with learning difficulties who are gay, lesbian or bisexual. Bristol: Policy Press.
- Age Concern (2001) OpeningDoors: workingwith older lesbians and gay men. London: Age Concern England.
- Bagley C and D’Augelli AR (2000) Suicidal behaviour in gay, lesbian, and bisexual youth. BMJ 320:1617–18.
- British Medical Association (2005) Sexual Orientation in the Workplace. www.bma.org.uk (accessed 20 May 2007).
- BrothersM(2003) Not just ramps and braille: disability and sexual orientation. In: Zappone KE (ed) Re-thinking Identity: the challenge of diversity. Dublin: Joint Equality and Human Rights Forum, pp. 49–64.
- Butt R and Maclellan K (2007) The gay globe. The Guardian April 14, pp. 20–21.
- Carabine (1995) Invisible sexualities: sexuality, politics and influencing policymaking. In: Wilson AR (ed) A Simple Matter of Justice? Theorizing lesbian and gay politics. London: Cassell.
- Carabine J (1996) A straight playing field or queering the pitch? Centring sexuality in social policy. Feminist Review 54:31–64.
- Carabine J (ed) (2004) Sexualities: personal lives and social policy. Bristol: Policy Press.
- Carabine J and Monro S (2004) Lesbian and gay politics and participation in New Labour’s Britain. Social Politics 11: 312–27.
- ChildLine (2006) Casenotes: calls to ChildLine about sexual orientation, homophobia and homophobic bullying. www. childline.org.uk (accessed 20 May 2007).
- Department for Communities and Local Government (2007a) The Equality Act (Sexual Orientation) Regulations 2007, Equality Impact Assessment. London: DCLG.
- Department for Communities and Local Government (2007b) The Equality Act (Sexual Orientation) Regulations 2007, Final Regulatory Impact Assessment. London: DCLG.
- Department for Education and Skills (2000) Don’t Suffer in Silence. www.dfes.gov.uk/bullying (accessed 20 May 2007).
- Donovan C, Heaphy B and Weeks J (1999) Citizenship and same sexrelationships. Journal of Social Policy 28:689– 732.
- Ellis SJ and Kitzinger C (2002). Denying equality: an analysis of arguments against lowering the age of consent for sex between men. Journal of Community and Applied Social Psychology 12:167–80.
- Ellis V and High S (2004) Something more to tell you: gay, lesbian or bisexual young people’s experiences of secondary schooling. British Educational Research Journal 30: 213–25.
- Equalities Review (2007) Fairness and Freedom: the final report of the equalities review. https://archive.cabinetoffice. gov.uk/theequalitiesreview/
- Evans DT (1990) Section 28: law, myth and paradox. Critical Social Policy 9:73–95.
- Fish J (2006) Heterosexism in Health and Social Care. Basingstoke: Palgrave.
- Fyfe A, Fleming R and Reid S (2006) Improving Policy and Practice for LGBTPeople: guidance for local authorities. Edinburgh: Scottish Executive. (www.scotland.gov.uk/ socialresearch).
- Heaphy B, Yip A and Thompson D (2003) Lesbian, Gay and Bisexual Lives over 50: a report on the project ‘The Social and Policy Implications of Non-heterosexual Ageing’. Nottingham Trent University: York House Publications.
- Hicks S (2005) Lesbian and gay foster care and adoption: a brief UK history. Adoption and Fostering Journal 29:42– 56.
- James B (1992) Ten years of Women’s Health. Feminist Review, Special Issue on Women’ Health 41:37–51.
- Johnson C (2002) Heteronormative citizenship and the politics of passing. Sexualities 5:317–36.
- Joint Committee on Human Rights (2007) Legislative Scrutiny: sexual orientation regulations, sixth report of Session 2006–7. London: House of Commons.
- King M, McKeown E, Warner J et al (2003) Mental health and quality of life of gay men and lesbians in England and Wales: controlled, cross-sectional study. British Journal of Psychiatry 183:552–8.
- Knocker S (2006) The Whole of Me: meeting the needs of older lesbians, gay men and bisexuals living in care homes and extra care housing. London: Age Concern.
- National Disability Authority (2005) Disability and Sexual Orientation: a discussion paper. www.nda.ie (accessed 20 May 2007).
- NHS Inclusion Project (2006) Fair For All – The Wider Challenge. Good LGBTpractice in the NHS. www. lgbthealthscotland.org.uk (accessed 20 May 2007).
- Palmer A (1995) Lesbian and gay rights campaigning: a report from the coalface. In: Wilson AR (ed) A Simple Matter of Justice? London: Cassell, pp. 32–50.
- Plummer DC (2001) The quest for modern manhood: masculine stereotypes, peer culture and the social significance of homophobia. Journal of Adolescence 24(1): 15–23.
- RahmanM(2004) The shape of equality: discursive deployments during the Section 28 repeal in Scotland. Sexualities 7:150–66.
- Richardson D (1996) Heterosexuality and social theory. In: Richardson D (ed) Theorising Heterosexuality: telling it straight. Buckingham: Open University Press, pp. 1–20.
- Richardson D (2000) Constructing sexual citizenship: theorising sexual rights. Critical Social Policy 62:105–35.
- Sanderson P and Buckley E (2006) Measure for Measure 2: needs assessment of services for lesbian, gay and bisexual individuals in the West Midlands. Birmingham: Gay Men’s Health Network and Staffordshire University.
- Sexuality Matters (2006) Leicester Lesbian, Gay and Bisexual Community Strategy. www.llgbc.com (accessed 20 May 2007).
- Spectrum (2003) Count Me In: health and social care needs assessment of LGBTcommunities in Brighton and Hove. Retrieved 10 November 2003 from www.countmeintoo. co.uk
- Stonewall (2006) Getting Equal: proposals to outlaw sexual orientation discrimination in the provision of goods and services. Response to the Government’s consultation. www. stonewall.org.uk (accessed 20 May 2007).
- Toynbee P (2007) Homophobia, not injustice, is what really fires the faiths. The Guardian 9 January, p. 27.
- Waites M (2003) Equality at last? Homosexuality, heterosexuality and the age of consent in the United Kingdom. Sociology 37:637–55.
- Weeks J (1979) Coming Out: homosexual politics in Britain, from the nineteenth century to the present. London: Quartet Books.
- Whittle S (2005) Born identity. Community Care 24–30 November:38–9.
- Women and Equality Unit (2006) Getting Equal: proposals to outlaw sexual orientation discrimination in the provision of goods and services. London: DTI.

