Keywords
health education, prevention, primary care
Introduction
Primary prevention
includes any intervention designed to reduce the risk of diseases occurring. It
aims to promote wellbeing and to prevent the onset of disease by reducing risk
factors in the population, either through changes in behaviour and lifestyle,
or through changes in the environment supported by appropriate health education
and public policies. Secondary pre-vention targets established disease, with
the aim of avoiding recurrence or alleviating consequences by early detection
and risk factor modification.[1] It is often
not easy to evaluate the effectiveness of preven-tive services,
especially lifestyle counselling, as part of primary prevention. Maciosek et al performed a systematic assessment of the value of
preventive pro-cedures, based on two dimensions: burden of disease prevented by
each procedure and cost-effectiveness.[2]
The most efficient preventive interventions were screen-ing for tobacco
use and alcohol consumption, followed by lipid profile measurement. Counselling
about phys-ical activity and healthy diet were less efficient at reducing
outcomes.
Although prevention may be effective, it is not as widely used as
it should be. The Polish Ministry of Health suggests offering preventive
procedures relat-ing to physical activity, alcohol consumption, tobacco use, diet,
body weight and blood glucose and lipid measurement, to all patients aged 40
years or over, on an annual basis. Lack of time is one of the most cited
barriers towards the delivery of prevention in primary care. A few studies have
examined the actual time physicians spend on preventive services. Yarnall et al estimated that counselling and screening could be
accomplished in 20 to 30 minutes and it would take 7.8 hours per
working day for a physician to deliver recommended preventive services.[3] A discussion around prevention often requires 5 to 10
minutes; an average consultation in primary care lasts 10 minutes.
As a consequence, general practitioners (GPs) have to establish
priorities on which preventive interven-tions to deliver and to whom. We were
interested, especially for patients aged 40 years and over, in which preventive
procedures were offered during routine primary care consultations. Women
are more frequent attendees to primary care than men.[4] Do they receive more prevention procedures, compared
to men? Is there a difference between the categories of preventive
procedures offered to male and female patients?
This study was designed to investigate the effect of patients’
gender on annual delivery of preventive procedures in patients aged 40 years
and over.
The study was performed during a baseline audit in surgeries in 2008 as
a part of the PIUPOZ programme carried out by the Family Medicine Department of
University of Medical Sciences, Poznan, Poland. The acronym PIUPOZ stands for
Poprawa Iakosci Uslug w Podstawowej Opiece Zdrowotnej which means ‘im-proving
quality in primary care’. The aim of the PIUPOZ is to improve the quality of
primary care in Poland by offering training in preventive medicine for
GPs. In the PIUPOZ programme, lectures and inter-active workshops were
undertaken with groups of 15 people, lasting 25 hours during two weekends. The
main topics were prevention, diagnosis and treatment of coronary heart disease
(CHD) and chronic obstruc-tive pulmonary disease (COPD), and breast and colon
cancer screening. Participation, accommodation and course materials were
provided free of charge. After completing the course, participants received a
certifi-cate and educational credits. Data presented in this paper were
collected prior to participation of phys-icians in the programme.
Method
The study
population consisted of all GPs working in the Wielkopolska region recruited to
the PIUPOZ programme. Doctors working or training in family medicine or those
in internal medicine working in primary care settings were included as GPs
invited to take part in the project. Invitations were sent by mail and email.
Recruitment to the programme was ex-tended through personal contacts, at
medical confer-ences or with the aid of adverts in the medical press.
Candidates were registered through the family medi-cine department until the
sample size of 120 GPs was achieved. Of the120 doctors who volunteered to
partici-pate, 113 were included in the present study; seven were excluded
because of subsequent withdrawal.
Observers (two men and two women) were recruited from final-year
medical students with an interest in family medicine. They received a four-hour
training session on preventive guidelines from a member of the research team.
They were also instructed about the study registration form and how to perform
an audit regarding confidentiality rules. The observers were exclusively
involved in collecting data in the offices (surgeries) of participating
GPs. They monitored GPs during consultations and observed each GP for
pre-ventive procedures undertaken with four consecutive patients aged 40 years
and over. The observers had access to patients’ medical records and recorded,
in addition to the observed preventive procedures dur-ing the consultation, all
preventive procedures noted in the patient’s medical record during the previous
year.
The recording form used by the observers collected information on 11
preventive procedures: screening for tobacco use, alcohol consumption, body
weight, body mass index (BMI), waist measurement, physical activity, diet (fat
or fruits and vegetables intake), blood pressure, blood glucose and lipid
profile. For each procedure, the observer recorded whether it was per-formed
(or not) during the observed consultation or recorded in the previous year. The
physician identity was not recorded on the study form and the observed doctors
did not have access to the forms.
Statistical
analysis
Descriptive
statistics were used to characterise the observed patients. The analysis
focused on delivery rates of different
preventive procedures and the differ-ences between female and male
patients. Chi-square tests were used to compare quantitative data. All tests
were analysed at the significance level of 0.05, and analyses were performed
using STATISTICA v.7.1 (StatSoft Inc, www.statsoft.com).
Results
Study sample
A total of 450
patient consultations and medical records (from 113 GPs) were collected and
analysed. For each patient only one consultation was registered. There were 267
(59.3%) women and 183 (40.7%) men observed. The GPs had a similar mixed patient
popu-lation of men and women. The proportion of men and women on the patient
lists of the doctors was com-parable. All study patients were aged 40 years or
over; the mean age was 59.5 (standard deviation (SD) = 11.23): 60.2 years (SD =
11.25) for women and 58.6 years for men (SD = 11.14); P =
0.13.
Preventive
procedures
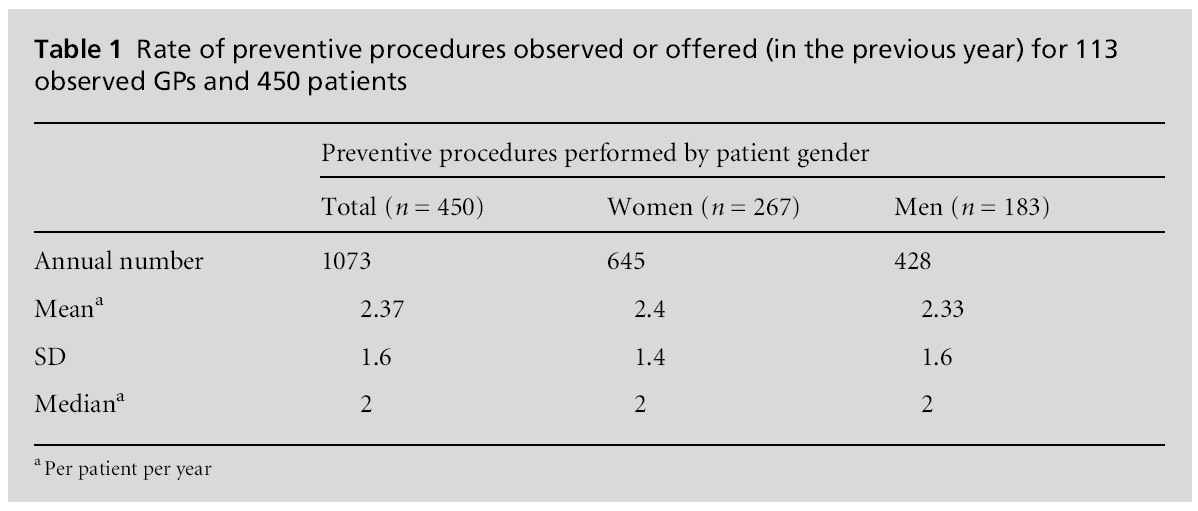
During the
observed consultations, 1073 preventive procedures were performed, 645 (60.1%)
in women and 428 (39.9%) in men. This difference was not statistically
significant. The mean number of pro-cedures per patient was 2.37 (SD = 1.6):
2.4 (SD = 1.4) for women and 2.33 (SD = 1.6) for men. The numbers of procedures
performed in women and men are presented in Table 1 and the rates of specific
preventive procedures are presented in Table 2. The most frequently recorded
procedures were serum glucose in 68.0% of the patients, blood pressure in 58.4%
and total cholesterol measurement in 55.6% of the patients. In 81 (18%)
patients who received only one preventive procedure at the observed
consultation or during the previous year, 35.8% had serum glucose measured and
34.6% had blood pressure checked. A high number of preventive procedures (six
out of 11) were offered to less than 10% of patients: dietary, tobacco
use and alcohol drinking screening, exercise counselling, BMI and waist
measurement.

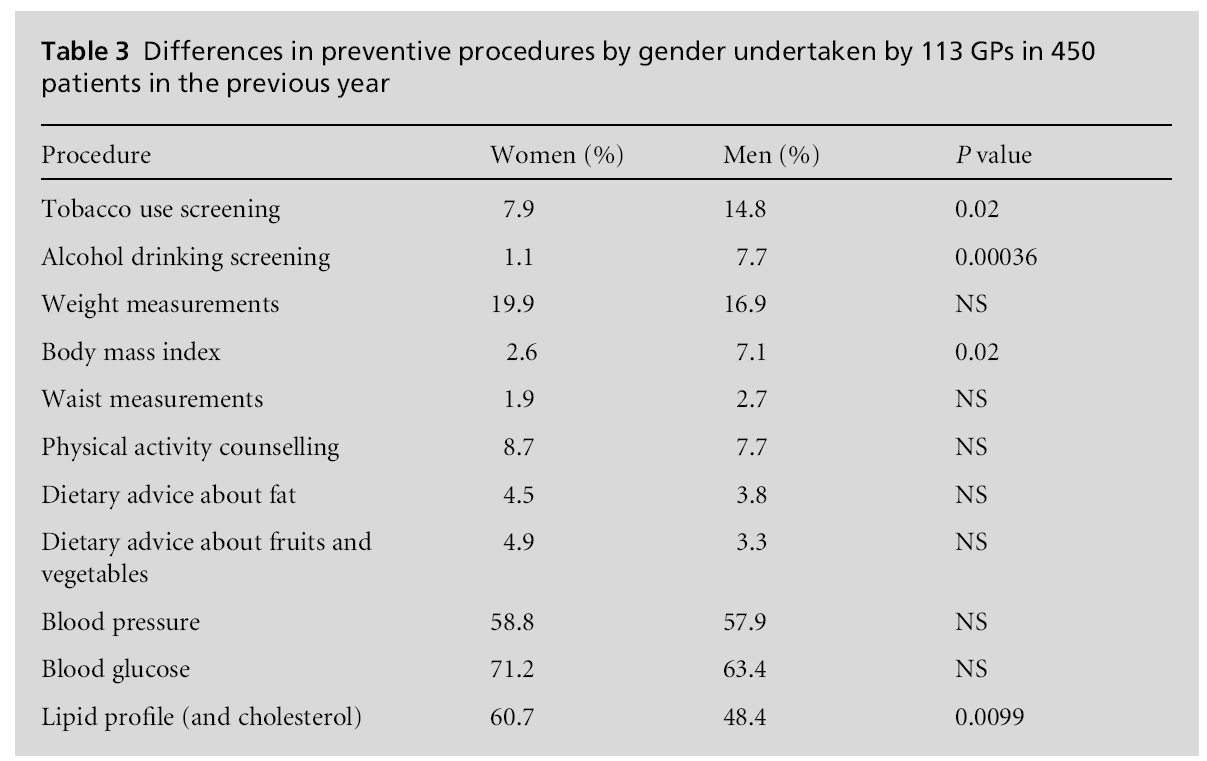
The correlation between gender and the delivery of preventive
procedures is presented in Table 3. There was a statistically significant difference
between patients’ gender and some preventive procedures. Men were more likely
to receive screening for tobacco use, alcohol consumption, and BMI measurement,
whereas women had their blood cholesterol checked more frequently.
Discussion
During the
observed consultations, screening for alcohol consumption, tobacco use and BMI
was more fre-quently offered to men than to women, while women were more
likely to have a laboratory test for choles-terol.
The overall delivery of preventive procedures (2.4 per patient per
year) in primary care fell below the levels recommended by the Polish Ministry
of Health for people aged 40 years in the target group to have the listed
preventive procedures each year. The finding of a low rate of preventive
interventions in primary care is consistent with previous studies in other
European countries.[5] The need to improve prevention is of
par-ticular interest to primary care. According to American, European,
Australian and World Health Organization (WHO) guidelines, preventive
activities such as tobacco use screening, alcohol screening, weight
measurement, BMI, waist circumference, blood pressure, diet and physical
activity counselling should be offered to all adult patients.[6–9] Lipid profile and blood glucose should be checked in
older patients, but cut-off points are different in different
countries. According to Polish guidelines they should be checked annually in
patients aged 40 years and older. Women or men should be offered
prevention in the same way.
In our study, five primary prevention procedures represented 13% of all
reported interventions, and together with blood pressure measurements, lipid
profile and blood
glucose comprised 76.3% of all procedures. According to the literature, the
secondary–tertiary prevention model leads to primary prevention being
undervalued.[10] It is a challenge for educational
pro-grammes to target GPs to focus on the real priorities in prevention efforts
for adults aged 40 years and over.
Gender differences
Although women
are more frequent attendees than men in primary care, this is not always
reflected in their receiving more preventive interventions.[11,12] Some studies show that women receive less prevention,
whereas others conclude the opposite. Most investi-gators agree that women
receive less lifestyle advice.[4,13] Compared
with men, more women had their total serum cholesterol measured. For
laboratory-based procedures, not only is a physician’s action involved but so
also is a patient’s co-operation. If doctors offer these tests with-out
patients’ agreement, they will not be performed. The difference between
clinically based preventive pro-cedures and lifestyle advice may be partly
explained by the doctor–patients interaction. Brotons et al,
in a study among GPs in 11 European countries, observed that more than half of
GPs were sceptical of helping patients to reduce tobacco use, decrease alcohol
con-sumption, achieve or maintain normal weight, and practise regular physical
exercise.[14] It is unusual for patients to ask for
lifestyle advice as a specific reason for a consultation, but many will ask
doctors for laboratory tests. Many GPs experience pressure from patients who
demand unnecessary tests or medical treatment. According to van Steenkiste et al, patients often perceive cholesterol as a very
important risk factor, even more important than smoking.[15] Women are often more concerned about their health and
may insist on their GP performing laboratory tests to prevent disease or to
maintain their healthy state.[13]
Tobacco
use screening
It is widely
accepted that brief advice against smoking can be effective. For every 50
smokers who receive advice to stop from their GP, one or two will do so.[16] Anti-smoking advice is one of the three most highly
ranked preventive interventions.[2] According to
Aus-tralian guidelines, smoking status should be checked annually in all
patients older than 12 years of age.[8]
In our study only 11% of patients were asked about smoking in the previous
year. According to the literature, GPs use few opportunities for discussing
smoking with patients, advising only a minority of those who consult.[17] In our study, a higher proportion of men received
anti-smoking advice, but GPs need to be aware that the number of women smoking
is increasing. In Poland, 33.9% of adult men and 19.3% of women are current
smokers.[4] As a consequence, the incidence of lung
cancer in women is also increasing. Research suggests that patients can become
irritated by GPs’ questions about tobacco use.[17]
The anticipation of patients’ irritation may explain why GPs are more likely to
discuss smoking with patients who have smoking-related problems.[18]
A concern about patient irritation may also explain other missed opportunities
for health promotion by GPs. Counselling about obesity is not well received by
patients.[19] Obese persons and those who are
over-weight are often self-conscious about their weight,[20] which may explain why doctors are not keen to discuss
body weight, waist circumference, BMI or dietary advice. It is estimated that
in Poland, despite 27% of women and 33% of men being obese, BMI is not
frequently measured. In our study it accounted for only 1.9 % of the performed
preventive procedures (see Table 2). Discussing obesity, in particular with
female patients, may be very difficult and lead to GPs avoiding such
uncomfortable situations by simply not discussing them.
Alcohol screening
GPs’ desire for
harmonious relationships with patients also appears to influence the way they
discuss alcohol drinking with patients. In general, only 3.8% of the observed
patients were asked about alcohol consump-tion, and the gender difference
is remarkable: 1.1% of the women, compared to 7.7% of the men (P = 0.0004). Although Poland
belongs to countries with a large average alcohol consumption and men drink on
average 4.5 times more than women, the rate of annual alcohol screening in
primary care is five times less than that in the UK.[4,21] It is clear that educational programmes for GPs to
ameliorate preventive counselling needs to pay attention to discussion of
alcohol consumption, espe-cially in female patients.
Strengths
and limitations of the study
There are
several weaknesses in our study. The study sample of doctors was not randomly
selected, but based on active recruitment of interested volunteers for a
training programme. Recruited physicians may have been more motivated than the
average doctor to incorporate prevention in their consultations. The real
preventive performance of the average GP in Poland may therefore be lower than
that in the current study.
Reported rates of delivered procedures may have been influenced by the
presence of an observer. We assumed that doctors performed and offered
preventive procedures unaffected by the observer. The recording of
preventive procedures in the medical records may vary between physicians, but
when a particular inter-vention was observed we assumed that this was effect-ively
performed. We believe that direct observation in combination with inspection of
the patient record gave fairly reliable estimates of the preventive activities
of GPs with any particular patient.
Although we performed our study in one region, many of the factors
identified are not unique to Poland and are probably seen in different
primary care set-tings in Europe.
In this study we did not explore the effect of doctors’ gender on
the delivery of preventive procedures be-cause participating physicians were
anonymous. This will be studied during the second phase of the PIUPOZ
programme. In the literature, there is evidence that doctors’ gender may affect
their performance in pre-vention activities. Bertakis and Rahman found that
female physicians were slightly more likely to check patients’ blood pressure,
but no significant differences were seen in other non-gender-specific
prevention procedures.[22] According to Frank and Harvey, female
physicians were reported to undertake systematic patient counselling more often
than male physicians.[23]
A strength of the present study was the direct observation of doctors’
preventive behaviour by trained observers. Many previous estimates of the
delivery of preventive procedures are based on doctors’ self-assessment or on
patients’ medical records, particu-larly electronic records. In Poland,
electronic patient records are not common. Direct observation of the doctor and
inspection of the patient record was the most appropriate
way to study doctors’ behaviour in real life. The healthcare system in Poland
is organised by registering patients in a specific primary care setting.
Patients cannot follow their personal preference for a particular doctor, which
means that every GP has a variety of patients of different ages and
gender and limits the possibility of a gender bias whereby female patients
register preferentially with female doctors, or male patients with male
doctors.
Conclusion
This study is
based on direct observation of doctors’ behaviour in combination with the
patient record and demonstrated that the annual delivery of preventive
interventions in primary care fell below recommended levels. Limited time and
resources encourage GPs to perform certain preventive procedures in preference
to others. In particular, preventive procedures based on clinical examinations
and laboratory tests were performed more often than lifestyle advice.
Education and lifestyle counselling need doctors’ personal engagement
and specific communication skills. Preventive guidelines should take into
account that patients’ gender and personal attitude to health advice may
influence GPs’ performance in preventive pro-cedures. Men are more likely to
receive preventive procedures such as tobacco screening, drinking screen-ing
and BMI measurement.
Changing beliefs and attitudes of GPs about giving lifestyle advice
during routine consultations remains a challenge. Effort made to
introduce lifestyle advice and education into the consultation may bring about
long-term health benefits and it is planned to encourage this change in
doctors’ behaviour through interactive work-shops as part of the PIUPOZ
programme.
Funding
The study was
supported by a grant from Iceland, Lichtenstein and Norway through the EEA
Financial Mechanism.
Ethical Approval
The PIUPOZ
programme was approved by the Bioethics Committee of the Poznan University of
Medical Sciences, Poland. Informed patient consent was obtained from all patients. All
patient/personal identifiers were removed or disguised so the patient/
person(s) described are not identifiable and cannot be identified thorough the
details of the story.
Peer Review
Not
commissioned; externally peer reviewed.
Conflicts of Interest
None.
References
- Stokes J, Noren J and
Shindell S. Definition of terms and concepts applicable to clinical preventive
medicine.Journal of Community Health 1982;8:33–41.
- Maciosek
MV, Coffield AB, Edwards NM and Flottemesch TJ. Priorities among effective
clinical pre-ventive services results of a systematic review and analy-sis. American Journal of Preventive Medicine 2006;31:52– 61.
- Yarnall
KS, Pollak KI, Ostbye T, Krause KM and Michener JL. Primary care: is there
enough time for prevention? American Journal of Public Health 2003;93: 635–41.
- Central Statistical Office.
Use of healthcare and con-sumption of medicines. In: State of Health of Polish Citizens in 2004. www.stat.gov.pl/cps/rde/xbcr/gus/PUBL_stan_ zdrowia_2004.pdf (accessed 7 September 2009).
- Steptoe A, Doherty S,
Kendrick T, Rink E and Hilton S. Attitudes to cardiovascular health promotion
among GPs and practice nurses. Family Practice 1999;16:158– 63.
- The World Health
Organization. Prevention of
Cardio-vascular Disease.
Geneva: World Health Organization, 2007.
- American Academy of
Family Physicians. Summary of Recommendations for Clinical Preventive Services. Re-vision 6.4, 2007. https://www.aafp.org/exam
(accessed 7 September 2009).
- The Royal Australian
College of General Practitioners ‘Red Book’ Taskforce. Guidelines for Preventive Activities in General Practice (7e).
Melbourne: The Royal Australian
College of General
Practitioners, 2009. www.racgp.org.au/Content/NavigationMenu/ClinicalResources/RACGP
Guidelines/TheRedBook/redbook_7th_edition_May_ 2009.pdf (accessed 7 September 2009).
- Graham I, Atar D,
Borch-Johnsen K et al. European guidelines on cardiovascular
disease prevention in clini-cal practice. European Journal of Cardiovascular Preven-tion and
Rehabilitation 2007;14(suppl
2):S1–S113.
- Mirand AL, Beehler GP,
Kuo CL and Mahoney MC. Explaining the de-prioritization of primary prevention:
physicians’ perceptions of their role in the delivery of primary care. BMC Public Health 2003;3:15.
- Goodwin MA, Zyzanski
SJ, Stange KC and Mendalie JH. Gender differences in time spent during
direct obser-vation of doctor–patient encounters. Journal of Women’s Health
2004;13:341–9.
- Barnhart J, Lewis V,
Hounghton JL and Charney P. Physician knowledge levels and barriers to coronary
risk prevention in women. Journal
of Women’s Health 2007;
17:93–100.
- Ashenden R, Silagy C
and Weller D. A systematic review of the effectiveness of promoting
lifestyle change in general practice. Family Practice 1997;14:160–76.
- Brotons C, Bjo¨rkelund
C, Bulc M et al. Prevention and health promotion in
clinical practice: the views of general practitioners in Europe. Preventive Medicine
2005;40:595–601.
- van Steenkiste B, van
der Weijden T, Timmermans D et
al. Patients’ ideas, fears and
expectations of their coronary risk: barriers for primary
prevention. Patient Education and Counseling 2004;55:301–7.
- Coleman T and Wilson A.
Anti-smoking advice from general practitioners: is a population-based approach
to advice giving feasible? British
Journal of General Practice 2000,50:1001–4.
- Young JM and Ward JE.
Influence of physician and patient gender on provision of smoking cessation
advice in general practice. Tobacco Control 1998;7:360–3.
- Coleman T, Murphy E and
Cheater F. Factors influ-encing discussion of smoking between general
prac-titioners and patients who smoke: a qualitative study. British Journal of General
Practice 2000;50:207–10.
- Sussman AL, Williams
RL, Leverence R, Gloyd Jr and Crabtree BF. The art and complexity of primary
care clinicians’ preventive counselling decisions: obesity as a case study. Annals of Family Medicine 2006;4:327–33.
- Harting J, van Assem P,
van der Molen HT, Ambergen T and de Vries NK. Quality assessment of health
counselling: performance of health advisors in
cardiovascular pre-vention. Patient Education and Counseling
2006;61:142– 51.
- McCormick KA, Cochran NE, Back AL et al.
How primary care providers talk to patients about alcohol. Journal of General Internal
Medicine 2006;21:966–72.
- Bertakis KD and Rahman
A. Patient gender and phys-ician practice style. Journal of Women’s Health
2007; 16:859–68.
- Frank E and Harvey L.
Prevention advice rates of women and men physicians. Archives of Family Medicine 1996;
5:215–19.

