Keywords
Carcinoid Tumor; everolimus; lanreotide; Neuroendocrine Tumors; Octreotide; pasireotide; Somatostatin
Abbreviations
ELECT: doublE-bLind, randomizEd placebo controlled Clinical Trial; mTOR: mammalian target of rapamycin; NET: neuroendocrine tumor; RADIANT: RAD001 in Advanced Neuroendocrine Tumors
INTRODUCTION
Gastroenteropancreatic neuroendocrine tumors (NETs) can range in biological behavior and metastatic potential. As described previously in our discussion detailing the 2013 ASCO Annual Meeting, treatment depends on the qualitative and quantitative assessment of the tumor, taking into account a qualitative and quantitative assessment of the patient [1]. Resection of localized disease can prove curative, especially when dealing with a less aggressive subtype of NET. However, in the setting of locally advanced or metastatic disease with aggressive histological features, systemic modalities involving cytotoxic and hormonally targeted agents become indispensable options for treatment.
Cytotoxic chemotherapy has been well established in the treatment of both locally advanced and metastatic gastroenteropancreatic NET. Mechanisms of action stem from alkylation of DNA, platinum crosslinking of DNA, and the incorporation of pyrimidine analogs to interrupt DNA synthesis.
Molecularly targeted agents have been used with varying degrees of success in the treatment of gastroenteropancreatic NET. Among these agents, tyrosine kinases, mammalian target of rapamycin (mTOR), and vascular endothelial growth factor receptors (VEGFR) have shown the greatest potential; however, studies continue to report variable degrees of activity against subsets of NET.
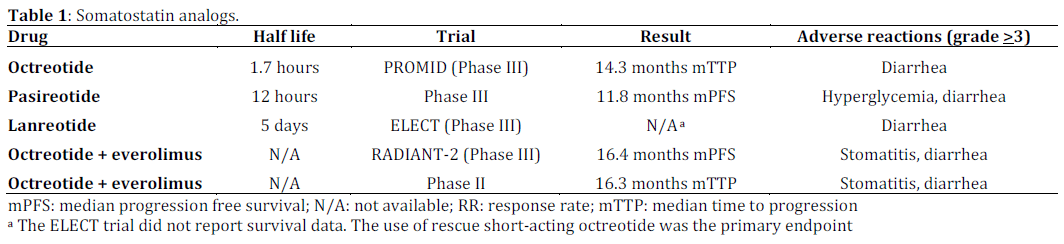
Given the scope of our discussion, we will focus our attention on highlighting our current understanding of somatostatin analogs, their use in gastroenteropancreatic NET, previous trials of these agents, and what the 2014 Gastrointestinal Cancers Symposium has brought to light in this exciting field. Table 1 summarizes the current breakdown of somatostatin analogs.
What We Knew Before the 2014 ASCO Gastroenterology Cancers Symposium
Somatostatin analogs have been shown to be efficacious in the treatment of gastroenteropancreatic NET. As demonstrated by Rubin et al., somatostatin analogs can be used to control symptoms associated with carcinoid syndrome [2]. Short and long acting octreotide remains the most widely used somatostatin analog. Acting as an analog to endogenous somatostatin, octreotide works to competitively inhibit somatostatin receptors, with a decrease in the secretion of vasoactive substances from NETs. In 2009, the PROMID (Placebo controlled, double-blind, prospective, Randomized study on the effect of octreotide LAR in the control of tumor growth in patients with metastatic neuroendocrine MIDgut tumors) trial demonstrated that the use of octreotide improved median time to progression to 14.3 months compared to 6 months in the placebo arm [3]. In 2013, follow up data assessing overall survival in the PROMID trial, found that patients in the octreotide arm had an increase in overall survival compared to the placebo arm; however, those patients with a low hepatic tumor burden seemed to benefit the most [4].
Pasireotide has also been assessed in the setting of gastroenteropancreatic NET. Pasireotide has a higher affinity for somatostatin, thus having a longer half life. However, compared to octreotide, pasireotide induces higher rates of hyperglycemia. The benefit of pasireotide was demonstrated by Wolin et al. in a randomized, blinded phase III trial assessing the efficacy of pasireotide versus octreotide. It was shown that symptom control was comparable between the two groups; however, the pasireotide group showed an improved (11.8 months) progression free survival compared to the octreotide (6.8 months) group (P=0.045) [5].
The inhibition of the mTOR pathway in gastroenteropancreatic NET has been evaluated in previous studies as a viable option in controlling gastroenteropancreatic NET. The RAD001 in Advanced Neuroendocrine Tumors (RADIANT-3) trial helped establish that everolimus can be used as monotherapy in pancreatic NET [6]. The randomized, phase III RADIANT-2 trial showed a pronounced benefit when everolimus and octreotide were compared to placebo and octreotide [7]. In fact, median progression free survival was among the highest (16.4 months) compared to trials looking at single agent somatostatin analogs. In 2013, an Italian group headed by Bajetta et al., presented data from a phase II trial that further corroborates that the addition of everolimus to octreotide therapy benefits progression free survival (16.3 months) in the first line setting when treating advanced gastroenteropancreatic NET [8].
What We Have Learned at the 2014 ASCO Gastrointestinal Cancers Symposium
The 2014 Gastrointestinal Cancers Symposium featured two noteworthy abstracts which detailed the efficacy of a novel somatostatin analog, lanreotide. Both abstracts are unique, in that the authors used symptom management as a primary aim in these studies. The long half life of lanreotide is also worth considering, as this may shift our understanding of how we treat gastroenteropancreatic NET. Additionally, lanreotide has already been approved in Europe for the treatment of gastroenteropancreatic NET; however, the U.S.A. has yet to follow suit.
ELECT: A Phase III Trial of Lanreotide (Abstract #268 [9])
The ELECT (doublE-bLind, randomizEd placebo controlled Clinical Trial) trial, as reported by Vinik et al., is a phase III study comparing lanreotide depot injections versus placebo in the setting of histologically confirmed gastroenteropancreatic NET, with those patients demonstrating carcinoid syndrome. The trial had two phases, with an equivalent distribution of 115 participants within each study arm. The first phase involved administration of the study drug in a randomized, double blind design. The second phase was an open label design. The primary end point was control of symptoms related to carcinoid syndrome. The study demonstrated a 15% absolute reduction in the use of short acting rescue somatostatin analogs for symptom control, favoring lanreotide (P=0.02). Additionally, a lower frequency and duration of use of short acting somatostatin analogs was seen with lanreotide (OR=2.4; 95% CI: 1.1-5.3; P=0.04). Patient tolerability of lanreotide appeared acceptable versus placebo [9].
SYMNET: An Observational Trial of Symptom Control with Lanreotide (Abstract #273 [10])
As an international, cross-sectional, nonintervention trial, the SYMNET study group assessed the use of lanreotide depot injections in 273 patients. The primary aim of the study was to assess patient satisfaction with symptom control related to carcinoid syndrome in gastroenteropancreatic NET. Parameters of satisfaction were measured in periodic patient surveys and documented by providers over the course of each patient’s treatment. Overall, a significant percentage of patients reported high levels of satisfaction with control of diarrhea (76%), flushing (73%), and improvement in daily activities (75%) [10].
Discussion
The field of gastrointestinal oncology continues to grow, and with it have come advances in the treatment of gastroenteropancreatic neuroendocrine tumors. These advances have looked at novel ways of targeting the neuroendocrine neoplasms. The use of hormonally active somatostatin analogs has become the mainstay of therapy in the way we approach this heterogeneous group of cancers.
Octreotide continues to exemplify the prototypical agent that has established the groundwork for the use of somatostatin analogs in NET. However, as noted above, our options continue to expand with the introduction of pasireotide and lanreotide. Both agents share the propensity as a longer acting alternative to octreotide. The 2014 Gastrointestinal Cancers Symposium offered us a closer look at lanreotide and the data looked encouraging. However, the ELECT and SYMNET trials did not prove efficacy over octreotide or pasireotide. The limitations of these studies are based in their design and merely show an improvement in symptom control without the prevention of progressive disease. As noted in Table 1, the survival advantage of octreotide and pasireotide has been demonstrated in multiple trials, in addition to an overall improvement in symptom control. Furthermore, the addition of everolimus to octreotide has demonstrated a stark increase in survival parameters, suggesting that the addition of molecularly targeted agents to somatostatin analogs should be considered as viable options for these patients.
As the field continues to advance, it is possible that we may see octreotide being used as a short acting rescue medication with the aforementioned newer somatostatin analogs taking more of an upfront role in the setting of both controlling symptoms of carcinoid syndrome and treating advanced NET. However, before we see a paradigm shift in the treatment of NET, we need studies that truly show an improvement in survival parameters.
Conflicts of interest
The authors have no potential conflicts of interest
References
- Khagi, S, Saif MW. Neuroendocrine Tumors: Treatment Updates. JOP. 2013 Jul 10;14(4):367-71 PMID 23846929
- Rubin J, Ajani J, Schirmer W, Venook AP, Bukowski R, Pommier R, Saltz L, Dandona P, Anthony L. Octreotide acetate long-acting formulation versus open-label subcutaneous octreotide acetate in malignant carcinoid syndrome. J Clin Oncol. 1999;17(2):600 PMID 10080605
- Rinke A, Müller HH, Schade-Brittinger C, Klose KJ, Barth P, Wied M, Mayer C, Aminossadati B, Pape UF, Bläker M, Harder J, Arnold C, Gress T, Arnold R, PROMID Study Group. Placebo-controlled, double-blind, prospective, randomized study on the effect of octreotide LAR in the control of tumor growth in patients with metastatic neuroendocrine midgut tumors: a report from the PROMID Study Group. J Clin Oncol. 2009;27(28):4656 PMID 19704057
- R. Arnold, M. Wittenberg, A. Rinke, C. Schade-Brittinger, B. Aminossadati, E. Ronicke, T. M. Gress, H. H. Mueller, PROMID Study Group. Placebo controlled, double blind, prospective, randomized study on the effect of octreotide LAR in the control of tumor growth in patients with metastatic neuroendocrine midgut tumors (PROMID): Results on long-term survival. ASCO 2013 Abstract No: # 4030
- E. M. Wolin, B. Jarzab, B. Eriksson, T. Walter, C. Toumpanakis, M. Morse, P. Tomassetti, M. Weber, D. R. Fogelman, J. Ramage, D. Poon, J. M. Huang, M. Hudson, X. Zhi, J. L. Pasieka, A. Mahamat, F. Swahn, J. Newell-Price, W. Mansoor, K. E. Oberg. A multicenter, randomized, blinded, phase III study of pasireotide LAR versus octreotide LAR in patients with metastatic neuroendocrine tumors (NET) with disease-related symptoms inadequately controlled by somatostatin analogs. ASCO 2013 Abstract No: # 4031
- Yao JC, Shah MH, Ito T, Bohas CL, Wolin EM, Van Cutsem E, Hobday TJ, Okusaka T, Capdevila J, de Vries EG, Tomassetti P, Pavel ME, Hoosen S, Haas T, Lincy J, Lebwohl D,Öberg. RAD001 in Advanced Neuroendocrine Tumors, Third Trial (RADIANT-3) Study Group. Everolimus for advanced pancreatic neuroendocrine tumors. N Engl J Med. 2011;364(6):514 PMID 21306238
- Pavel ME, Hainsworth JD, Baudin E, Peeters M, Hörsch D, Winkler RE, Klimovsky J, Lebwohl D, Jehl V, Wolin EM, Oberg K, Van Cutsem E, Yao JC, RADIANT-2 Study Group. Everolimus plus octreotide long-acting repeatable for the treatment of advanced neuroendocrine tumours associated with carcinoid syndrome (RADIANT-2): a randomised, placebo-controlled, phase 3 study. Lancet. 2011;378(9808):2005 PMID 22119496
- E. Bajetta, L. Catena, N. Fazio, S. Pusceddu, P. Biondani, G. Blanco, S. Ricci, M. Aieta, F. Pucci, M. Valente, N. Bianco, F. Bellomo, C. Mauri, P. Buonandi, V. Roberto. Everolimus in combination with octreotide LAR as the first-line treatment for advanced neuroendocrine tumors: A phase II trial of the I.T.M.O. (Italian Trials in Medical Oncology) group. ASCO 2013 Abstract No: #4136
- A. Vinik, E. M. Wolin, H. Audry, E. L. Gomez-Panzani. ELECT: A Phase 3 study of efficacy and safety of lanreotide autogel/depot (LAN) treatment for carcinoid syndrome in patients with neuroendocrine tumors (NETs). 2014 GI Cancers Symposium Abstract No: #268
- P.B. Ruszniewski, M. Caplin, J.W. Valle, C.L. Bohas, P. Maisonobe, P. Atlan. Patient-reported satisfaction with symptom control during lanreotide autogel/depot (LAN) treatment for carcinoid syndrome (CS) in gastroenteropancreatic neuroendocrine tumor (GEP-NET) patients: Symnet, a large multinational, cross-sectional, observational study. 2014 GI Cancers Symposium Abstract No: #273

