Key words
ethnicity, focus groups, qualitative research,
reproduction, women’s health
Introduction
Endometriosis is a chronic, disabling condition, and a
common cause of chronic pelvic pain. Estimates of its
incidence range between 5% and 15% of the adult
female population (Damewood et al, 1997; Ballard et al,
2006). It is usually characterised by pelvic and abdominal
pain, lower back pain, and deep dyspareunia (pain
on deep penetration during sexual intercourse); other
symptoms, such as urinary and bowel dysfunction, may
be present in some women. The symptoms usually
fluctuate in a cyclical manner, but the pain can be
constant. However, a woman who is diagnosed as
having ‘mild’ disease by diagnostic categorisation may
experience severe symptoms, while a woman who has
extensive disease may be asymptomatic, and is only
diagnosed opportunistically (e.g. during investigations
for infertility). Endometriosis is associated with up to
40% of attendance at fertility clinics (Lessey, 2000).
Although there are many medical and surgical interventions
for endometriosis, there is no definitive cure.
There is growing evidence in the research literature
about the experience of living with endometriosis.
Within this body of work, a picture of many years of
pain is consistently catalogued, along with difficulties
and delay in getting a diagnosis and treatment, negative
effects on work, social relationships and family
life, and poor experiences in the healthcare system
(Cox et al, 2003; Whelan, 2003, 2007; Denny, 2004a;
Jones et al, 2004; Huntington and Gilmour, 2005).
These studies contain descriptions of many problems
for women with endometriosis, some of which derive
from the enigmatic nature of the condition and the
highly gendered ‘delegitimation’ of women’s accounts
by the medical profession (Whelan, 2007). However,
such important studies are largely confined to women
from majority white communities. Little is known
about the incidence of endometriosis by ethnicity, or
of the specific experiences or needs of minority groups
(Cramer and Missmer, 2002; Kyama et al, 2004).
In this articlewe report the first phase of a UK-based
study (the Endocul Project) which used focus groups
to explore community awareness of endometriosis
and experiences of living with endometriosis in a sample
of women from a range of minority ethnic communities
(Indian, Pakistani, African Caribbean, Chinese
and Greek/Greek Cypriot). Within the study, which
was funded by the UK National Institute for Health
Research, we also explored the experiences of women
with endometriosis from these five minority ethnic
groups (phase 2), and the attitudes and information
needs of healthcare providers (phase 3). A paper
addressing the second phase of the study and the
overall outcomes is in preparation.
Background
Endometriosis is a condition characterised by a largely
hidden stigma (Goffman, 1963), which affects intimate
aspects of female bodies. The majority of women
experience the worst of their symptoms around the
time of menstruation, and many find that these are
treated as dysmenorrhoea, which tends to be viewed
by medical practitioners and others as a ‘normal’ part
of the menstrual cycle (Denny, 2009). This normalisation
is described as a ‘narrative of endurance’
(Markovic et al, 2008), both in the interpretation of
pain by women and in their acceptance of the often
dismissive response of medical practitioners. Doctors
will frequently undermine patients’ accounts of their
illness, and therefore their credibility, by portraying
them as nervous and irrational women who exaggerate
their symptoms (Whelan, 2007). The experience of
endometriosis is thus gendered, both physiologically
and culturally, and concepts surrounding it are bound
up with other gendered and culturally variable concepts
such as womanhood, menstruation and reproduction.
There are no robust published data on ethnic differences
in the prevalence ofendometriosis (Shaw et al,
2003), or data on how women with endometriosis, who
are members of minority ethnic communities, experience
healthcare. We know from many other studies
that healthcare systems in many societies do not always
respond appropriately to the needs of minority groups,
and that minority ethnic patients in developed societies
generally evaluate care more negatively than white
majority patients (Aspinall and Jacobson, 2004; Bhopal,
2007; Mead and Roland, 2009).
The experience of both illness and healthcare is
multifaceted. Illness behaviour and themedical response
to this are clearly mediated by ethnic and cultural
difference (Denny, 2009). The experience of endometriosis
for all women is bound up with cultural representations
of menstruation. Although ideas relating
to menstruation are historically and culturally specific,
most societies have some taboos or rituals concerned
with the menstruating woman. In her research among
men in the UK, Laws (1990) uses the term ‘etiquette of
menstruation’ to describe the expected behaviour of
women during this time. Interestingly, it is cultures
other than the dominant white cultures that have most
frequently been studied in terms of menstrual taboos.
This, Laws argues, demonstrates complacency about
how menstruation is dealt with in the UK, and by
extension in other developed, post-industrial countries.
It also reflects a culturalist approach to ethnic
inequalities whereby only minority ethnic communities
are seen as having ‘culture.’ Laws argues that the
meaning of menstruation is bound up with ideas that it is something that must be hidden, and derives more
strongly from the social rules surrounding it than
from its biological nature. The ‘etiquette of menstruation’
is often associated with negative connotations,
including feelings of shame, embarrassment, and the
need for concealment. Britton (1996) found that, from
an early age, women learned negative images of menstruation,
associated with bleeding and pain. Yet
women are also told that menstruation is a normal
and natural event, something that marks one as a
mature woman who is capable of reproduction. Seear
(2009) argues that the stigmatisation of menstruating
women as discreditable is associated with concealment
and a consequent reluctance to disclose the symptoms
of endometriosis. Even when women identify that
their experience is not normal, obstacles such as
criticism and the trivialising of pain by family, employers
and others deter them from seeking professional
help.
The idea of ‘menstruation as pollution’ is common
in many cultures, and influences practices and taboos.
For example, Helman (2007, p. 47) talks about cultural
conceptions of the ‘polluting power’ of menstrual
blood, which is believed to cause weakness in
males, and of the perception of menstruating women
as having a contagious pollution by South African
Zulu peoples: ‘Crops may be ruined or cattle fall ill if
she walks among them’ (Helman, 2007, p. 48). He
further argues that the menstruating woman can also
be viewed as ‘vulnerable’, and that customs and taboos
are designed to symbolically protect women while also
shielding men from the polluting power of menstrual
blood. However, Laws (1990) warns against the conflation
of these types of taboo and the rules of etiquette,
which may be quite minor cultural markers of menstruation,
and emphasises diversity of cultural practice.
It has to be remembered that, for many societies
and for much of history, menstruation was a rare
occurrence for women, who were either pregnant,
breastfeeding or malnourished for many of their
reproductive years, and therefore it may also have
been viewed as something out of the ordinary.
Cultural ideas of reproduction and motherhood
can also influence how women experience endometriosis,
because it is implicated in infertility. Helman
(2007) states that, in societies where the desire for high
rates of childbearing is low and where contraception is
easily available, sex gradually becomes divorced from
fertility, and practices that do not lead to pregnancy
are more widely tolerated. Conversely, if large families
are highly desirable, then sex and fertility are conceptually
intertwined, and sex outside marriage is not
tolerated. Whether or not sex is seen as purely for the
purpose of procreation, most contemporary societies
are pronatalist (Letherby, 1999). They display attitudes
and policies that are pro-motherhood and encourage
reproduction at least in some sections of the population (Culley and Hudson, 2009). Infertility, whether voluntary
or not, is considered deviant or abnormal, and
childlesswomen are seen as not realwomen (Letherby,
1999; Culley and Hudson 2009). Those women for
whom being childless has traditionally been socially
sanctioned, such as widows, nuns and nannies, have
been defined by loss, self-sacrifice or the nurturing of
other people’s children, thereby bolstering pronatalist
cultural discourse (Gillespie, 2003).
Although expectations about childbearing for normative
adulthood are dominant in most societies, the
intensity of such attitudes and the impact on women
and men is culturally diverse. A range of studies of
cultural differences in the experience of infertility within
low-resource and developed countries (van Balen and
Inhorn, 2002; Culley et al, 2006) have demonstrated
the often devastating consequences for the social and
psychological well-being of women in particular. In
their study of infertility in South Asian communities
in the UK, Culley and Hudson (2006) found a very
intense pronatalist ideology, withmarriage being almost
universal and infertility being highly stigmatised.
Study design
The sensitive nature of the topic and the need to
sensitise the research team to the views of the communities
in the study meant that a qualitative design
was deemed appropriate for this study (Green and
Thorogood, 2004; Atkin and Chattoo, 2006). A multiphased
approach was adopted in order to obtain the
views and experience of a range of stakeholders whose
attitudes and behaviours may influence the experience
of endometriosis (Whelan, 2007).
Phase 1 of the Endocul Project focused on healthy
women, who were each invited to take part in one
focus group with other members of the minority group
to which they belonged (see Table 1). The aim was to
gain insight into community views, values and practices
regarding reproductive issues such as womanhood,
reproduction and sexuality which gave a cultural
context for the experience of endometriosis among
women from minority ethnic groups.
Focus groups can serve a useful function by setting
data in context during the exploratory phase of a
project (Culley et al, 2007). They can also allow participants
to bring to the fore issues of significance to
them (Bryman, 2008), and offer a reflexive framework
for the nature of attitudes and the construction of issues
(Waterton and Wynne, 1999).
Although the term ‘focus group’ may be used to
describe any form of group interview (Wilkinson, 1999;
Green and Thorogood, 2004), there are various types
of grouping, and those involved in this study may
more accurately be described as ‘natural groups’, since a number of the women who participated came from
the same geographical location, and some of them
already knew each other. This was particularly appropriate
in order to maximise interactions between the
participants, and in providing access to a shared culture.
In researching sensitive issues such as sexuality
and reproduction, a natural group with similar people
may encourage more openness than other types of
interview situation, and solidarity stemming from
shared problems may encourage more free expression
of opinions (Wilkinson, 1999). The researchers in this
study were particularly interested in how the participants
discussed the issues raised as members of a social
group, rather than as individuals. The goal was to elicit
community perspectives rather than personal views.
Thus, as well as showing solidarity, individuals could
challenge or refute the views of another as not reflective
of the culture (Bryman, 2008).
Table 1: Details of focus group participants
Ethical approval
Ethical approval for the study was obtained from
North Staffordshire Local Research Ethics Committee
in March 2008.
Method
Community facilitators were recruited from the target
minority ethnic communities to conduct the focus
groups. Their role was to organise, facilitate and transcribe
focus group discussions that took place with
members of their community group, and to verify the translated participant information sheets. Most of
them were experienced in conducting focus groups,
and all of them attended a one-day training event
designed to familiarise them with the aims of the
project and to provide background information on
endometriosis. They also played an important role in
discussing a draft of the focus group guide drawn up
by the research team, and were able to input suggestions
relevant to the cultural context of their own
communities. In discussing this guide the team of
facilitators were able to develop some conceptual consistency
of the instrument across the different culture
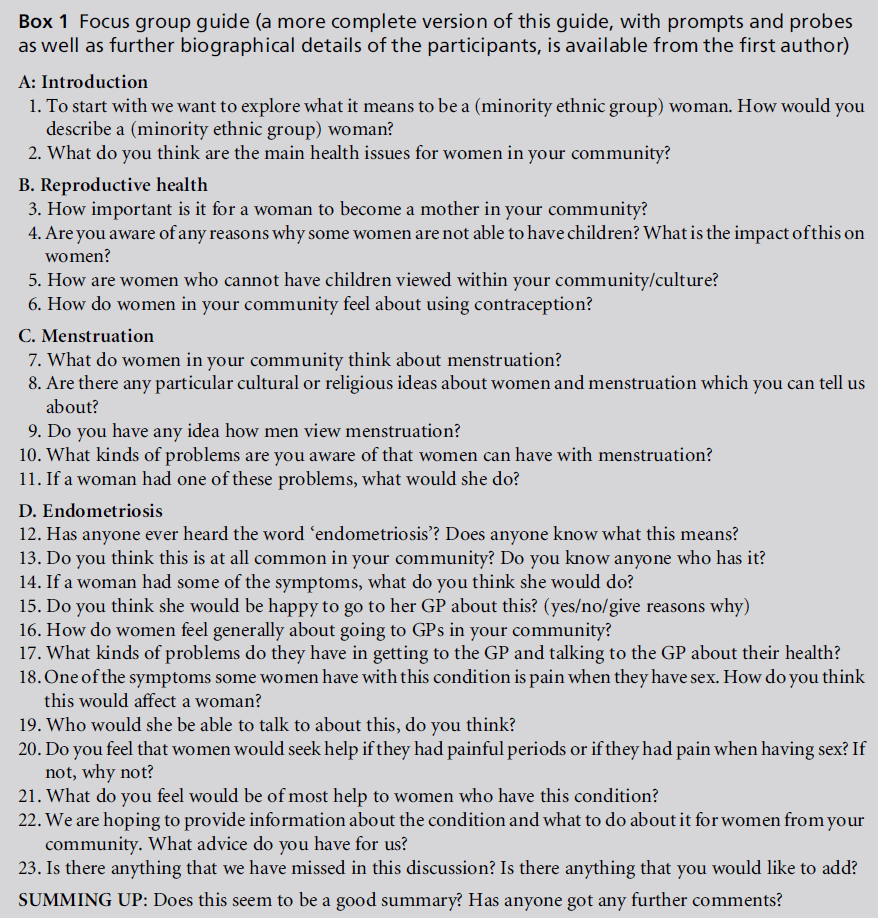
and languages (Culley et al, 2007). As endometriosis is
a gendered condition that can potentially affect fertility,
the focus group guide included issues for discussion
about gender and ethnic identity, menstruation,
and reproductive health, as well as endometriosis (see
Box 1).
The rationale for using community facilitators was
both to ensure cultural competence and to enable the
project to benefit from the advantages of the ‘insider’
researcher (Culley et al, 2007; Gunaratnam, 2009).
They were all well placed to use their knowledge of
their owncultures in a constructive and reflexive manner
prior to, during and after fieldwork, and could also
conduct the focus groups in the target group’s language
if necessary. It was important that the main
issues raised during discussions were interpreted with
relevance, as meanings are often lost in the literal
translation of terms (Mehta, 2005).
Women were recruited to the focus groups by the
community facilitators and through contacts of the
research team. The only criterion for selection was a willingness to discuss issues relating to reproductive
health with other women from their community. Four
of the five focus groups were co-facilitated by the same
member of the research team (PA), while the focus
group with members of the Greek/Greek Cypriot
community was co-facilitated by a different member
of the team, who is a Greek Cypriot (IP). This ensured
a consistent approach, thus increasing reliability (Kidd
and Parshall, 2000). The researcher and facilitator set
ground rules for the conduct of the groups, in terms of
keeping the discussion confidential and respecting the
views of other members. The Indian, Pakistani and
Greek/Greek Cypriot focus groups were conducted in
English, with some references being made in the Gujarati, Urdu or Greek languages. The Chinese focus
group was conducted solely by the community facilitator
in Chinese. The researcher had no understanding
of the language, and merely sat through the discussion,
although they noted non-verbal cues. This is
consistent with the findings of Chiu and Knight (1999),
who observed an effect on group dynamics when
discussion was interrupted by translations. The focus
group discussions lasted between 54 minutes and 2
hours.
Participants in the focus groups were each given a
£20 high-street store gift token in appreciation of their
giving time to a research project with no immediate
benefit to themselves.
Analysis
Each focus group discussion was transcribed verbatim,
and, in the case of the Chinese discussion,
translation was carried out by the community facilitator,
and verified by one of the Chinese focus group
members (Mehta, 2005). All members of the research
team familiarised themselves with the transcripts and
identified initial themes. The team then discussed
these at length and reached a consensus on key themes.
Verification occurred through discussion about the
analyses, comparison and subsequent consensus (Braun
and Clarke, 2006). The community facilitators also
had an input into this analysis by commenting on and
validating the themes identified and providing additional
insight into the context, thus enhancing the
dependability of the research process (Culley et al,
2007).
One member of the team then performed an indepth
analysis drawing on the information generated
from the preliminary analysis, which was guided by
framework analysis (Ritchie and Spencer, 1994), which
categorises data analysis into five key stages, namely
familiarisation, identifying a thematic framework, indexing,
charting, and mapping and interpretation. The
team member who had been present at all but one of
the focus groups verified the transcripts, which added
to the credibility of the study. She was involved in the
preliminary analysis, and had therefore internalised
the data. A framework was developed from the themes
previously agreed by the research team. Indexing,
charting and coding were aided by qualitative software
(NVivo version 8). The data were coded in accordance
with the thematic framework, again using NVivo
version 8. The final stage of framework analysis, namely
mapping and interpretation, was undertaken by sorting
the data by theme, identifying patterns in the data and
piecing these together to form a story. This stage was
further refined as each member of the team fed in their
interpretation of various quotes, and during discussion
at team meetings.
Findings
The data are presented here using the key themes
identified by the analytical process, whichwere ‘ethnic
and gender identity’, ‘menstruation’, ‘reproduction’
and ‘endometriosis.’
Ethnic and gender identity
There were marked differences in the ways in which
groups perceived gender and ethnic identity, but all
agreed that traditional identities were being increasingly influenced by younger women living (and in some
instances educated) in the UK.
The African Caribbean group described women
in their community as leaders, in the forefront of
community life. They felt themselves to be empowered
and independent. All of them were in paid work and
were the main breadwinners for their families.
‘I think we have high status. I think especially nowadays
men realise our worth and the balance has moved from
men being the providers to women. Most black women
tend to earn more than black men.’
(African Caribbean woman)
The Chinese women (C) viewed living in the UK as
different fromliving in China.Whereas in China most
women work outside the home, in the UK they faced
language difficulties, expensive childcare and other
problems in getting suitable jobs. Many women within
this community were unemployed and stayed at home,
or worked in a family business. There was also a
perceived lack of integration into theUK, and a stronger
identity with the Chinese community than with gender.
The Greek/Greek Cypriot focus group included a
wide age range. Members of the group perceived
Greek women as being in the process of breaking
out of the traditional female Greek/Greek Cypriot
mould. They were more liberal and had more choice
than the traditional Greek/Greek Cypriot woman,
whowas viewed as being subservient to men. This group
perceived themselves as strong and able to multi-task
while maintaining their responsibilities for their home
and children as they moved to new roles. The generational
differences between Greek women were summed
up by a young woman who was born in the UK, as she
spoke of older Greek women:
‘They were quite powerless really. Also they worried about
what other people thought, you know your house had to
be clean if anybody came round, whereas now women are
out a lot of hours working, whereas mymumwas at home
looking after the children. It was very different.’
(Greek Cypriot woman)
According to the Indian group, children in their
community were brought up to respect the family
and in-laws. Being a Gujarati woman meant having
close family ties and respecting the older generation.
Gujarati women in the UK saw themselves as more
liberal and open than their counterparts living in
India. They related more to their children. The children
born in the UK were exposed to other cultures
and tended to question Gujarati ways, and parents
therefore needed to be able to deal with this. The
Gujaratiwomen felt that it was important to keep their
culture alive within their children.
The Pakistani women described women in their
community mainly as housewives. However, as the following three extracts demonstrate, the younger
generation were educated in the UK and were engaging
in paid work.
‘Women manage the home and organise the family, which
is seen as their main role, but although they view it as an
important one, they are generally not given the credit for
this.’
(Pakistani woman)
‘I think personally the women are most important because
they do everything and they make a lot of decisions,
they do most of the housework, run around the children,
they basically do everything. But in some families they’re
not seen as dominating.’
(Pakistani woman)
‘They’re not appreciated either.’
(Pakistani woman)
In summary, the traditional role of the woman as
mother and homemaker was evident in all of the
groups, but there were differences in the way that
this was played out, particularly with regard to the
amount of power and control that women felt they
had, with the African Caribbean women viewing themselves
as having most control, and the Pakistani
women least. Acculturation within a dominant British
culture was increasingly influencing gender and ethnic
identities, particularly for those women who had been
born and/or educated in the UK, and all of the groups
recognised that there were generational differences
within their community. For example, in contrast to
the older women, younger Greek/Greek Cypriot women
did not expect to do paid work as well as all of the work
in the home.
Menstruation
The experience of menstruation was viewed negatively
by all of the groups. Women used terms such as ‘curse’
by either the Devil or God, and spoke of embarrassment
about buying sanitary towels or about the private
and personal nature of menstruation. The Indian,
African Caribbean and Greek/Greek Cypriot groups
also mentioned that menstruation was regarded as
unclean, and yet, as the following exchange from the
latter group demonstrates, women were often unclear
why such views persisted.
G/GC1: ‘I don’t know, what is the thing about having a
period and being dirty?’
G/GC2: ‘Well, I thought that it originated from the fact
that when women used to be on their periods many, many
years ago, and there wasn’t proper sanitary towels.’
G/GC3: ‘Yes, that’s what my yiayia [grandmother] says.’
G/GC2: ‘And it could be disastrous. But nowadays I don’t
know why it’s carried on.’
G/GC4: ‘Yes, but I’ve heard that is a myth, because a
cousin of mine who is quite religious asked a church elder,
he’s one of the monks who go to Mount Athos, and he
said, it’s better you go to church and kiss the icons if that’s
what you feel to do rather than not kiss them.’
Paradoxically, some women simultaneously viewed
menstruation positively as a cleansing process. Menstruation
was also seen as a marker of not being
pregnant, which could be positive or negative, depending
on the wishes of the woman at that point in time.
All of the groups spoke of religious or cultural
taboos relating to menstruating women, based on
the idea of the menstruating woman as unclean, or
as potentially causing harm to others. For example, it
was reported that Rastafarian men will not eat with
their wives while they are menstruating, and the Indian
women spoke of not being allowed into the kitchen at
that time.
I7: ‘ I do know of a friend here who this is happening to ...
she lives with her mother-in-law and she is not allowed
into the kitchen.’
I2: ‘I was not allowed into the kitchen ... no. I was not
allowed to even cook. I know this also happens in India.’
I3: ‘It is considered ‘‘dirty’’, and that is why we are not
allowed into the kitchen ... but why? It is natural ... yes.’
[all in agreement]
Not being allowed into places of worship was also
mentioned by the Indian, Pakistani and Chinese groups,
but most of the women reported knowing about these
restrictions rather than experiencing them. Pakistani
women reported that they were not allowed to read the
Quran or pray during menstruation, and this was the
only group which stated that sexual intercourse was
forbidden at this time. The fact that these restrictions
seem to be widespread across different religious traditions
is consistent with the assertion of Laws (1990)
that most societies emphasise menstruation in some
way. There is also some evidence that these restrictions
are not imposed by women themselves as protection
during a time of vulnerability, but rather that they are
imposed by a sexual hierarchy intended to demonstrate
the inferiority of women (Laws, 1990).
Women were also asked about the experience of
menstrual pain, and how this was dealt with within
their community.
‘Women in our community would treat it as a normal
period pain and dismiss it.’
(Pakistani woman)
‘If it’s just period pain I think they would think that it is
normal.’
(Chinese woman)
Women from the African Caribbean and Chinese
groups mentioned traditional remedies that might be
used for menstrual pain, but within these groups there
was some disagreement as to whether these were
effective, or whether Western medicine was preferable.
Some African Caribbean women mentioned white
rum containing ganja, and the Chinese women spoke
of dietary therapy, mainly soups such as brown sugar
and ginger.
‘It [the brown sugar and ginger soup] helps [the body
drive] the cold Qi out of body. Because coldness in uterus,
and the cold cannot get out, then causes period pain.’
(Chinese woman)
The Chinese group also spoke of people having traditional
remedies sent from China, but commented
that Chinese medicine was expensive compared with
western drugs.
The other three groups talked about taking analgesia,
and consulting with family members and friends.
The Indian women thought that women in their
community would talk to a friend rather than a family
member, and that this person being of a similar age
was important. Discussion of personal topics between
the age groups was difficult, and the group thought
that older women would be inhibited. One of the
Indian group members spoke of how the closeness of
the community made it hard for women to discuss
what are seen as personal issues.
‘For example, if my in-laws know or are related to my
doctor I would not be physically able to say look this is my
problem because they would know. Even though I would
hope the doctor would not tell them in my mind I would
know that what if they find out.’
(Indian woman)
The women in the Pakistani group felt embarrassed to
talk to a doctor, but felt that they could talk to family
members or a friend.
‘We know lots of girls that just wouldn’t go to the doctor’s
and talk about a problem, because it’s so embarrassing,
especially if it’s a male doctor. ‘‘I can’t tell a bloke about
this’’, and hope the pain will go away.’
(Pakistani woman)
The African Caribbean women felt that painful periods
were a very personal, private affair and not open for
discussion. Some members of the group disliked what
they described as their white British colleagues openly
discussing menstruation.
The Greek women were the only ones who felt that,
within their community, issues relating to menstruation
could be discussed openly, not only with other
female family members and friends, but also with
men.
All of the focus groups demonstrated that Laws’
idea of a menstrual etiquette is quite widespread
among many ethnic groups, but the way in which
this is played out varies. The feeling that menstruation
is polluted or dirty is common, but it is also clear that
although these beliefs are perpetuated, there is no clear
indication of their origin. They are generally accepted
as part of a specific religion. Secrecy about menstruation
was a feature of all the groups except the Greek/
Greek Cypriot group, and reinforced the notion of
menstruation as a discrediting attribute, which, as Seear
(2009) has argued, can influence help-seeking behaviour,
as will be demonstrated below.
Reproduction
Motherhood was important to the women in all the
groups. The Indian and Pakistani groups in particular
felt that women in their communities were defined by
this role, and emphasised the status that came with
motherhood, particularly from bearing male children.
The Greek women also spoke of the pressure on them
to have children:
‘You feel pressured to become a mother. It’s also not the
norm to say we don’t want to have children. It’s expected
of you, I think. Then if it’s not your own personal family,
your mother, father, it’s your in-laws and family around
you. Friends start having children once they get married,
you feel pressured from them as well. You start feeling,
you know, that something is wrong with yourself, so there
are loads of pressures around them to becoming a
mother.’
(Greek/Greek Cypriot woman)
For the Chinese and African Caribbean women, reproductionwas
seen more as an individual choice, and
members of these groups did not experience familial
or communal pressure to become mothers. The African
Caribbean group also spoke about the role of black
women changing from mother to provider, and the
importance of a career in fulfilling their lives in the
same way that that motherhood had done for previous
generations. There was less consensus among this group
about community perceptions of the importance of
motherhood, with one woman stating that, for men,
reproduction was an indication of their masculinity. A
woman who did not conceive might feel that she had
failed her husband or partner, who might then leave
her for someone with whom he could have children.
The only group that was unequivocal in their view
that it was acceptable for women not to have children
was the Chinese women, who reported that the pressure
to be educated and have a career was greater than
the imperative of motherhood. This may be reflective
of China’s population policies, particularly the ‘one
child’ policy.
‘According to Chinese tradition of course you should have
[a] child, but [we] won’t discriminate [against] you because
of that.’
(Chinese woman)
‘We have no pressure.’
(Chinese woman)
However, within this group all of the Chinese women
who had children felt pride in becoming mothers.
All of the groups felt that, as a result of living in the
UK, women’s ideas about motherhood were changing,
including the acceptability of working mothers and
smaller family size. As in earlier responses, generation
and assimilation appeared to be strong influencing
factors with regard to community groups’ views.
Although there were varying community views about
the importance of motherhood to women’s roles and
status, all reported negative views of involuntary
childlessness. The Caribbean group thought that infertility
was not a major problem within their community,
but one woman thought that this perception
might be because health issues of black women are
under-represented in the media. The Caribbean group
also thought that women would be willing to adopt
children, as did the Chinese, but this practice was
unacceptable to the Pakistani group.
Involuntary infertility was regarded as problematic
by the women in all of the groups, including the
Chinese and African Caribbean women, who were
more accepting of voluntary childlessness. Most of the
groups talked about the pity felt by the community for
infertile women. It was usually the woman who was
‘blamed’ for the inability to conceive, even when there
was no evidence of this, and women bore the brunt of
the stigma, as one Pakistani woman demonstrated.
‘The in-laws give them a hard time, and the husband as
well, and they’re under constant pressure. Some are under
abuse as well, mental and physical.’
(Pakistani woman)
The Chinese, Pakistani and African Caribbean groups
thought that in their communities some men in
childless relationships might look for a woman who
could have children. The Pakistani and Chinese women
thought that men would divorce their wives in order
to do this, but the African Caribbean women thought
that men would take an additional partner instead. A
Pakistani woman commented:
‘If the woman does not have a child the man would just
leave them, they won’t have themselves checked out, and
they’ll just divorce the wife and move on. And later on
maybe find out they’re the ones with the problem.’
(Pakistani woman)
Within the African Caribbean community the reaction
to infertility, as expressed below, was in contrast
to the acceptability of voluntary childlessness
reported above.
‘A woman may feel she has failed her husband or partner,
who may then move on to someone who can conceive. It
then means the woman must decide whether to leave him
or to share him with another, which as a woman I find
unacceptable.’
(African Caribbean woman)
In the communities where there was an expectation
that women would reproduce, childlessness, whether
voluntary or involuntary, was stigmatised; childless
women felt pressure from family and a sense of worthlessness.
In the African Caribbean community, where
women reported greater acceptability of voluntary
childlessness, infertility was nevertheless stigmatised
in a similar way. These findings confirm those of Culley
et al. (2006), who highlighted the considerable stigma
attached to involuntary childlessness in British South
Asian communities. However, it is also clear that
generation and educational background influence
women’s ability to resist such stigma. There is little
information available about perceptions of infertility
in other minority ethnic groups in the UK. Although
there are some similarities in understandings and
perceptions of infertility in these accounts and reports
of the dominant white community (Letherby, 2002),
there are also areas of cultural specificity.
Endometriosis
The above discussion has provided a glimpse of the
way in which different cultures view aspects of femaleness.
When we moved on to discuss awareness and
cultural perceptions of endometriosis we found that
most of the women had not heard of the disease, and
there were differingways in which theywould respond
to its symptoms. The groups were all shown diagrams
of the female pelvic anatomy by the facilitators, and an
explanation of endometriosis was given. Following
this all of the groups asked questions and were keen to
know more, expressing the view that more information
needed to be available. One participant in
the Indian group and two participants in the Greek
group had been diagnosed with endometriosis, but
no one in the other groups even knew anyone who
suffered from the condition.
The groups all wondered how to tell a ‘painful
period’ from the pain of endometriosis. The discussion
reflected that about menstruation, and many
of the participants felt that, in their community,
women would think that it was normal, and would
discuss it with friends and family rather than seek
professional help.
‘Women in our community would treat it as a normal
period and dismiss it.’
(Pakistani woman)
‘I don’t think there is much she can do, we all have
different periods, different symptoms. It is relative to
how you feel. What some people call painful periods to
others are not.’
(African Caribbean woman)
Normalisation of period pain, and the problems for
women of either differentiating their pain themselves,
or of having others take them seriously, are a feature of
much research on endometriosis (Denny, 2004b;
Ballard et al, 2006; Markovic et al, 2008). Seear (2009)
argues that this is compounded by the secretive and
stigmatised way inwhich menstruation is dealt with in
most societies.
Some women seemed to think that the experience of
deep dyspareunia would be a more likely trigger for
help seeking than painful periods, but even on this
there was not universal agreement. It was generally
agreed that inability to become pregnant would lead
them to seek help from their general practitioner, but
the women in the Chinese group felt that friends and
partners might be consulted in the first instance.
However, there was some disagreement within this
group.
C9: ‘I think it must be the doctor, they won’t talk to
others.’
C3: ‘I think they would talk to people around her and then
go to see the doctor.’
C2: ‘ I think they will not talk to people around her, she
must talk to her husband, but if it is abnormal, I think if
there is pain it should be abnormal, and will then go to see
GP, I think.’
Opinions about painful intercourse reflected the earlier
discussion on menstruation. For the African Caribbean
group, sex was regarded as a private topic and one that
was not readily discussed. The Pakistani and Indian
groups reported that, in their communities, women
would feel embarrassed to discuss painful intercourse
except with a female doctor. The women in the Indian
focus group were initially silent, and this was followed
by nervous laughter at the mention of painful sex.
‘An Asian man would not understand this ... [all agree]. ...
I am not blaming all Asian men, but some Asian men do
not understand that sex can be painful for some women,
but they would not understand and when he does not
understand what his wife is going through he would just
demand it ... and so for her [for the woman] it would be a
stigma because if he cannot have what he wants ...’
(Indian woman)
‘I think when the man knows it’s to do with sex he would
tell her to go to the doctors and sort it out, otherwise he
wouldn’t get any sex.’
(Pakistani woman)
The African Caribbean women were most likely to
refrain from sexual activity if it was painful. As one of
them commented, ‘If I had sex and it was painful, then
I just wouldn’t want it.’ However, many women in all
of the groups worried about the effect of abstention on
their husbands, and it seemed to be their husband’s
needs rather than their own pain that that these
women would respond to.
The common symptoms of endometriosis, menstrual
pain, painful sexual intercourse and infertility
are all problematic in terms of help-seeking behaviour.
The social stigma of menstruation constituted a barrier
to open discussion and help seeking, although
conversely the stigma of infertility provided an impetus,
which could lead to a diagnosis of endometriosis.
Discussion
In each of the groups the women spoke freely about
the issues that were raised. Their discussions highlighted
similarities and differences between the five
groups and between them and the white majority
population. This is consistent with the findings of
other research (Atkin and Chattoo, 2006; Salway et al,
2007). They also highlighted differences within each
community group, and the influence of generation and
acculturation on the views of women. For example,
one Indian woman commented:
‘The children raised in this country are very confused.
Many a time even we are confused about what is going on
around us. So we cannot explain our culture and concepts
to our children. So we blame the children and find fault
with them.Wecan try and teach them in our way, but they
question our ways and ask if there is anything wrong with
the culture in school and at work.’
The main limitation of the study was the representativeness
of the sample. The focus groups were recruited
via the community facilitators or the researchers’ own
contacts, and consisted of well-educated, Englishspeaking
women who had some level of acculturation
into UK society. They were also willing to discuss
sensitive issues about reproduction in an open forum.
We were not able to recruit women who lived in
communities with little contact outside of their own
ethnic group, or those unable to speak English confidently.
The exclusion of these women may mean that
we failed to capture a sufficiently diverse perspective of
the issues under discussion.
The data illustrate the potential significance of the
cultural context of the experience of endometriosis,
and demonstrate that although the women shared
experiences that transcended culture, each individual
group also discussed issues that were specific to them.
For example, the economic independence of the African
Caribbean women was unique to that group, and
cultural taboos surroundingmenstruationwere stronger
in the Pakistani group than in the other groups.
The data also show that women within the five
ethnic groups had multiple identities, or intersecting
statuses, that transcended ethnicity (Culley andHudson,
2009). They were clear that aspects of their ethnic
identity were important. However, other social divisionswere
much in evidence both within and between
the groups. Perhaps the most obvious of these was
generation, with all of the groups discussing the impact
of living in the UK on traditional beliefs, and expressing
the view that there were significant differences
between those who had migrated to theUKas children
or adults and those who were born and educated
within the host society (Bradby, 2007). Thus, younger
women were viewed as being less focused on the home
and more engaged in higher education and paid work.
However, most still retained responsibility for the
home and children, but saw this role as undervalued
both by men within their community and by society
more generally. However, the younger Greek women
spoke more of the dual responsibility of men and
women, rejecting the ‘double shift’ of their mothers’
generation. Probably the starkest difference between
the generations was expressed by the African Caribbean
women, where young women with good educational
qualifications viewed themselves as empowered and
independent. Here generation, gender and level of
education all intersected with ethnicity to produce a
complex articulation of concepts of menstruation and
motherhood. This complexity serves to repudiate a
deterministic notion of ethnicity as fixed; rather it
suggests a cultural fluidity (Culley and Hudson, 2009),
and the dangers of generalisations that are based on
categories of ethnicity.
This fluidity is highlighted by the relationship between
individual choices and family and community obligations.
Discussions about reproduction and (in)fertility
illustrated this very well. All of the groups, to
some extent, demonstrated adherence to pronatalist
cultural values in common with most other societies.
The Indian and Pakistani groups viewed having children
as the primary purpose of marriage, and felt great
personal and community pressure to start a family
soon after marriage. The Greek women also reported
pressure from family and friends to have children.
Decisions on optimum family size were also assumed
to be of community concern, in contrast to the dominant
white culture, which would view such matters
as a personal choice (Gillespie, 2003). Although such pressure was difficult to resist, particularly in closeknit
communities, younger women were reported to
be delaying childbearing and developing careers, making
decisions about their own families for themselves,
rather than in response to community obligation.
Within the African Caribbean and Chinese communities,
reproduction was seen as a personal choice rather
than a community concern, although these two groups
made a distinction between voluntary and involuntary
childlessness. This relationship between personal choice,
family and community obligation is shifting in most
communities as strong ties to the country of origin
loosen and the balance of people’s motives for having
children moves from the economic to the social and
psychological (Guˆ rtin-Broadbent, 2009). Both conformity
and resistance to cultural norms were apparent
within all of the groups.
One theme running through the discussions on
menstruation, reproduction and the symptoms of
endometriosis was that of stigma. Although only the
African-Caribbean group actually used this term, all of
the groups described stigmatising acts and attitudes.
In his seminal work on stigma, Goffman (1963, p. 14)
describes ‘discreditable’ individuals whose stigma is
not immediately apparent, and argues that they are
often labelled as weak. The stigma of menstruation is
reinforced by rituals and behaviours that are common
within most religions, such as the restrictions on food
handling and preparation mentioned by the African-
Caribbean, Indian and Pakistani groups. In contrast to
the study by Seear (2009), we also found some positive
aspects ofmenstruation, as a perceived cleansing process,
or a marker of a (non-)pregnant state. The important
point here is the consequence of menstruation as a
stigmatised state for help-seeking behaviour. Seear’s
study of Australian women’s experience of endometriosis
points to the stigma surrounding menstruation
positioning women as discreditable individuals, who
then conceal their menstrual state in order to avoid
social sanctioning. Where menstruation is problematic,
as is the case in symptomatic endometriosis, this
is complicit in the well-documented delay in diagnosis.
Seear’s findings are consistent with this study, in
which women had firm ideas about whom menstruation
should be discussed with, and even whether it
should be discussed openly at all. The exception to this
was the Greek group, who were very open with family
and friends of both sexes.
Although all of the ethnic groups demonstrated a
pronatalist culture, with infertility being regarded as a
deeply stigmatising state, within the Greek, Indian and
Pakistani groups this was particularly pronounced,
which is consistent with the findings of Culley and
Hudson (2009) in their study of South Asian women.
All of the groups spoke of the blame and stigma
attached to infertile women, and the fact that women
were always held responsible for lack of children within a marriage. Stigma is more likely to be discussed
in the literature on infertility (Donkor and
Sandall, 2007; Slade et al, 2007; McCarthy, 2008) than
in that on endometriosis. Imeson and McMurray
(1996) studied women’s experience of infertility, and
although they did not use the term ‘stigma’, they
reported that women felt socially isolated from their
peers and excluded from the social groupings that
come with parenthood.
Although much of the literature on endometriosis
discusses fertility and the possible threat posed to it by
the disease (Butt and Chesla, 2007; Denny, 2009),
most of this discussion is about the importance
attached to various symptoms both by women and
by health professionals. For example, Markovic et al
(2008) suggest that infertility is taken more seriously
than other symptoms of endometriosis, and Seear
(2009) states that women who present to health
services with infertility will receive an endometriosis
diagnosis in around half the time that other women
do.
An important finding of this study was the suggestion
that, for some minority ethnic women, childlessness
rather than menstrual problems or pain would
perhaps be the major motivating factor for seeking
professional help for symptoms of endometriosis.
This is in contrast to women from the majority community,
where those presenting with infertility who
are subsequently found to have endometriosis frequently
report no other symptoms (JK Gupta, Professor
of Obstetrics and Gynaecology, personal communication,
2010).
Conclusion
The data presented here demonstrate some important
values and beliefs which are likely to influence the
understanding of endometriosis and behaviour in
relation to it.Many of these are consistent with research
about the dominant white community in the UK
(Letherby, 1999). The data also highlight issues where
there are likely to be significant differences, both within
and between groups. Although the women felt that
specific cultural values might influence the experience
of endometriosis, other markers of difference were
clearly also significant. When addressing issues relating
to cultural influences on women’s experience of
endometriosis and the provision of health services to
manage it, we are conscious of the need to avoid
essentialising culture and ethnicity (Culley, 2006;
Phillips, 2007). Culture is an important aspect of the
way in which people make sense of a health condition,
but at the same time it must be acknowledged that
other dimensions of identity, such as age, gender and
socio-economic status, will also influence experience to a greater or lesser extent (Nazroo, 1997). Culture
will not necessarily be the determining factor in a
health and illness experience or a healthcare encounter.
Barriers to accessing services may be caused by a
number of factors, not least the power relationships
inherent in biomedicine (Seear, 2009) and the difficulties
of accessing appropriate treatment that were
experienced by many of those with lower socioeconomic
status in the UK and elsewhere. Nevertheless,
this study suggests that an accessible service will
also need to take account of potentially important
socio-cultural differences in the experience of endometriosis,
which may provide additional barriers to
presentation to healthcare providers.
References
- Aspinall PJ and Jacobson B (2004) Ethnic Disparities in Health and Healthcare: a focused review of the evidence and selected examples of good practice. London: London Health Observatory.
- Atkin K and Chattoo S (2006) Approaches to conducting qualitative research in ethnically diverse populations. In: Nazroo J (ed) Health and Social Research in Multiethnic Societies. London: Routledge, pp. 95ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â115.
- Ballard K, Lowton K and Wright J (2006) WhatÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢s the delay? A qualitative study of womenÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢s experiences of reaching a diagnosis of endometriosis. Fertility and Sterility 86:1296ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â 301.
- Bhopal R (2007) Ethnicity, Race and Health in Multicultural Societies. Oxford: Oxford University Press.
- Bradby H (2007) Watch out for the aunties! Young British AsiansÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢ accounts of identity and substance use. Sociology of Health and Illness 29:656ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â72.
- Braun V and Clarke V (2006) Using thematic analysis in psychology. Qualitative Research in Psychology 3:77ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â101.
- Britton CJ (1996) Learning about ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ãâ¹Ã
âthe curseÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢: an anthropological perspective on experiences of menstruation.WomenÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢s Studies International Forum 19:645ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â53.
- Bryman A (2008) Social Research Methods, 3rd edn. Oxford: Oxford University Press.
- Butt FS and Chesla C (2007) Relational patterns of couples living with chronic pelvic pain from endometriosis. Qualitative Health Research 17:571ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â85.
- Chiu L-F and Knight D (1999) How useful are focus groups for obtaining the views of minority groups? In: Barbour RS and Kitzinger J (eds) Developing Focus Group Research: politics, theory and practice. London: Sage, pp. 99ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â112.
- Cox H, Henderson L and Henderson N (2003) Focus group study of endometriosis: struggle, loss and the medical merry-go-round. International Journal of Nursing Practice 9:2ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â9.
- Cramer DW and Missmer SA (2002) The epidemiology of endometriosis. Annals of the New York Academy of Sciences 955:11ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â22.
- Culley L (2006) Transcending transculturalism? Race, ethnicity and health-care. Nursing Inquiry 13:144ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â53.
- Culley L and Hudson N (2006) Diverse bodies and disruptive reproduction. International Journal of Diversity in Organisations, Communities and Nations 5:117ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â26.
- From womanhood to endometriosis 179 Culley L and Hudson N (2009) Commonalities, differences and possibilities: culture and infertility in British South Asian communities. In: Culley L, HudsonNand van Rooij F (eds) Marginalized Reproduction: ethnicity, infertility and reproductive technologies. London: Earthscan Books, pp. 97ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â116.
- Culley L, Hudson N, Rapport F et al (2006) British South Asian communities and infertility services. Human Fertility 9:37ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â45.
- Culley L, Hudson N and Rapport F (2007) Using focus groups with minority ethnic communities: researching infertility in British Asian communities. Qualitative Health Research 17:102ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â12.
- Damewood M, Kresch AJ, Metzger D et al (1997) Current approaches to endometriosis. Patient Care 31:34ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â43. Denny E (2004a) WomenÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢s experience of endometriosis. Journal of Advanced Nursing 46:641ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â8.
- Denny E (2004b) ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ãâ¹Ã
âYou are one of the unlucky onesÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢: delay in the diagnosis of endometriosis. Diversity in Health and Social Care 1:39ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â44.
- Denny E (2009) ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ãâ¹Ã
âI never know from one day to another how I will feelÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢: pain and uncertainty in women with endometriosis. Qualitative Health Research 19:985ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â95.
- Donkor ES and Sandall J (2007) The impact of perceived stigma and mediating social factors on infertility-related stress among women seeking infertility treatment in Southern Ghana. Social Science and Medicine 65:1683ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â94.
- Gillespie R (2003) Childfree and feminine: understanding the gender identity of voluntarily childless women. Gender and Society 17:122ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â36.
- Goffman I (1963) Stigma: notes on the management of spoiled identity. Harmondsworth: Penguin.
- Green J and Thorogood N (2004) Qualitative Methods for Health Research. London: Sage.
- Gunaratnam Y (2009) What difference does our difference make in researching infertility? In: Culley L, Hudson N and van Rooij F (eds) Marginalized Reproduction: ethnicity, infertility and reproductive technologies. London: Earthscan Books, pp. 80ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â94.
- GuÃÆÃââââ¬Ã¹ÃÆââ¬Å¡Ã¢ââ¬Ã rtin-Broadbent Z (2009) ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ãâ¹Ã
âAnything to become a motherÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢: migrant Turkish womenÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢s experiences of involuntary childlessness and assisted reproductive technologies in London. In: Culley L, Hudson N and van Rooij F (eds) Marginalized Reproduction: ethnicity, infertility and reproductive technologies. London: Earthscan Books, pp. 117ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â 33.
- Helman CG (2007) Culture, Health and Illness, 5th edn. London: Hodder Arnold. Huntington A and Gilmour JA (2005) A life shaped by pain: women and endometriosis. Journal of Clinical Nursing 14:1124ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â32.
- Imeson M and McMurray A (1996) CouplesÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢ experience of infertility: a phenomenological study. Journal of Advanced Nursing 24:1014ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â22.
- Jones G, Jenkinson C and Kennedy S (2004) The impact of endometriosis upon quality of life: a qualitative analysis. Journal of Psychosomatic Obstetrics and Gynecology 25: 123ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â33.
- Kidd PS and Parshall MB (2000) Getting the focus and the group: enhancing analytical rigor in focus group research. Qualitative Health Research 10:293ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â308.
- Kyama MC, DÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢Hooghe TM, Debrock S et al (2004) The prevalence of endometriosis among African-American and African-indigenous women. Gynecologic and Obstetric Investigation 57:40ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â2.
- Laws S (1990) Issues of Blood: the politics of menstruation. Basingstoke: Macmillan.
- Lessey BA (2000) Medical management of endometriosis and infertility. Fertility and Sterility 73:1089ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â96.
- Letherby G (1999) Other than mother and mothers as others: the experience of motherhood and non-motherhood in relation to ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ãâ¹Ã
âinfertilityÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢ and ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ãâ¹Ã
âinvoluntary childlessness.ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢ WomenÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢s Studies International Forum 22:359ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â72.
- Letherby G (2002) Childless and bereft? Stereotypes and realities in relation to ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ãâ¹Ã
âvoluntaryÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢ childlessness and womanhood. Sociological Inquiry 72:7ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â20.
- McCarthy MP (2008) WomenÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢s lived experience of infertility after unsuccessful medical intervention. Journal of Midwifery and WomenÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢s Health 53:319ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â24. Markovic M, Manderson L and WarrenN(2008) Endurance and contest: womenÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢s narratives of endometriosis. Health 12:349ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â67.
- Mead N and Roland M (2009) Understanding why some ethnic minority patients evaluate medical care more negatively than white patients: a cross-sectional analysis of a routine patient survey in English general practices. BMJ 339:b3450. doi10.1136/bmj.b3450.
- Mehta P (2005) Promoting Equity of Access to Genetic Healthcare. London: Genetic Interest Group.
- Nazroo J (1997) The Health of BritainÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢s Ethnic Minorities: findings from a national community survey. London: Policy Studies Institute.
- Phillips A (2007) MulticulturalismWithout Culture. Princeton, NJ: Princeton University Press.
- Ritchie J and Spencer L (1994) Qualitative data analysis for applied policy research. In: Bryman A and Burgess RG (eds) Analysing Qualitative Data. London: Routledge, pp. 173ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â94.
- Salway S, Platt L, Harriss K et al (2007) Long-term health conditions and disability living allowance: exploring ethnic differences and similarities in access. Sociology of Health and Illness 29:907ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â30.
- Seear K (2009) The etiquette of menstruation: stigmatisation, menstrual concealment and the diagnostic delay. Social Science and Medicine 69:1220ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â7.
- Shaw R, Soutter WP and Stanton S (eds) (2003) Gynaecology, 3rd edn. Edinburgh: Churchill Livingstone.
- Slade P, OÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢Neill C, Simpson AJ et al (2007) The relationship between perceived stigma, disclosure patterns, support and distress among new attendees at an infertility clinic. Human Reproduction 23:2309ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â17.
- Van Balen F and InhornMC(2002) Interpreting infertility: a view from the social sciences. In: Inhorn MC and van Balen F (eds) Infertility Around the Globe: new thinking on childlessness, gender and reproductive technologies. Berkeley, CA: University of California Press, pp. 3ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â32.
- Waterton C and Wynne B (1999) Can focus groups access community views? In: Barbour RS and Kitzinger J (eds) Developing Focus Group Research: politics, theory and practice. London: Sage, pp. 127ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â43.
- Whelan E (2003) Putting pain to paper: endometriosis and the documentation of suffering. Health 7:463ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â82. 180 E Denny, L Culley, I Papadopoulos et al
- Whelan E (2007) No one agrees except those of us that have it: endometriosis patients as an epistemological community. Sociology of Health and Illness 29:957ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â82.
- Wilkinson S (1999) How useful are focus groups in feminist research? In: Barbour RS and Kitzinger J (eds) Developing Focus Group Research: politics, theory and practice. London: Sage, pp. 64ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â78.


