Keywords
Dehydration; Evidence-Based Medicine; Resuscitation; Therapeutics
Dear Sir,
Acute pancreatitis is an acute inflammation of the pancreas associated with a high morbidity and even the risk of mortality [1, 2]. To date, there exists no specific treatment for this disease [3, 4, 5] and fluid therapy forms the cornerstone of management of these patients who present acutely to emergency departments around the world. There is a need to review the data on fluid resuscitation in acute pancreatitis to aid the development of evidence-based guidelines.
A systematic search of the scientific literature was carried out using EMBASE, PubMed/MEDLINE, and the Cochrane Central Register of Controlled Trials for the years 1965-2011 to obtain access to all publications, especially randomized controlled trials, systematic reviews, and meta-analyses involving the various factors related to the use of fluid resuscitation in acute pancreatitis.
The search strategy was that described by Dickersin et al. [6] with the appropriate specific search terms, namely, “acute pancreatitis”, “fluid resuscitation”, “haemoconcentration”, “hemoconcentration”, “fluids”, “pancreatitis”, “systematic”, and “randomized controlled trials”. All available major publications from the past 45 years were considered.
Using the above search strategy, a total of 12 studies were identified describing regimens for fluid therapy. These included two randomized controlled trials, one retrospective cohort study, and 9 reviews.
Rationale for Fluids in Acute Pancreatitis
The impact of retroperitoneal fluid losses and dehydration on the development of hypovolemia seen in patients with severe acute pancreatitis resulting in high mortality was recognized in the 1950s [7, 8]. Although, this fluid loss was largely shown to respond to intravenous fluid therapy [9, 10, 11], the initial understanding was that the shock was mainly due to a loss of red blood cells [12]. Thereafter, despite the link between hemoconcentration at admission and mortality in acute pancreatitis being suggested by Davis et al. [13] and Gray et al. [14], a reduction in hematocrit in the first 48 hours was considered a poor risk factor in acute pancreatitis [15, 16] as evidence by the scoring system proposed by Ranson et al. [11]. Ranson et al. [11] attributed the low hematocrit to pre-existing anemia encountered in alcoholics while Trapnell [16] founds the fall in hematocrit to correlate with internal hemorrhage. The early use of fluid therapy has certainly reduced early mortality in acute pancreatitis associated with hypovolemia. In the 1990s, the importance of hemoconcentration was re-visited by the group from the Brigham and Women’s Hospital in Boston [17, 18]. Since then, hemoconcentration based on a serum hematocrit level at admission has been consistently demonstrated to be linked to the development of pancreatic necrosis [19, 20, 21, 22]. Pancreatic microcirculation depends on circulating volume and responds poorly to other influences.
Available Evidence on Regimens for Fluid Therapy in Acute Pancreatitis
Human Studies
Table 1 lists the articles/studies involving fluids in acute pancreatitis [23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34], their conclusions, as well as, the level of evidence [35].
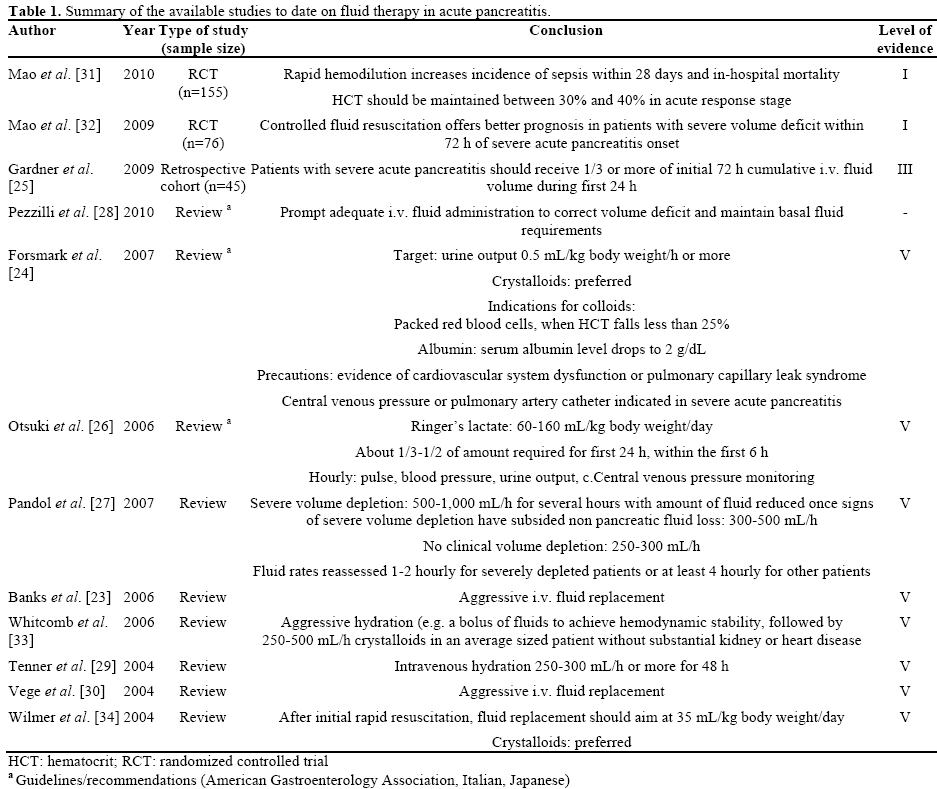
The only two randomized controlled trials till date have been based on studies conducted by Mao et al. [31, 32] In their first randomized controlled trial published in 2009, Mao et al. [32] randomized 76 patients within 72 hours of onset of severe acute pancreatitis to undergo either rapid fluid expansion (Group I; n=36) or controlled fluid expansion (Group II; n=40). They found that the patients in Group I had poorer outcomes based on measures such as higher APACHE II scores on days 1, 2, and 3 (P<0.05), greater need for mechanical ventilation (94.4% versus 65%; P<0.05), higher incidence of abdominal compartment syndrome and sepsis (P<0.05), and an overall lower survival rate (69.4% versus 90%; P<0.05).
In the second randomized controlled trial [31], Mao et al. randomized 115 patients within 24 hours of onset of severe acute pancreatitis to either undergo rapid hemodilution (hematocrit less than 35%; n=56) or slow hemodilution (hematocrit equal to 35% or more; n=59) over the next 48 hours. They found a higher incidence of sepsis in the rapid hemodilution group compared to the slow hemodilution group (P<0.01) with significant differences in the time interval to development of sepsis (7.4±1.9 days versus 10.2±2.3 days; P<0.01) in the first 28 days. The survival rate of the slow hemodilution group was also better (84.7% versus 66.1%; P<0.05).
The type of fluids used in the two studies included a combination of crystalloids (normal saline and/or lactated Ringer’s solutions) and colloids (plasma and 6% hydroxyl ethyl starch).
A retrospective cohort study by Gardner et al. [25] examined primary clinical outcomes including mortality, development of organ failure and duration of hospitalization in patients who received more than 33% (early resuscitation; n=17) or less than 33% (late resuscitation; n=28) of their cumulative 72-hour intravenous fluid volume within the first 24 h of presentation. They found that patients in the “late resuscitation” group experienced greater mortality than those in the “early resuscitation” group (18% versus 0%; P< 0.04) and demonstrated a trend toward greater rates of persistent organ failure (43% versus 35%; P=0.31).
Animal Studies
Animal studies conducted over the last four decades [36, 37, 38, 39, 40, 41] have aided our understanding of fluid resuscitation in overcoming microcirculatory disturbances in acute pancreatitis and attenuating endorgan injury. However, in the context of aiding the decision on the choice of fluid in the clinical setting, the results have not been particularly helpful.
Conclusions
Based on the review of literature we can conclude that hemoconcentration in a patient with acute pancreatitis (based on serial measurements of hematocrit) within the first 48 hours of admission is a marker of poor prognosis and indicates the need for fluid resuscitation. The ideal cut-off level for serum hematocrit (44% or 47%) remains to be determined. What can also be concluded from the available literature is that fluid therapy remains the cornerstone in the early management of acute pancreatitis and especially in the prevention of severe acute pancreatitis. In patients who go on to develop severe acute pancreatitis either due to a late presentation or despite resuscitation, fluid therapy has the potential to reduce the progression of pancreatic necrosis and its associated risk of mortality.
In 2008, Gardner et al. [42] reviewed the available evidence on fluid resuscitation in acute pancreatitis and found that there was a paucity of evidence to support clinical recommendations at that time. To date, there continues to be a lack of high-level evidence to guide the ideal “initial” fluid strategy for all patients presenting with acute pancreatitis in terms of choice of fluid, namely crystalloids and/or colloids, and if crystalloids, Ringer’s lactate or normal saline, as well as in terms of rate of administration. While crystalloids appear to be the ideal choice based on expert opinion and the guidelines/recommendations from America, Italy and Japan [23, 24, 26, 27, 28, 29, 30, 33, 34], these recommendations are not based on high-level evidence in patients with acute pancreatitis. In patients with severe acute pancreatitis, the two randomized trials available [31, 32] used a combination of crystalloids and colloids, and favored controlled resuscitation over rapid infusion within the first 72 hours. Considering that both these trials were performed by the same group, these results need to be validated by other groups.
There has been no further impetus even in animal studies since the last major review by Gardner et al. [42]
In conclusion, fluid therapy remains the mainstay of early management of patients with acute pancreatitis and severe acute pancreatitis. High-level evidence is lacking to guide protocols for fluid resuscitation in patients presenting with acute pancreatitis. In those patients with severe acute pancreatitis, the available evidence indicates that controlled fluid resuscitation with crystalloids and colloids offers the best outcome. Hematocrit remains a useful marker to guide fluid resuscitation in acute pancreatitis. However, the timing and ideal “cut-off” level needs to be determined.
Conflicts of interest
None declared
References
- Barreto S, Rodrigues J. Acute pancreatitis in Goa - a hospital based study. J Indian Med Assoc 2008; 106:575-6, 578. [PMID: 19552084]
- Barreto S, Rodrigues J. Comparison of Apache II and Imrie scoring systems in predicting the severity of acute pancreatitis. World J Emerg Surg 2007; 2:33. [PMID 18067678]
- Barreto S, Carati C, Schloithe A, Mathison R, Davison J, Toouli J, et al. The efficacy of combining feg and galantide in mild caerulein-induced acute pancreatitis in mice. Peptides 2010; 31:1076- 82. [PMID 20214943]
- Barreto S, Carati C, Schloithe A, Toouli J, Saccone G. The combination of neurokinin-1 and galanin receptor antagonists ameliorates caerulein-induced acute pancreatitis in mice. Peptides 2010; 31:315-21. [PMID 19944731]
- BarretoSG, Bazargan M, Zotti M, Hussey DJ, Sukocheva OA, Peiris H, et al. Galanin receptor 3 - a potential target for acute pancreatitis therapy. Neurogastroenterol Motil 2011; 23:e141-51. [PMID 21303427]
- Dickersin K, Scherer R, Lefebvre C. Identifying relevant studies for systematic reviews. BMJ 1994; 309:1286-91. [PMID 7718048]
- Keith LM, Jr., Watman RN. Blood volume deficits in pancreatitis. Surg Forum 1955; 5:380-84. [PMID 13247057]
- Siler VE, WulsinJH. Consideration of the lethal factors in acute pancreatitis. AMA Arch Surg 1951; 63:496-504. [PMID 14868204]
- Elliott DW. The mechanism of benefit derived from concentrated human serum albumin in experimental acute pancreatitis. Surg Forum 1955; 5:384-90. [PMID 13247058]
- Elliott DW, ZollingerRM, Moore R, Ellison EH. The use of human serum albumin in the management of acute pancreatitis; experimental and clinical observations. Gastroenterology 1955; 28:563-87; discussion, 588-92. [PMID 14366120]
- RansonJH, Rifkind KM, Roses DF, Fink SD, Eng K, Spencer FC. Prognostic signs and the role of operative management in acute pancreatitis. Surg Gynecol Obstet 1974; 139:69-81. [PMID 4834279]
- ZollingerRM, Keith LM, Jr., Ellison EH. Pancreatitis. N Engl J Med 1954; 251:497-502. [PMID 13203731]
- Davis CE, Jr., Amir-Jahed AK, ChalkleyMR, Jr., Richardson GS. Fatal acute pancreatitis. A survey. Va Med Mon (1918) 1962; 89:578-83. [PMID 14025455]
- Gray SH, Rosenman LD. Acute pancreatitis. The significance of hemoconcentration at admission to the hospital. Arch Surg 1965; 91:485-9. [PMID 14332409]
- Jacobs ML, Daggett WM, CivetteJM, Vasu MA, Lawson DW, Warshaw AL, et al. Acute pancreatitis: Analysis of factors influencing survival. Ann Surg 1977; 185:43-51. [PMID 831635]
- Trapnell JE. The natural history and prognosis of acute pancreatitis. Ann R CollSurgEngl 1966; 38:265-87. [PMID 5939282]
- Baillargeon JD, Orav J, Ramagopal V, Tenner SM, Banks PA. Hemoconcentration as an early risk factor for necrotizing pancreatitis. Am J Gastroenterol 1998; 93:2130-4. [PMID 9820385]
- Brown A, Orav J, Banks P. Hemoconcentration is an early marker for organ failure and necrotizing pancreatitis. Pancreas 2000; 20:367-72. [PMID 10824690]
- Lankisch PG, Mahlke R, Blum T, Bruns A, Bruns D, Maisonneuve P, et al. Hemoconcentration: An early marker of severe and/or necrotizing pancreatitis? A critical appraisal. Am J Gastroenterol 2001; 96:2081-5. [PMID 11467635]
- Muddana V, Whitcomb DC, Khalid A, Slivka A, Papachristou GI. Elevated serum creatinine as a marker of pancreatic necrosis in acute pancreatitis. Am J Gastroenterol 2009; 104:164-70. [PMID 19098865]
- Remes-Troche JM, Duarte-Rojo A, Morales G, Robles-Diaz G. Hemoconcentration is a poor predictor of severity in acute pancreatitis. World J Gastroenterol 2005; 11:7018-23. [PMID 16437609]
- Wu BU, Conwell DL, Singh VK, Repas K, Maurer R, Bollen TL, et al. Early hemoconcentration is associated with pancreatic necrosis only among transferred patients. Pancreas 2010; 39:572-6. [PMID 20182394]
- Banks PA, Freeman ML. Practice guidelines in acute pancreatitis. Am J Gastroenterol 2006; 101:2379-2400. [PMID 17032204]
- Forsmark CE, Baillie J. AGA institute technical review on acute pancreatitis. Gastroenterology 2007; 132:2022-44. [PMID 17484894]
- Gardner TB, Vege SS, Chari ST, Petersen BT, Topazian MD, Clain JE, et al. Faster rate of initial fluid resuscitation in severe acute pancreatitis diminishes in-hospital mortality. Pancreatology 2009; 9:770-6. [PMID 20110744]
- Otsuki M, Hirota M, Arata S, Koizumi M, Kawa S, Kamisawa T, et al. Consensus of primary care in acute pancreatitis in Japan. World J Gastroenterol 2006; 12:3314-23. [PMID 16733846]
- PandolSJ, Saluja AK, ImrieCW, Banks PA. Acute pancreatitis: Bench to the bedside. Gastroenterology 2007; 132:1127-51. [PMID 17383433]
- Pezzilli R, Zerbi A, Di Carlo V, Bassi C, DelleFave GF, et al. Practical guidelines for acute pancreatitis. Pancreatology 2010; 10:523-35. [PMID 20975316]
- Tenner S. Initial management of acute pancreatitis: Critical issues during the first 72 hours. Am J Gastroenterol 2004; 99:2489- 94. [PMID 15571599]
- SwaroopVS, Chari ST, Clain JE. Severe acute pancreatitis. JAMA 2004; 291:2865-8. [PMID 15199038]
- Mao EQ, Fei J, PengYB, Huang J, Tang YQ, Zhang SD. Rapid hemodilution is associated with increased sepsis and mortality among patients with severe acute pancreatitis. Chin Med J (Engl); 123:1639- 44. [PMID 20819621]
- Mao EQ, Tang YQ, Fei J, Qin S, Wu J, Li L, et al. Fluid therapy for severe acute pancreatitis in acute response stage. Chin Med J (Engl) 2009; 122:169-73. [PMID 19187641]
- Whitcomb DC. Clinical practice. Acute pancreatitis. N Engl J Med 2006; 354:2142-50. [PMID 16707751]
- Wilmer A. ICU management of severe acute pancreatitis. Eur J Intern Med 2004; 15:274-80. [PMID 15450983]
- Wright JG, Swiontkowski MF, Heckman JD. Introducing levels of evidence to the journal. J Bone Joint Surg Am 2003; 85-A:1-3. [PMID 12533564]
- Horton JW, Dunn CW, Burnweit CA, Walker PB. Hypertonic saline-dextran resuscitation of acute canine bile-induced pancreatitis. Am J Surg 1989; 158:48-56. [PMID 2472751]
- Kerner T, Vollmar B, Menger MD, Waldner H, Messmer K. Determinants of pancreatic microcirculation in acute pancreatitis in rats. J Surg Res 1996; 62:165-71. [PMID 8632634]
- Knol JA, Inman MG, Strodel WE, Eckhauser FE. Pancreatic response to crystalloid resuscitation in experimental pancreatitis. J Surg Res 1987; 43:387-92. [PMID 3682803]
- Schmidt J, Fernandez-del Castillo C, RattnerDW, Lewandrowski KB, Messmer K, Warshaw AL. Hyperoncotic ultrahigh molecular weight dextran solutions reduce trypsinogen activation, prevent acinar necrosis, and lower mortality in rodent pancreatitis. Am J Surg 1993; 165:40-4. [PMID 7678189]
- Shields CJ, Sookhai S, Winter DC, Dowdall JF, Kingston G, Parfrey N, et al. Attenuation of pancreatitis-induced pulmonary injury by aerosolized hypertonic saline. Surg Infect (Larchmt) 2001; 2:215-23. [PMID 12593711]
- Shields CJ, Winter DC, Sookhai S, Ryan L, Kirwan WO, Redmond HP. Hypertonic saline attenuates end-organ damage in an experimental model of acute pancreatitis. Br J Surg 2000; 87:1336- 40. [PMID 11044157]
- Gardner TB, Vege SS, Pearson RK, Chari ST. Fluid resuscitation in acute pancreatitis. Clin Gastroenterol Hepatol 2008; 6:1070-76. [PMID 18619920]

