Keywords
Cyst Fluid; GNAS protein, human; KRAS protein, human; Loss of Heterozygosity; Pancreatic Cyst
INTRODUCTION
The widespread use of cross-sectional imaging has led to the increased detection of pancreatic cysts. Cysts detected include inflammatory pseudocysts, benign SCNs (serous cystadenomas), mucinous lesions (MLs), and cystadenocarcinomas. Today, among the most frequently detected pancreatic cysts are mucinous lesions [1]. MCN’s (mucinous cystic neoplasms) are mucin-producing and septated cyst-forming epithelial neoplasias of the pancreas with a distinctive ovarian-type stroma. Also detected with increasing frequency are IPMNs. IPMNs are neoplasms that grow within the pancreatic ducts and side branches characterized by the production of thick, mucinous fluid. MCNs and IPMNs are mucinous lesions (MLs). Given their known malignant potential, yet unclear natural history and rate of progression, resection of these lesions is usually recommended [2]. EUS (Endoscopic Ultrasound) with fine-needle aspiration and cyst fluid analysis is routinely used to evaluate pancreatic cysts. There are no reliable radiologic criteria to distinguish benign and premalignant from malignant cysts [3]. Current methods to evaluate pancreatic cysts rely heavily on imaging and cyst fluid aspirate analysis. However, cytologic analysis of cyst aspirate is complicated by acellular specimens. Cyst fluid CEA level is considered the best indicator of a mucinous cyst [4]. Unfortunately, it cannot predict the likelihood of an existing or developing malignancy. Tools to better assess the malignant potential of MCNs would help physicians offer better guidance to their patients. This is especially important in our older patients with higher surgical risk.
The progression of pancreatic mucinous cysts to pancreatic cancer hinges on genetic mutations and chromosomal deletions. In comparison to benign cysts, those cysts with underlying malignancy have higher cell turnover resulting in more frequent mutational damage reflected in the DNA mutations and changes seen in fluid analysis. Moreover, cyst epithelial cells with a high rate of turnover would contribute more DNA [4]. Accordingly, malignant cyst fluid should be enriched with DNA, and analysis of pancreatic cyst fluid should allow for detection of malignancy. The overall low specificity of the current diagnostic methods and need for DNA amplification methods has led to the development of new molecular testing capabilities. PCR amplification tests of DNA from the cells shed from mucinous cyst wall lining provides opportunity for accurate fluid analysis even when the amount of fluid aspirate is small [5].
Genetic analysis of interest included detection of KRAS (Kirsten rat sarcoma viral oncogene homolog) mutations, GNAS (Guanine Nucleotide Binding Protein Alpha Stimulating Complex Locus) mutations, and allelic imbalance (loss of heterozygosity; LOH). The KRAS gene is an oncogene that provides instructions for making a protein called K-RAS that is involved primarily in regulating cell division. The KRAS gene is in the Ras family of oncogenes and the proteins it produces encodes various GTPases which play important roles in cell division, cell differentiation, and apoptosis. When mutated, KRAS has the potential to cause normal cells to become cancerous. The GNAS complex locus is a protein in humans which is encoded by the GNAS gene. The protein encoded by this gene is the stimulatory G-protein alpha subunit (Gs-α), a key component of many signal transduction pathways linking receptor-ligand interactions with the activation of adenylyl cyclases and a variety of cellular responses. When the Gs-α subunit is mutated, the resulting dysregulation of classical signal transduction pathways can lead to cancerous growth. Loss of heterozygosity (LOH) was determined using microsatellite markers linked to a broad panel of genomic loci associated with tumor suppressor genes. Loss of tumor suppressor genes is associated with cancer development.
With this in mind, our study evaluated whether EUS imaging, cyst fluid CEA, and cytology combined with cyst fluid genetic analyses for the presence of KRAS mutations, GNAS mutations, and allelic imbalance (LOH) can be used to better predict the malignant potential of pancreatic cysts.
METHODS
In a retrospective analysis, we collected data from seventytwo patients (43 women and 29 men, mean age 66 (30-84)) with pancreatic cysts who underwent EUS with FNA by a single operator (VE) from 2010 to 2013. The study was approved by the Institutional Review Board at Torrance Memorial Medical Center in Torrance, California.
Follow-up data was obtained over a range of 1 to 3 years with a median follow-up time of 2.2 years. EUS was performed with a GF UE160 radial echoendoscope, Olympus Inc. FNA was performed with a GF UTC 180 linear array echoendoscope, Olympus Inc. Both echoendoscopes were used in sequence for the first EUS procedure on a regular basis. In subsequent endosonographies, only the linear echoendoscope was used. The aspirated cyst fluid was analyzed for the presence of CEA, KRAS mutations, GNAS mutations, and allelic imbalance (LOH) using a molecular test – PathFinder TG; RedPath Integrated Pathology, Inc. based out of Pittsburgh, Pennsylvania. Fluid was also sent for cytology. Minimum fluid for testing was 200 microliters or 0.2 milliliters for neat testing. Analysis of cyst fluid quantity less than 200 microliters was always attempted in less dilution with a comment on the final report. Samples were shipped at 2-8°C with cold packs. Neat samples were also stored at 2-8°C. Of note, for frozen fresh samples, extracted DNA was frozen at -20°C for long term storage.
Based on RedPath molecular reports in combination with patient (demographics, presenting symptoms) and index EUS characteristics, cyst fluid genetic analyses were reported as benign, statistically indolent, or aggressive.
Patient follow-up data from the time of the index EUS to July 2013 included surveillance EUS or MRI every 6 months or annually. Cysts considered to be non-benign were followed every six months or referred for surgery. Cysts diagnosed as benign were followed at longer intervals.
A final diagnosis was based on combined evidence of endoscopic features (presence of cyst solid nodules, thick septations, wall thickness), fluid CEA level, and final pathology specimens obtained endoscopically or surgically. Cysts with lack of endoscopic or MRI features concerning for malignancy or benign pathology were diagnosed as benign. Cysts with one or more features including features on endoscopy or MRI concerning for malignancy or malignant pathology were diagnosed as non-benign or containing highly malignant potential.
Pancreatic cysts were evaluated and categorized as follows: cysts thought to be serous contained CEA <5 ng/ml, no cyst nodules or cyst wall thickening on EUS and watery aspirate. Cysts categorized as mucinous contained CEA >192 ng/ml and/or viscous aspirate. Cysts categorized as branch duct intraductal papillary mucinous neoplasm contained CEA >192 ng/ml, EUS characteristics consistent with IPMN such as connection with the pancreatic duct and watery or viscous aspirate. An indeterminate cyst contained CEA < 192 ng/ml, no mucinous aspirate, and no connection to the pancreatic duct.
One-hundred and 14 patients were screened for the study. Forty-two patients were excluded (Figure 1). Exclusion criteria included those patients with pseudocyst, overt cancer invasion or metastasis by EUS or imaging, and presence of other malignancies. Inclusion criteria included > 18 years of age, cystic fluid analysis consistent with a mucinous or indeterminate cyst, and complex cysts by EUS.
Figure 1. Pancreatic cysts.
STATISTICS
All statistical analyses were performed by using SAS/ STAT v. 9.2. (reference: SAS Institute Inc. 2010. SAS®9.2 Language Reference: Concepts, Second Edition. Cary, NC: SAS Institute Inc. – Biostatistician Eunyoung Song).
RESULTS
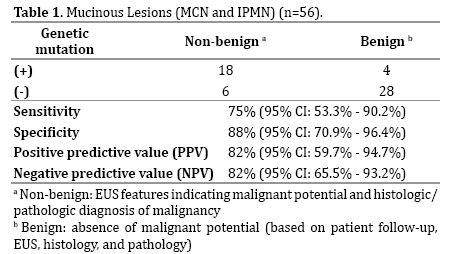
Seventy-two patients who underwent endoscopic ultrasound with fine-needle aspiration were eligible for the study revealing 39 IPMN’s, 17 MCN’s, and 16 SCN’s based on EUS findings and final pathologic specimens. All SCN’s were diagnosed as benign and contained a negative genetic analysis. Out of the 56 patients with pancreatic cysts with malignant potential (IPMNs & MCNs), 22 (39%) patients had pancreatic cysts with abnormal molecular fluid analysis (Table 1). Of those 22 patients, 18 contained a non-benign diagnosis based on EUS or conventional imaging features and final histology/pathology. This is consistent with cyst fluid genetic analysis carrying a sensitivity and specificity of 75% and 88%, respectively, and a positive predictive value of 82%. There was also a significant correlation between negative cystic fluid genetic analysis and exclusion of a non-benign course with a negative predictive value of 81%.
We examined IPMNs and MCNs individually. Of the 39 patients with IPMN’s, 16 (41%) patients had cyst fluid genetic analyses demonstrating either KRAS/GNAS mutation or allelic imbalance (LOH) or both (Table 2). Fourteen of those 16 patients (88%) contained cysts with a non-benign diagnosis, indicating a sensitivity of 70%, specificity of 90%, PPV 88%, and NPV 74%. Of the 17 patients with MCNs, 6 (35%) patients had abnormal genetic fluid analysis (Table 3). Four of those 6 patients (67%) contained cysts with a non-benign diagnosis. All patients with MCNs who did not have a genetic mutation had a benign course and a NPV of 100%. In contrast, all patients with a positive genetic mutation carried a nonbenign course showing a sensitivity of 100%, specificity of 85%, and a PPV of 67%.


Ultimately, 19 patients (Table 4) with findings suspicious for malignancy were referred for surgery. 11 patients were deemed poor surgical candidates. 2 patients declined surgery. Of the 6 remaining patients who underwent pancreatectomy, 5 patients had final pathology showing adenocarcinoma (1 patient was not diagnosed with malignancy). 4 out of 5 patients with adenocarcinoma contained cyst molecular analysis with KRAS mutations or LOH (Figure 1).


Additionally, we conducted a multivariable logistic regression analysis (Table 5) to evaluate the relationship between cyst fluid genetic mutation and risk of malignancy. Analyses showed that patients who had a positive genetic mutation in their cyst fluid were 6.74 times more likely to have a non-benign pancreatic cyst than patients who did not have a positive genetic mutation after adjusting for age and gender.

The results of the current study demonstrate a significant agreement between molecular diagnosis of PathFinder TG and malignant potential of pancreatic cysts. The 5 patients diagnosed with pancreatic adenocarcinoma ranged from age 60-80 (3 F, 2 M). Only 1 of the 5 patients was symptomatic, and only 1 of 5 patients had a cyst size > 3 cm. Only 2 out of 5 contained a solid component. The 3 accepted independently high-risk features for a cyst as described by the Sendai criteria [6] (size greater than 3 cm, presence of symptoms, and a cyst solid component), or the high risk features listed on the recently updated Fukuoka guidelines [7] (obstructive jaundice in the presence of a cyst in the head of the pancreas, an enhancing solid component within the cyst, a rapidly growing cyst size, or the presence of high-grade atypia on cytology) were not present in 40% of our patients who were diagnosed with adenocarcinoma. Our results showed that pancreatic cyst fluid KRAS mutation and LOH are independently associated with a non-benign course.
DISCUSSION
Preoperative diagnosis currently depends on a multidisciplinary approach that incorporates radiologic analysis, cyst fluid analysis, and cytology [8]. Analysis of cyst fluid for CEA level is considered the most accurate predictor of a mucinous cyst [4]. However, many incidental pancreatic cysts produce scant fluid insufficient for CEA quantification. Although radiologic features can be specific for some pancreatic cysts, most often it is insufficient to characterize non-inflammatory pancreatic cysts with imaging alone. The challenge in differentiating between pancreatic mucinous cysts with a benign course and those who are premalignant or malignant has led to the practice of resecting the majority of MLs found incidentally on routine imaging studies.
Though MLs constitute approximately 25% of all resected pancreatic cyst neoplasms, they are slow-growing neoplasms with an unclear natural history [9]. Because these neoplasms have a tendency to progress to malignancy and usually involve the body and tail of the pancreas, surgical resection is the recommended treatment [10]. MLs with features suspicious of invasive malignancy, such as size greater than 3 cm, presence of mural nodules, massforming lesions, and peripheral egg-shell calcifications, are treated with oncologic resections with lymphadenectomy [11]. In smaller lesions without other suspicious signs of malignancy, parenchyma-sparing procedures without lymphadenectomy such as middle pancreatectomy, spleenpreserving distal pancreatectomy, and laparoscopic resections are considered [12]. Overall, regardless of the size of the pancreatic lesion, the recommended treatment modality is often surgical resection. Unfortunately, a significant number of our patients will undergo major, high-risk surgery for a benign cyst. On the contrary, some patients may opt to defer surgery on a malignant cyst whose malignant potential is incompletely appreciated.
In terms of pancreatic cyst carcinogenesis, the pattern and rate of mutation accumulation ultimately leading to a malignant lesion is unclear and the significance of DNA markers – KRAS, GNAS, and LOH in combination and with respect to one another may vary [4]. An advantage of DNA molecular analysis is the small amount of fluid required for high performance. In the last decade, cyst aspirate CEA level has been accepted as the most accurate predictor of a nonbenign course in a ML. However, unless presenting with an extreme value, CEA level often lacks the ability to accurately predict risk for malignancy [4]. In addition, the amount of fluid aspirate obtained during FNA is often suboptimal for various reasons limiting the accuracy of the actual CEA level of a potentially malignant cyst [12]. It is reasonably accepted that benign pancreatic cysts (pseudocysts, SCNs) have a low rate of cell turnover and thus less DNA material in cyst fluid and wall lining surrounding the fluid. All our serous cysts had a negative DNA analysis. In contrast, a malignant cyst with uncontrolled epithelial cell growth should exhibit the highest cell turnover and contribute more DNA. Thus, analysis of pancreatic cystic fluid should be capable of detecting malignancy even if only a small amount of cyst aspirate is sampled.
Pancreatic MLs are challenging for clinicians to manage because of the difficulty to predict their potential for malignant behavior. We hope to deliver the most accurate assessment of a cyst’s biologic behavior to our patients so that they may receive the appropriate recommendation regarding surgical versus conservative management. We believe DNA damage including genetic mutations and allelic imbalance detected in pancreatic mucinous cysts reflect the pathology of the cysts. Resection of MLs with symptomatic presentation and/or solid component > 3 cm is widely accepted. However, not all MLs > 3 cm are malignant. Results of a large patient series of various cyst types suggest that size should not be used independently in management decisions [13]. Moreover, as evidenced in our study, all patients with mucinous cystic neoplasms regardless of size of the cyst who did not contain a genetic fluid mutation were diagnosed as benign indicating a NPV of 100%.
Recent studies support close monitoring for cysts that manifest a fluid KRAS mutation [14]. A 2013 retrospective analysis, collected data from fifty-one patients with pancreatic cysts who underwent EUS-FNA at a tertiary care center from June 2004 to June 2007. Detailed followup data obtained through October 2010 found KRAS mutations in cyst fluid were independently associated with a nonbenign course, and were associated with progression and development of malignancy in mucinous cysts [14]. Another recent study evaluated twenty-five patients with pancreatic cysts diagnosed on imaging who underwent EUS-FNA followed by surgical resection. In their results mutations in GNAS were found to have an oncogenic role in IPMN’s [15]. Nine cysts were classified as IPMN according to surgical pathology. Four of 9 (44%) IPMN patients carried a mutation in GNAS, all of which harbored various degrees of dysplasia [16]. We are in agreement with the current research.
Based on our results, the most sensitive and specific predictor of malignant potential in pancreatic cysts is the presence of DNA mutation or loss of heterozygosity. Of the patients included in our study, 75% of the patients with non-benign pancreatic cysts contained a Red Path Diagnosis with abnormal genetic fluid – based on the presence of either a KRAS mutation, GNAS mutation, LOH, or a combination. It is clear the KRAS/GNAS gene mutation and LOH are independent markers of malignant behavior in pancreatic cysts. More striking was the strong correlation (NPV of 82% and 100% for all MLs and MCNs, respectively) between the absence of cyst fluid DNA mutations and negative cyst malignant potential. For this reason, molecular analysis of pancreatic cyst fluid could be utilized in patients with potentially benign pancreatic cysts (especially those with elevated but non-specific CEA levels), and could help these patients avoid unneeded high-risk surgery.
We recommend asymptomatic cysts whose fluid analyses do not contain genetic changes be followed at longer intervals (based on symptoms or annual imaging) supported by the strong negative predicative value in our study. We recommend close monitoring with imaging (every 3-6 months) or surgical resection in those patients with cyst fluid analysis revealing a genetic mutation or allelic imbalance. With this in mind, clinicians can confidently recommend surgery to those patients who merit the intervention and offer regular follow-up to patients with likely benign cysts.
Overall, genetic analysis is best used in concert with endosonographic imaging, cytology, and standard cyst fluid analysis to make the most informed clinical decision as to whether a recommendation for surgery is appropriate, and to help guide follow-up in patients with neoplastic cysts. Our study strongly supports the value of molecular testing of pancreatic cyst fluid in predicting cyst behavior.
Conflict of Interest
The authors have no potential conflicts of interest
References
- Fernández-del Castillo C, Targarona J, Thayer SP, Rattner DW, Brugge WR, Warshaw AL. Incidental pancreatic cysts: clinicopathologic characteristics and comparison with symptomatic patients.. Arch Surg. 2003; 138: 433-434. [PMID: 12686529]
- Talukdar R, Reddy DN. Treatment of Pancreatic Cystic Neoplasm: Surgery or Conservative? Clinical Gastroenterology and Hepatology 2014; 12: 145–151. [PMID: 23978346]
- Ahmad NA, Kochman ML, Brensinger C, Brugge WR, Faigel DO, Gress FG, Kimmey MB, et al. Interobserver agreement among endosonographers for the diagnosis of neoplastic versus non-neoplastic pancreatic cystic lesions. Gastrointest Endosc. 2003; 58:59–64. [PMID: 12838222]
- Brugge WR, Lewandrowski K, Lee-Lewandrowski E, Centeno BA, Szydlo T, Regan S, del Castillo CF,et al. Diagnosis of pancreatic cystic neoplasms (a report of the cooperative pancreatic cyst study). Gastroenterology 2004; 126:1330–1336. [PMID: 15131794]
- Khalid A, McGrath KM, Zahid M, Wilson M, Brody D, Swalsky P, Moser AJ, et al. The role of pancreatic cyst fluid molecular analysis in predicting cyst pathology. Clin Gastroenterol Hepatol. 2005; 3:967–973. [PMID: 16234041]
- Tanaka M, Chari S, Adsay V, Fernandez-del Castillo C, Falconi M, Shimizu M, Yamaguchi K, et al. International consensus guidelines for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas. Pancreatology 2006; 6:17-32. [PMID: 16327281]
- Tanaka M, Fernández-del Castillo C, Adsay V, Chari S, Falconi M, Jang JY, Kimura W, et al. International consensus guidelines 2012 for the management of IPMN and MCN of the pancreas. Pancreatology 2012; 12: 183–197. [PMID: 22687371]
- Pitman MB, Deshpande V. Endoscopic ultrasound-guided fine needle aspiration cytology of the pancreas: a morphological and multimodal approach to the diagnosis of solid and cystic mass lesions. Cytopathology 2007; 18:331-347. [PMID: 17559566]
- Valsangkar NP, Morales-Oyarvide V, Thayer SP, Ferrone CR, Wargo JA, Warshaw AL, Fernández-del Castillo C. 851 resected cystic tumors of the pancreas. A 33-year experience at the Massachusetts General Hospital. Surgery 2012; 152 (Suppl 1): S4–S12. [PMID: 22770958]
- Fernandez-del Castilo C. Mucinous cystic neoplasms. J Gastrointest Surg 2008; 12: 411–413.
- Sperti C, Beltrame V, Milanetto A, Moro M, Pedrazzoli S. Parenchyma-sparing pancreatectomies for benign or border-line tumors of the pancreas. World J Gastrointest Surg 2010; 2: 272–281. [PMID: 2999190]
- Salvia R, Fernández-del Castillo C, Bassi C, Thayer SP, Falconi M, Mantovani W, Pederzoli P, et al. Main-duct intraductal papillary mucinous neoplasms of the pancreas: clinical predictors of malignancy and long-term survival following resection. Ann Surg. 2004; 239: 678–687. [PMID: 1356276]
- Walsh RM, Vogt DP, Henderson JM, Hirose K, Mason T, Bencsath K, Hammel J, et al. Management of suspected pancreatic cystic neoplasms based on cyst size. Surgery. 2008; 144: 677–685. [PMID: 18847654]
- Rockacy MJ, Zahid M, McGrath KM, Fasanella KE, Khalid A. Association Between KRAS Mutation, Detected in Pancreatic Cyst Fluid, and Long-term Outcomes of Patients. Clinical Gastroenterology and Hepatology 2013; 11: 425–429. [PMID: 23267865]
- Wu J, Matthaei H, Maitra A, Molin MD, Wood LD, Eshleman JR, Goggins M, et al. Recurrent GNAS mutations define an unexpected pathway for pancreatic cyst development. SciTransl Med. 2011; 3: 92ra66. [PMID: 3160649]
- Siddiqui AA, Kowalski TE, Kedika R, Roy A, Loren DE, Ellsworth E, Adler D. EUS-guided pancreatic fluid aspiration for DNA analysis of KRAS and GNAS mutations for the evaluation of pancreatic cystic neoplasia: a pilot study. Gastrointest Endosc. 2013. 77: 669-670. [PMID: 23498145]


