Keywords
erlotinib; gemcitabine; Neoplasm Metastasis; Pancreatic Neoplasms
Abbreviations
ASCO: American Society of Clinical Oncology; TTF2: time to treatment failure of second-line therapy
Introduction
Pancreatic cancer is the fourth leading cause of cancer related death among men and women in United States [1]. Patients diagnosed with pancreatic cancer typically have a poor prognosis which is attributable to the fact that most patients have metastatic disease at the time of diagnosis. For patients with metastatic disease, the median survival time is 3-6 months and the 5-year survival is less than 1% [2]. Treatment for stage IV pancreatic cancer may include palliative surgery and chemotherapy. Despite a palliative goal, single agent and combination chemotherapy trials have been conducted to measure response and survival rates with the approach of improving chance of remission and prolonging survival.
Until the introduction of gemcitabine, 5-fluorouracil (5-FU) was considered the standard treatment for advanced pancreatic cancer. The reported response rates for single-agent 5-FU ranged from 0% to 19% [3]. The median survival time for patients treated with single-agent 5-FU ranged from 4.2 months to 5.5 months [4]. Gemcitabine has become the cornerstone of chemotherapy for locally advanced and metastatic pancreatic cancer since 1997. This standard was established by a phase III trial in which 126 chemotherapy-naïve patients with advanced disease were randomized to receive either gemcitabine (1,000 mg/m2) or 5-FU (600 mg/m2). Both drugs administered as a 30 minutes infusion weekly for 7 weeks followed by 1 week off, and then weekly for 3 weeks of every 4 weeks [4]. Although, no statistically significant difference was found in the overall response rate between the two groups (5.4% for gemcitabine and 0% for 5-FU), the number of patient who experienced clinical benefit response (improvement in pain or Karnofsky performance status) was significantly greater in the gemcitabine group than 5-FU group (23.8% versus 4.8%, P=0.0022). The treatment of gemcitabine versus 5-FU was associated with improvement in the median overall survival (5.65 months versus 4.41 months, P=0.0025) and 1-year survival (18% versus 2%). In the last 10 years, a significant amount of studies on other agents comparing gemcitabine alone or gemcitabine-based combinations have been reported, such as gemcitabine with fluorouracil, capecitabine, cisplatin, docetaxel, irinotecan, oxaliplatin, or pemetrexed, and produced no clear survival benefit [5]. In the age of molecular targeted therapy, several classes of target agents have been evaluated in clinical trials. Only agents targeting human epidermal growth factor receptor (EGFR) have shown promise. In a phase III trial, the combination of gemcitabine (1,000 mg/m2 infused 30 minutes weekly for 7 weeks followed by 1 week off, and then weekly for 3 weeks of every 4 weeks) plus erlotinib (100 mg/day) versus gemcitabine alone showed statistically significant improvements in overall survival (6.2 months versus 5.9 months; hazard ratio (HR): 0.82; P=0.038) and 1-year survival (23% versus 17%, P=0.023) [6]. Erlotinib in combination with gemcitabine was approved by FDA for first-line treatment of patients with advanced pancreatic cancer. Although the survival improvement with the combination was statistically significant, it is questionable whether the two-week improvement in survival is clinically meaningful. Studies evaluating the combinations of gemcitabine with cetuximab or bevacizumab, or the combination of bevacizumab with gemcitabine and erlotinib have failed to report an overall survival benefit [5]. Several new front line treatment approaches in metastatic setting were presented at the 2010 American Society of Clinical Oncology (ASCO) Annual Meeting. The data from two phase III and two phase II trials (Table 1) are reviewed and discussed, which may have a positive impact to our current practice.
Updates from the 2010 ASCO Annual Meeting
Phase III studies
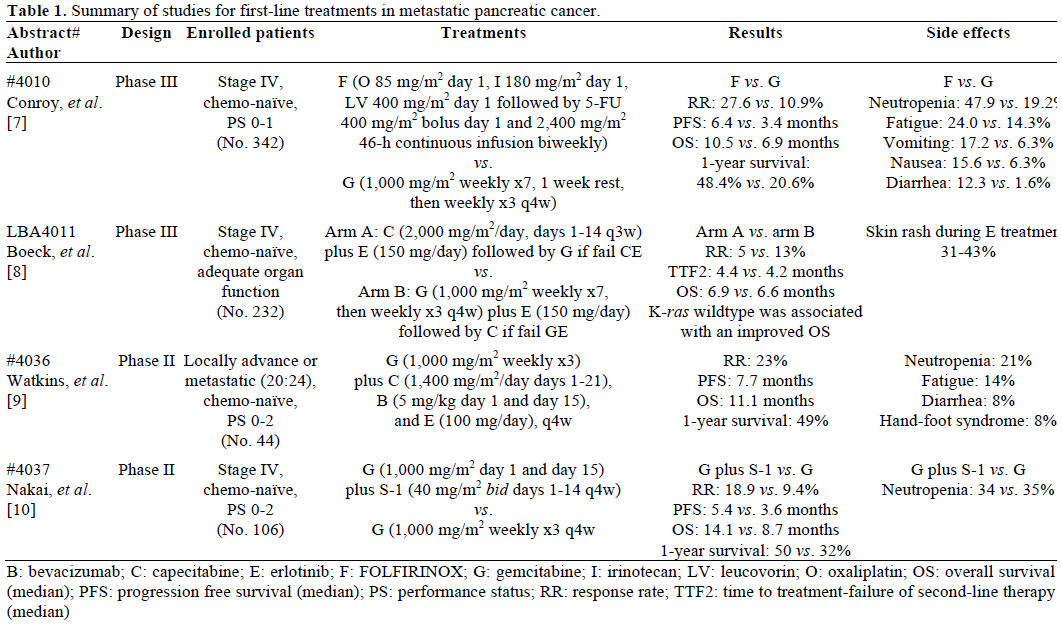
The PRODIGE 4/ACCORD 11 trial was conducted in France with a primary end point of overall survival (Abstract #4010) [7]. Three-hundreds and forty-two patients were randomized to received FOLFIRINOX (oxaliplatin 85 mg/m2, irinotecan 180 mg/m2, leucoviron 400 mg/m2 on day 1 followed by 5-FU 400 mg/m2 bolus on day 1 and 2,400 mg/m2 46-hour continuous infusion biweekly) or gemcitabine (1,000 mg/m2 weekly for 7 weeks followed by 1 week off, and then weekly for 3 weeks of every 4 weeks). The treatment of combination regimen versus gemcitabine showed statistically significant improvement in response rate (27.6% versus 10.9%; P=0.0008) as well as longer median overall survival (10.5 months versus 6.9 months; HR: 0.61; P<0.001) and 1-year survival (48.4% vs. 20.6%; P value not provided). Patients treated with combination regimen experienced higher incidence of grade 3 or 4 toxicities: neutropenia, fatigue, nausea, vomiting, and diarrhea.
The AIO trial conducted in Germany compared capecitabine-erlotinib to standard of care (Abstract LBA4011) [8]. Two-hundreds and seventy-nine patients were randomly assigned to arm A and arm B. Patients in arm A were treated with capecitabine (2,000 mg/m2/day, days 1-14, every 3 weeks) plus erlotinib (150 mg/day) as first-line and cross-over to gemcitabine alone as second-line if patients fail to firstline. Patients in arm B were treated with gemcitabineerlotinib standard regimen as first-line and cross-over to capecitabine alone if patients fail to first-line. The primary end point was time to treatment failure of second-line therapy (TTF2), and secondary end point was overall survival. No statistically significant differences were found for TTF2 and overall survival between the two groups. In subgroup analysis, patients with K-ras wildtype had a significant improvement in overall survival (wildtype 8.0 months versus mutation 6.6 months; HR: 1.62; P=0.011).
Phase II studies
The TARGET study, conducted in United Kingdom, combined the inhibition of both vascular endothelial growth factor (VEGF) and EGFR pathway as treatment strategy (Abstract #4036) [9]. Forty-four patients who had locally advanced disease (20 patients) or metastatic disease (24 patients) received gemcitabine (1,000 mg/m2 weekly for 3 weeks), capecitabine (1,400 mg/m2/day, days 1-21), bevacizumab (5 mg/kg days 1 and 15), and erlotinib (100 mg/day) every 28-day cycle. Patients with metastatic disease had an improved overall survival (11.1 months) and 1-year survival (49%) compared with historical data of standard therapy. Patients experienced grade 3 or 4 neutropenia (21%) and lethargy (14%).
The GEMSAP trial is a Japanese study to compare the activities of gemcitabine plus S-1 combination and gemcitabine alone (Abstract #4037) [10]. S-1 is an oral fluorinated pyrimidine developed in Japan, which is 5- chloro-2,4-dihydroxypyridine and potassium oxonate combined with tegafur, a prodrug of 5-FU. The biochemical combination can enhance and prolong the 5-FU antitumor activity. The primary end point was progression free survival. One-hundred and six patients were randomized to receive gemcitabine (1,000 mg/m2 infused over 30 minutes, days 1 and 15) plus S-1 (40 mg/m2 bid days 1-14 every 28 days) versus gemcitabine (1,000 mg/m2 infused over 30 minutes days 1, 8 and 15 every 28 days). A trend of longer median overall survival was observed in S-1 combination regimen (14.1 months versus 8.7 months; HR: 0.69; P=0.105), as well as 1-year survival rate (50.1% versus 32.0%; P value not provided). Gemcitabine plus S-1 regimen demonstrated significant longer median progression free survival than gemcitabine alone (5.4 months versus 3.6 months; HR: 0.64; P=0.036). The most common grade 3 or 4 toxicities in both group was neutropenia.
Discussion
The results of the PRODIGE 4/ACCORD 11 trial may represent a start of a paradigm shift in the management of advanced pancreatic cancer. Single agent gemcitabine has been the mainstay in the treatment of the disease and gemcitabine based combination therapies, with the exception of gemcitabine/erlotinib, have failed to show improvement in overall survival in randomized clinical trials. The 10-month overall survival seen with a non gemcitabine containing regimen, FOLFIRINOX, is the longest ever reported in the metastatic setting. However, caution should be exercised before considering FOLFIRINOX the new standard of care in this disease; the toxicity profile associated with the 3-drug regimen will limit its use to patients with good performance status.
Focus and resources should be directed towards identifying which patients are likely to benefit from a particular drug or regimen. The subgroup analysis in AIO trial highlighted the values of optimal patient selection and individualized medicine. Patients with K Kras wildtype had a significant improvement in overall survival. K-ras status is an important factor in personalized medicine in colorectal cancer, and we now have evidence that pharmacogenomics can play the same role in pancreatic cancer. This is even more important as we continue to evaluate the efficacy of combined inhibition of VEGF and EGFR pathways in the treatment of the disease. The potential cost of the combined inhibition could be prohibitive unless we target these likely to benefit patients.
The phase II trials of TARGET and GEMSAP show promising results, and warrant phase III studies to show a statistically significant improvement in survival.
Can we improve on the results seen with single agent gemcitabine in first line treatment of advanced pancreatic cancer? Studies presented at the ASCO Annual Meeting this year tell us that the answer is yes, but patient factors should be carefully considered when selecting the optimal therapy. More studies are needed to confirm the efficacy and safety of non gemcitabine containing regimens and to examine the association between K-ras mutation and tumor response. Eligible patients should be encouraged to participate in clinical trials.
Conflict of interest Authors report no conflict of interest
References
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer
Statistics, 2009. CA Cancer J Clin 2009; 59:225-49. [PMID
19474385]
- National Cancer Institute. Pancreatic Cancer Treatment (PDQ®).
Health Professional Version. Bethesda, MD, USA. (Accessed: June
12, 2010).
- Evans DB, Abbruzzese JL, Willett CG. Cancer of the pancreas.
In: DeVita VT, Hellman S, Rosenberg SA (editors). Cancer:
Principles and Practice of Oncology. 6th ed. Vol. 1. Philadelphia:
Lippincott, Williams & Wilkins; 1997. p. 1126-61. [ISBN 0-7817-
7207-9]
- Burris HA 3rd, Moore MJ, Andersen J, Green MR, Rothenberg
ML, Modiano MR, et al. Improvements in survival and clinical
benefit with gemcitabine as first-line therapy for patients with
advanced pancreas cancer: a randomized trial. J Clin Oncol 1997;
15:2403-13. [PMID 9196156]
- Stathis A, Moore MJ. Advanced pancreatic carcinoma: current
treatment and future challenges. Nat Rev Clin Oncol 2010; 7:163-72.
[PMID 20101258]
- Moore MJ, Goldstein D, Hamm J, Figer A, Hecht JR, Gallinger
S, et al. Erlotinib plus gemcitabine compared with gemcitabine alone
in patients with advanced pancreatic cancer: a phase III trial of the
National Cancer Institute of Canada Clinical Trials Group. J Clin
Oncol 2007; 25:1960-6. [PMID 17452677]
- Conroy T, Desseigne F, Ychou M, Ducreux M, Bouche O,
Guimbaud R, et al. Randomized phase III trial comparing
FOLFIRINOX (F: 5FU/leucovorin [LV], irinotecan [I], and
oxaliplatin [O]) versus gemcitabine (G) as first-line treatment for
metastatic pancreatic adenocarcinoma (MPA): Preplanned interim
analysis results of the PRODIGE 4/ACCORD 11 trial. J Clin Oncol
2010; 28(15 Suppl):4010.
- Boeck SH, Vehling-Kaiser U, Waldschmidt D, Kettner E,
Märten A, Winkelmann C, et al. Gemcitabine plus erlotinib (GE) followed by capecitabine (C) versus capecitabine plus erlotinib (CE)
followed by gemcitabine (G) in advanced pancreatic cancer (APC):
A randomized, cross-over phase III trial of the Arbeitsgemeinschaft
Internistische Onkologie (AIO). J Clin Oncol 2010; 28(18
Suppl):LBA4011.
- Watkins DJ, Starling N, Chau I, Thomas J, Webb J, Oates JR, et
al. The combination of a chemotherapy doublet (gemcitabine plus
capecitabine) with a biologic doublet (bevacizumab plus erlotinib) in
patients with advanced pancreatic adenocarcinoma: The TARGET
study. J Clin Oncol 2010; 28(15 Suppl):4036.
- Nakai Y, Isayama H, Sasaki T, Sasahira N, Hirano K, Tsujino T,
et al. A multicenter randomized controlled trial of gemcitabine (G)
alone versus gemcitabine and S-1 combination therapy (GS) in
patients with unresectable advanced pancreatic cancer (PC):
GEMSAP study. J Clin Oncol 2010; 28(15 Suppl):4037.

