Vasilis S Ramfidis1, Amanda Psyrri1, Kostas N Syrigos2, Muhammad Wasif Saif3
1Oncology Unit, Second Department of Medicine, Attikon University Hospital. Athens, Greece
2Oncology Unit, Third Department of Medicine, University of Athens, Sotiria General Hospital. Athens, Greece
3Department of Medicine and Cancer Center, Tufts Medical Center. Boston, MA, USA
- *Corresponding Author:
- Muhammad Wasif Saif
Department of Medicine and Cancer Center
Tufts Medical Center
800 Washington
Street Box 245
Boston, MA 02111
USA
Phone +1.617.636.8077
Fax +1.617.636.7060
E-mail wsaif@tuftsmedicalcenter.org
Keywords
Antineoplastic Agents; Drug Therapy; Pancreatic Neoplasms
What Did We Know Before the 2014 American Society of Clinical Oncology (ASCO) Annual Meeting?
Pancreatic cancer is a lethal disease and despite the progress that has been achieved the last years, its prognosis remains poor. More than 50% of patients have locally advanced or metastatic disease at the time of initial diagnosis and the five-year relative survival rate is approximately 2% [1, 2].
The therapeutic approach of patients with pancreatic adenocarcinoma in the first line setting is based in combination chemotherapy when Eastern Cooperative Oncology group (ECOG) performance status allows it. Results from the randomized phase III PRODIGE trial evaluating FOLFIRINOX versus gemcitabine showed significant superiority of the combination, but with considerable toxicity [3]. Gemcitabine-based combinations with albumin-bound paclitaxel, 5FU, erlotinib, capecitabine or cisplatin are also acceptable treatment options but clinical benefit remains modest [4-8].
What Have We Learnt from the 2014 American Society of Clinical Oncology (ASCO) Annual Meeting?
In this year’s ASCO Annual Meeting, four remarkable abstracts about advanced or metastatic pancreatic cancer were presented concerning first line treatment. The purpose of this paper is to dispose the data and the main findings of these studies as shown collectively in Table 1. The incorporation of the new data on a patient approach algorithm is illustrated in Figure 1.
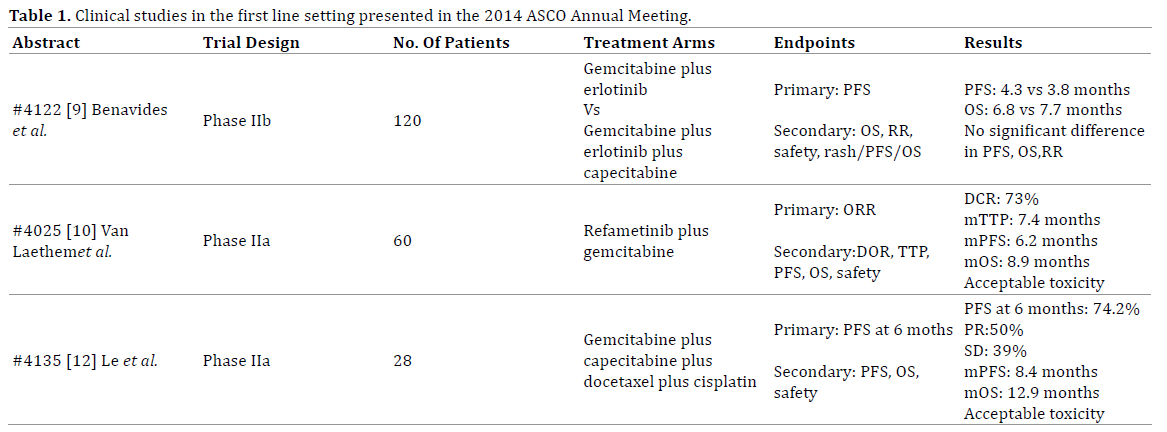
Figure 1. Therapeutic strategies in first line setting of advanced or metastatic pancreatic adenocarcinoma.
Gemcitabine and Erlotinib plus Capecitabine in the First Line Setting
Benavides et al. (Abstract #4122) conducted a phase IIb randomized trial in the first line setting in chemonaïve patients with advanced or metastatic pancreatic adenocarcinoma [9]. The 120 enrolled patients were equally randomized to receive gemcitabine plus erlotinib or Gemcitabine plus Erlotinib plus Capecitabine. The primary endpoint was PFS and the study didn’t achieve to show statistically significant difference between the two arms. Concerning the secondary endpoints, overall survival (OS) and response rate (RR) also failed to show significant difference. Patients who experienced skin rash demonstrated better PFS and OS and toxicity profile was more severe in the triplet arm.
Refametinib (a MEK1/2 Inhibitor) plus Gemcitabine and Their Role in the First Line Setting
MEK has been suggested as pivotal pathway for malignant progression in pancreatic cancer [10]. Refametinib, an allosteric dual MEK1/2 inhibitor, seem to have a role in the management of pancreatic cancer according to a single-arm, open-label, phase IIa study by Van Laethem et al. A total of 60 patients were recruited and received both rafametinib and gemcitabine as first line treatment [11]. Best overall response was partial response in 35% and stable disease in 38%. Disease control rate (DCR) was 73%, time to progression (TTP) was 7.4 months, median PFS was 6.2 months and OS 8.9 months. The subgroup of KRAS wild type population has significant better ORR and longer median PFS and OS. The toxicity profile of the combination was acceptable and manageable.
Multi-Agent Chemotherapy with Four Drugs in The First Line Treatment
A single arm phase II study examined the clinical activity of four therapeutic regimens in the first line setting [12]. The 28 patients that participated in the trial received low dose of capecitabine, gemcitabine, docetaxel and cisplatin. The primary endpoint of PFS at 6 months was 74.2%. The median PFS was 8.4 months, the OS 12.9 months and the disease control rate (DCR) was 89% with manageable toxicity.
Predictive Value of a Biomarker Panel Testing Response to Gemcitabine With or Without the Addition of Erlotinib
The addition of erlotinib to gemcitabine has shown statistically significant benefit in OS. At the NCIC Clinical Trials Group PA.3 study plasma samples were examined before receiving either monotherapy with gemcitabine or gemcitabine plus erlotinib. The 483 available samples showed on one hand that lower levels of IL-8 were correlated with longer OS if treated only with gemcitabine and on the other patients with lower levels of IL-8, CEA and HIF-1 alpha seem to benefit more if receiving both gemcitabine and erlotinib [13].
Discussion
Looking back few years ago, our therapeutic options in the first line setting in pancreatic cancer were limited. The recent years, clinical research revealed new treatment strategies that were added to our therapeutic quiver. Nevertheless, the prognosis of advanced or metastatic pancreatic cancer remains dismal and the need of newer more active approaches is imperative.
In this year ASCO Annual Meeting, two studies examined the efficacy of a triplet combination and a four-regimen combination. The first one of gemcitabine plus erlotinib plus capecitabine showed no significant clinical benefit compared to gemcitabine plus erlotinib alone. The second one examined the efficacy of capecitabine plus gemcitabine plus docetaxel plus cisplatin. Although it was a small trial, the results showed that this treatment strategy might be clinically active and these results remain to be examined in larger studies.
MEK pathway seems to play a role in carcinogenesis of pancreatic cancer but MEK inhibitors are still looking for their role in the therapeutic algorithm. Refametinib, a MEK 1/2 inhibitor, that was presented in this year ASCO Meeting in combination with gemcitabine showed remarkable clinical activity and especially in the subgroup with KRAS wild-type status. These results could help further the understanding of molecular biology of pancreatic cancer. Molecular alterations have not yet been elucidated in pancreatic cancer and these kinds of trials are useful research tools.
Finally, the development of drug strategies demands the presence of biomarkers with prognostic and predictive value. The last presenting abstract of this paper revealed the potential predictive value of plasma IL-8, CEA and HIF-1 alpha in patients that received gemcitabine plus erlotinib. Tailoring therapies to individual tumor and patient characteristics based on predictive biomarkers could change the therapeutic landscape of pancreatic cancer in the future.
Conflict of Interest
The authors have no conflicts to disclose.
References
- Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin. 2014; 64(1):9-29.
- SEER Cancer Statistics Review. Surveillance, Epidemiology, and End Results Program, 2013.
- Conroy T, Desseigne F, Ychou M, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011; 364:1817-1825. [PMID:21561347]
- Von Hoff DD, Ramanathan RK, Borad MJ, Laheru DA, Smith LS, Wood TE, Korn RL, et al. Gemcitabine Plus nab-Paclitaxel Is an Active Regimen in Patients With Advanced Pancreatic Cancer: A Phase I/II Trial. J ClinOncol. 2011; 29: 4548-4554. [PMID:21969517]
- Berlin JD, Catalano P, Thomas JP, Kugler JW, Haller DG, Benson AB 3rd., et al. Phase III study of gemcitabine in combination with fluorouracil versus gemcitabine alone in patients with advanced pancreatic carcinoma: Eastern Cooperative Oncology Group Trial E2297. J ClinOncol. 2002; 20:3 270-3275. [PMID:12149301]
- Moore MJ, Goldstein D, Hamm J, Figer A, Hecht JR, Gallinger S, Au HJ, et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: a phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J ClinOncol. 2007; 25:1960-1966. [PMID:17452677]
- Oliver GR, Sugar E, Laheru D, Diaz LA. Family history of cancer and sensitivity to platinum chemotherapy in pancreatic adenocarcinoma [abstract] . Gastrointestinal Cancers Symposium 2010:180.
- Neoptolemos JP, Stocken DD, Friess H, Bassi C, Dunn JA, Hickey H, Beger H, et al. A randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancer. N Engl J Med. 2004; 350: 1200-1210. [PMID:15028824]
- Benavides M, Plazas JG, Guillen C, Vera R, Iranzo V, Diaz IA, et al. Gemcitabine(G)/erlotinib(E) versus gemcitabine/ erlotinib/ capecitabine(C) in the first-line treatment of patients with metastatic pancreatic cancer (mPC): Efficacy and safety results of a phase IIb randomized study from the Spanish TTD Collaborative Group. J ClinOncol. 32:5s, 2014; (suppl; abstr 4122).
- Diep CH, Munoz RM, Choudhary A, Von Hoff DD, Han H. Synergistic effect between erlotinib and MEK inhibitors in KRAS wild-type human pancreatic cancer cells. Clin Cancer Res. 2011; 17(9):2744-56. [PMID:21385921]
- Van Laethem JL, Jassem J, Heinemann V, Weekes CD, Bridgewater JA, Cascinu S, et al. Phase II study of refametinib (BAY 86-9766), an allosteric dual MEK 1/2 inhibitor, and gemcitabine in patients with unresectable, locally advanced, or metastatic pancreatic cancer. J ClinOncol. 32:5s, 2014; (suppl; abstr 4025).
- Le DT, Laheru DA, Purtell K, Uram JN, Wang H, Lawrence S, et al. A phase 2 trial of low-dose multiagent chemotherapy with gemcitabine, docetaxel, capecitabine, and cisplatin (GTX-C) in subjects with metastatic pancreatic cancer. J ClinOncol. 32:5s, 2014; (suppl; abstr 4135).
- Shultz D, Pai J, Graber MS, Heestand GM, Chang DT, ParulekarWr, et al. A novel biomarker panel examining response to gemcitabine (G) with or without erlotinib (E) for pancreatic cancer (PA) therapy in NCIC clinical trials group PA.3. J ClinOncol. 32:5s, 2014; (suppl; abstr 4133).


