Keywords
130-nm albumin-bound paclitaxel; CA-19-9 Antigen; oxaliplatin; Pancreatic Neoplasms
Pancreatic cancer remains a deadly disease with an estimated 45,000 new cases in 2013 and nearly 38,500 deaths [1].
Gemcitabine has long been the agent of choice for locally advanced or metastatic pancreatic cancer [2]. In the last few years FOLFIRINOX (oxaliplatin, irinotecan, fluorouracil, and leucovorin) has emerged as the combination of choice for those patients with good performance status [3]. However, with a median age at diagnosis in the 70s there are a number of patients who are deemed inappropriate for this aggressive and often toxic therapy. Research in the field continues to push for new, novel combinations to provide a better benefit for patients without significant toxicity.
This year at the American Society of Clinical Oncology (ASCO) Annual Meeting the big news was MPACT, a phase III trial evaluating weekly nabpaclitaxel (abraxane) plus gemcitabine versus gemcitabine alone for patients with metastatic adenocarcinoma. Here we will discuss three abstracts relating to this trial (Abstracts #4005, #4058, and #4059).
What We Learned at the 2013 American Society of Clinical Oncology (ASCO) Annual Meeting
Results of a Randomized Phase III Trial (MPACT) of Weekly Nab-Paclitaxel Plus Gemcitabine Versus Gemcitabine Alone for Patients with Metastatic Adenocarcinoma of the Pancreas with PET and CA 19-9 Correlates (Abstract #4005 [4]).
Nab-paclitaxel (albumin-bound paclitaxel) is currently FDA-approved for use in metastatic breast cancer as well as locally advanced or metastatic non-small cell lung cancer. In pre-clinical models it has demonstrated activity in pancreatic cancer.
Emerging data has suggested that poor drug delivery is one of the key reasons why the currently available treatments for pancreatic cancer have failed [5] and there have been suggestions that nabpaclitaxel may aid in drug delivery.
A phase I/II trial of nab-paclitaxel plus gemcitabine published in 2011 found the combination to have tolerable adverse effects with substantial tumor activity [6]. The response rate was an outstanding 48% with a median 12.2 month overall survival. The laboratory correlate revealed decreased CA 19-9 levels corresponding to increases in response rate and survival. Secreted protein acidic and rich in cysteine (SPARC) in the stroma also corresponded with improved survival. SPARC, which is expressed and secreted by pancreatic fibroblasts, may act as an albumin binding protein and serve as a docking station for nab-paclitaxel, allowing for high intratumoral concentrations of the drug [7].
This study also included a murine xenograft correlate with human pancreatic cancer cells implanted into mice. The mice were treated with nab-paclitaxel alone and in combination with gemcitabine; in both cases the desmoplastic stroma was depleted.
Mice were also treated with gemcitabine alone or in combination with nab-paclitaxel. Those mice receiving combination therapy had an almost threefold increase in intra-tumoral concentration of gemcitabine, suggesting that by disrupting the stroma nab-paclitaxel is able to increase perfusion and drug delivery [6].
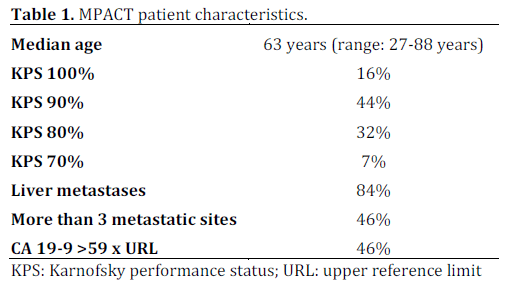
With positive results from the phase I/II trial, the authors proceeded with a phase III evaluation of the combination. The trial took place in 151 academic and community practices in five countries (Australia, Canada, Italy, Spain and the US). Patients were randomized in a 1:1 fashion to gemcitabine alone or gemcitabine in combination with nabpaclitaxel (Figure 1). Eight-hundreds and sixty-one patients with metastatic pancreatic cancer and a Karnofsky performance status (KPS) of 70 or more were randomized. The primary end point of the study was overall survival with secondary end points of progression free survival and overall response rate.
Figure 1. MPACT control and experimental arms.
The median age of patients was 63 years with the majority having a KPS of 80% or 90%. Over 80% of patients had liver metastasis (Table 1). The combination of nab-paclitaxel and gemcitabine was superior to gemcitabine alone at all of the end points. The mean duration of treatment was 3.9 months for combination and 2.8 months for gemcitabine alone (Figure 2).
Metabolic responses assessed by PET in 257 patients (29.8%) were 63% for the combination arm and 38% for gemcitabine alone (P=0.000051). CA 19-9 response (defined as a more than 90% decrease) was 31% for combination and 14% for gemcitabine alone (P<0.0001).
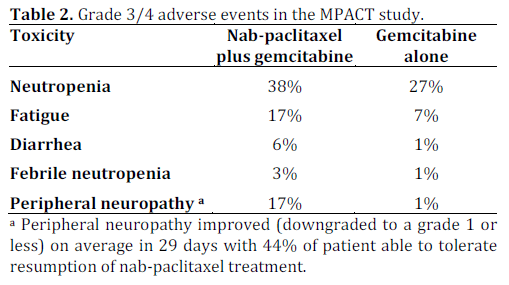
The toxicity profile, not surprisingly, reveals more side effects in the combination arm. Neutropenia, diarrhea and neuropathy were the most common side effects (Table 2).
The authors conclude that the combination of nab-paclitaxel and gemcitabine is tolerable in addition to being superior to gemcitabine alone. They consider this combination to be a new standard for treatment of metastatic pancreatic cancer.
CA 19-9 Decrease at 8 Weeks as a Predictor of Overall Survival (OS) in a Randomized Phase III Trial (MPACT) of Weekly Nab-Paclitaxel (nab-P) Plus Gemcitabine (G) Versus G Alone in Patients with Metastatic Pancreatic Cancer (MPC) (Abstract #4058 [8])
Authors involved in the MPACT trial presented results from a pre-specified exploratory analysis of CA 19-9. CA 19-9 was evaluated at baseline and then every 8 weeks while on study. The authors chose two numerical cut-offs for comparison: those patients with a decrease in CA 19-9 of 20% or more and then ultra-responders who had a decrease in CA 19-9 of more than 90%. More patients in the experimental arm experienced CA 19-9 responses. Patients who achieved a CA 19-9 decrease at 8 weeks in either category had an improved overall survival when treated with nab-paclitaxel plus gemcitabine compared to those patients who received gemcitabine alone.
Prognostic Factors (PFs) of Survival in a Randomized Phase III Trial (MPACT) of Weekly Nab-Paclitaxel (nab-P) Plus Gemcitabine (G) versus G Alone in Patients (pts) with Metastatic Pancreatic Cancer (MPC) (Abstract #4059 [9])
Again authors involved in the MPACT trial assessed potential prognostic factors that correlate with improved overall survival.
Using a stepwise multivariate analysis they identified region of Eastern Europe, age greater than 65 years, poorer performance status, presence of liver metastases and number of metastatic sites all predicted for an increased risk of death. After correction for these factors assignment to nabpaclitaxel plus gemcitabine was an independent significant predictor of improved survival.
DISCUSSION
The landscape of treatment for metastatic pancreatic cancer did not change much from 1997 when gemcitabine was improved to 2011 when researchers made headlines using FOLFIRINOX. Now just two years later there is another new active combination.
FOLFIRINOX provided a median survival of 11.1 months compared to 6.8 months in gemcitabine treated patients in a pivotal phase II/III trial published in 2011 [3]. This marked a significant improvement in survival in a disease with a quite dismal prognosis; however, this just over 3-month improvement came with some toxicity.
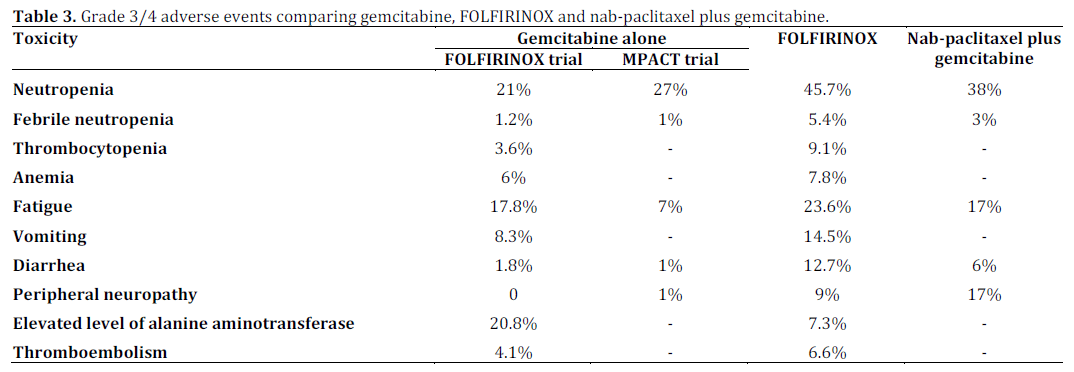
The combination of nab-paclitaxel and gemcitabine has more toxicity than gemcitabine alone but less toxicity than the FOLFIRINOX regimen (Table 3). The major differences are more frequent grade 3 or 4 anemia, thrombocytopenia, vomiting and worsened fatigue with FOLFIRINOX. Peripheral sensory neuropathy was worse with the nab-paclitaxel containing regimen, but as they noted in the trial seemed to diminish quickly. Almost half of the patients who came off therapy for neuropathy were able to resume treatments.
A comparison of overall survival reveals a similar overall survival for gemcitabine in both trials (6.7 and 6.8 months). The current study achieved an overall survival of 8.5 months with nabpaclitaxel and gemcitabine; however, the FOLFIRINOX trial reached 11.1 months, an impressive standard in metastatic pancreatic cancer. Gemcitabine plus erlotinib is another active combination that showed modest improvement over gemcitabine alone.
With the results from MPACT, oncologists now have three combinations and one single agent regimen for treating patients with metastatic pancreatic cancer. While the outlook for the patients with metastatic pancreatic cancer is not good, it has certainly improved over the last 2-3 years. The challenge for physicians will be in deciding which patients should receive which treatments. Those patients with poorer performance status will likely be offered single agent gemcitabine therapy, while those with better performance status will receive one of the two very active combinations. Patients with a KPS of 90-100 (without any obvious contraindications) are likely to receive the most aggressive therapy, FOLFIRINOX that also provides the best median survival. Patients with slightly depressed KPS maybe be offered the nab-paclitaxel-gemcitabine combination in hopes of providing better tumor control without a significant increase in toxicity.
Conflict of interest
The authors have no potential conflict of interest
References
- Cancer Facts and Figures 2013. American Cancer Society
- Burris HA, et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: a randomized trial. J Clin Oncol 15:2403-13, 1997.
- Conroy T, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med 364:1817-25, 2011.
- Von Hoff DD, Ervin TJ, Arena FP, Chiorean EG, Infante JR, Moore MJ, et al. Results of a randomized phase III trial (MPACT) of weekly nab-paclitaxel plus gemcitabine versus gemcitabine alone for patients with metastatic adenocarcinoma of the pancreas with PET and CA19-9 correlates. J Clin Oncol 31, 2013(Suppl): Abstract #4005.
- Komar G, et al. Decreased blood flow with increased metabolic activity: a novel sign of pancreatic tumor aggressiveness. Clin Cancer Res 2009; 15:5511-7.
- Von Hoff D, et al. Gemcitabine Plus nab-Paclitaxel Is an Active Regimen in Patients With Advanced Pancreatic Cancer: A Phase I/II Trial. JCO 2011;29:4548-4554.
- Frese K, et al. nab-Paclitaxel Potentiates Gemcitabine Activity by Reducing Cytidine Deaminase Levels in a Mouse Model of Pancreatic Cancer. Cancer Discovery 2012; 261-269.
- Chiorean EG, Von Hoff DD, Ervin TJ, Arena FP, Infante JR, Bathini VG, et al. CA 19-9 decrease at 8 weeks as a predictor of overall survival (OS) in a randomized phase III trial (MPACT) of weekly nab-paclitaxel (nab-P) plus gemcitabine (G) versus G alone in patients with metastatic pancreatic cancer (MPC). J Clin Oncol 31, 2013(Suppl): Abstract #4058.
- Moore MJ, Von Hoff DD, Ervin TJArena FP, Chiorean EG, Infante JR, et al. Prognostic factors (PFs) of survival in a randomized phase III trial (MPACT) of weekly nab-paclitaxel (nab-P) plus gemcitabine (G) versus G alone in patients (pts) with metastatic pancreatic cancer (MPC). J Clin Oncol 31, 2013(Suppl): Abstract #4059.



