Keywords
Pancreatic Neoplasms
INTRODUCTION
Intraductal Pancreatic Mucinous Neoplasms (IPMNs) represent approximately 1% of invasive pancreatic neoplasms and 24% of pancreatic cystic neoplasms. In contemporary surgical series, IPMN accounts for 8% to 20% of pancreatic resections [1,2]. Despite advancement in understanding the natural history and molecular mechanisms involved in the neoplastic progression of IPMN, several aspects of clinical management continue to be poorly defined. We sought to review the surgical literature for a better understanding of trends in intra and postoperative management of the pancreatic remnant following surgical resections performed for IPMN.
Histologic Classification
The World Health Organization classifies IPMN histologically into four successive stages: mild dysplasia (IPMN adenoma), moderate dysplasia (IPMN borderline), severe dysplasia (IPMN carcinoma in situ), and invasive carcinoma [3-5].
Risk factors for malignancy
Based on location, IPMN can be distinguished as mainduct IPMN, branch-duct IPMN, and mixed type involving both the main-duct and branch-duct. Main-duct IPMNs harbor a five-year actuarial risk of malignancy of 60% (range: 11% to 81%). Branch-duct IPMNs have a risk of malignant transformation of approximately 26% (range: 6% to 47%) [6-8]. Mixed IPMNs have a risk of malignant transformation between 35% to 40% [9].
SURGICAL MANAGEMENT
According to the International Consensus Guidelines for the management of IPMNs released in 2012, all high-risk main-duct or mixed IPMNs should be resected due to high incidence of malignant transformation if the patient is a surgical candidate [6]. Management of branch-duct IPMNs is more controversial due to the lower risk of malignant transformation. In the development of the treatment algorithm of branch-duct IPMNs different factors were taken into account such as cyst size, patient symptoms (abdominal pain, pancreatitis, jaundice and constitutional symptoms for cancer), and high-risk features (mural nodules, rapidly increasing cyst size, high-grade atypia). Resection is recommended in patients with IPMN ranging from one cm to three cm in the presence of symptoms or high risk-features (mural nodules with a blood flow signal confirmed by contrast enhanced endoscopic ultrasounds and exclusion of mucous clots, rapidly increasing cyst size of more than two mm/yr, high-grade dysplasia) [6,10,11]. Resection can be recommended in patients with IPMNs greater than three cm based on size alone although size itself is a weaker indicator of malignancy than presence of some other high-risk features [6,12,13].
Types of Surgical Procedures
The surgical procedure of choice is based on the location of the lesion within the pancreas with additional consideration given to short-term and long-term implications related to surgery. Total pancreatectomy, classic pancreaticoduodenectomy, pylorus preserving pancreaticoduodenectomy, central pancreatectomy, distal pancreatectomy with splenectomy, spleen preserving distal pancreatectomy, and enucleation have all been described and widely utilized [1,14-19].
Interpretation and Management of Positive Pancreatic Resection Margins
Currently, there are no clear guidelines for the management of pancreatic transection margins following resections for high risk IPMN. The risk of recurrent IPMN in the pancreatic remnant has to be balanced against the long-term side effects of extensive pancreatectomies and finding this balance can be difficult, especially in an aging population with increasing co-morbidities. Positive margins following IPMN resection can be classified into positive margins with mild to moderate dysplasia (non-invasive IPMN), positive margins with high-grade dysplasia or carcinoma in situ (non-invasive IPMN) and positive margin with invasive carcinoma. However, the definition of positive margin varies amongst different authors [20-23].
Unfortunately, the majority of the studies available combine patients with primary noninvasive IPMN (term that encompasses a wide range of histologies from mild dysplasia to carcinoma in situ) and invasive IPMN making it difficult to draw conclusions for the management of positive margins. In addition, patients with branch-duct versus main-duct IPMN are also usually lumped together making it challenging to compare rates of margin positivity and recurrences between two disease entities with clearly different risk of malignancy.
Positive Margins with Non-Invasive IPMN
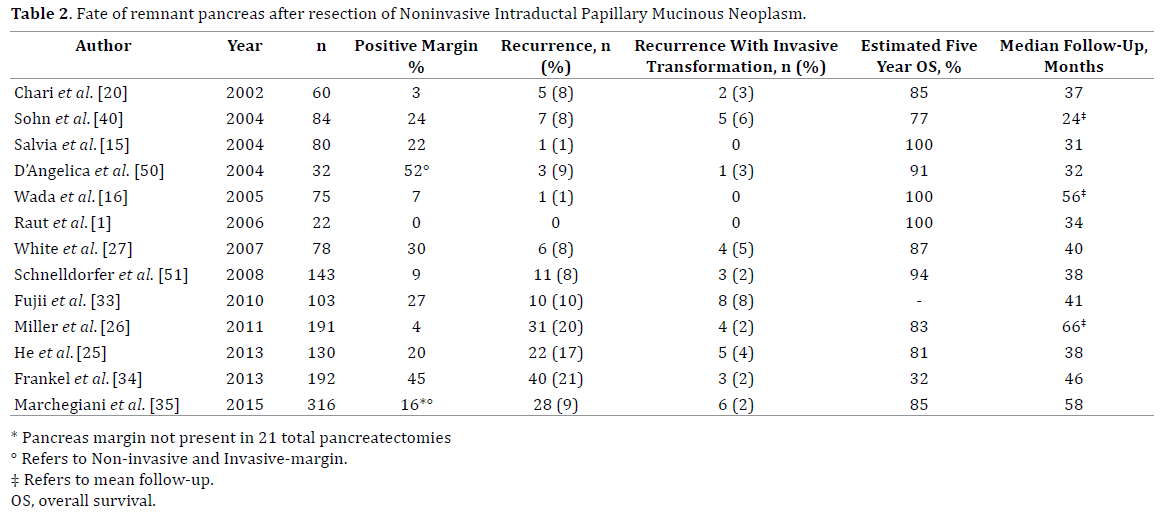
Tanaka et al. reported that positive margins for resected adenomas and borderline lesions more closely resembling adenomas (low-grade or moderate-grade dysplasia) do not warrant subsequent resection [24]. In a review of the literature done by Moriya et al. [17] which included nine studies totaling 1131 cases, 18% of individuals with some form of noninvasive IPMN had a positive resection margin. No correlation was found between positive margins following resection and development of a new lesion in the pancreatic remnant after median follow-up of 24 to 64 months. The authors concluded that pancreatic preservation should be a priority. The five-year overall survival rate following resection for non-invasive IPMN ranges between 77% to 100% [20,25-27].
In a study by White et al. [27] only one of 50 patients (2%) with margins negative for IPMN recurred versus four of 23 patients (17%) with margins positive for IPMN. Only two of the reported recurrences were clearly borderline or invasive recurrences.
He et al. [25] analyzed the fate of the remnant pancreas of 130 patients. Atypia or low-grade dysplasia was present in the resection margin of 26 (20%) patients of these patients 20% (6 of 30) had recurrence at a median of 38 months when compared to 16% (16 of 100) without IPMN at the margin that developed recurrence. In this study there was no correlation between margin status and risk of recurrence except for family history of pancreatic cancer independently predicting recurrence.
Positive Margins with Invasive IPMN
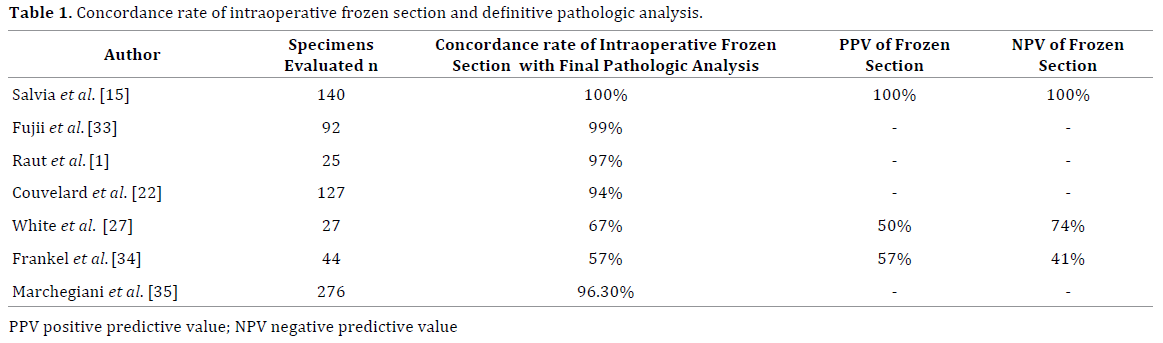
The management of surgical margins for invasive IPMN is less controversial given its higher risk of recurrence and poor five-year survival ranging from 40%-85% for node-negative invasive IPMN and 0-45% for nodepositive invasive IPMN. The lymph node positivity rates for invasive IPMN range between 33% and 54% in most recent studies. In a meta-analysis by Kai-Ming Leng et al. [28], 339 patients with invasive IPMNs were identified in 11 cohort studies. Recurrence after resection occurred in 39% of patients with margin-negative resection versus 54% with margin-positive resection (OR: 0.47; 95% CI: 0.25-0.88, p=0.020) suggesting that positive margins are relevant to the risk of recurrence in this setting. However, in a study by Schnelldorfer et al. [14] only 15% of those with recurrence had a positive operative margin at resection (5 patients: malignant positive, 4; benign positive, 1). In this same study, 46 patients who underwent partial pancreatectomy had a total recurrence rate of 54% and a distant recurrence rate of 39%. These recurrence rates were not significantly different when compared to the 11 patients in the same series who underwent total pancreatectomy and had a 73% overall recurrence rate and 73% distant recurrence rate. This finding is similar to other described series [14,15,20,29,30] and suggests that the pursuit of negative margins in patients with IPMNs may not significantly impact the patient’s risk of IPMN recurrence, suggesting a field defect. However many authors still advocate for negative margins (R0) when faced with a positive margin for invasive IPMN or in presence of diffuse pancreatic involvement with this premalignant condition [20,31,32]. Studies conducted to evaluate the concordance rate between intraoperative frozen sections and definitive pathological evaluation of pancreatic margins reported rates ranging between 57% and 99% (Table 1) [1,15,22,27,33,34]. Nevertheless, according to the International Consensus Guidelines, intraoperative frozen sections are useful to assess margin status and decide the extent of resection [6,22]. In the absence of other severe comorbidities, the presence of positive margins for high-grade dysplasia or invasive adenocarcinoma, should prompt additional pancreatic resections to achieve negative margins [35].
Risk of Recurrence
Following surgical resection, the pancreatic remnant has a persistent risk for metachronous or “recurrent” disease. Metachronous lesions represent new occurrence of IPMNs or pancreatic ductal adenocarcinoma that arise following prior complete resection of the initial pancreatic lesion [36]. Two types of recurrence can occur: metachronous multifocal occurrence of IPMNs in the remnant pancreas or metastatic or local recurrence of invasive carcinoma.
There is increasing evidence that some synchronous pancreatic lesions identified at the time of the original operation are genetically distinct entities from the target lesion [37]. It is reasonable to speculate that some of the metachronous lesions could represent de novo IPMNs or pancreatic ductal adenocarcinoma without any genetic relations with the original resected lesion.
Non-Invasive IPMN
A recent meta-analysis completed by Kai-Ming Leng et al. [28] reported that post-operative recurrence rate with non-invasive IPMNs was 4.9% over a follow up period of 24 to 65 months. Palaez-Luna et al. [38] found that up to 8% of patients with benign branch-duct IPMNs will have recurrence in the remnant pancreas (median follow-up of 15 months). White et al. [27] found a 7.7% local recurrence rate following resections for noninvasive IPMN at a median of 40 months follow-up. Recurrence histology was only known in three patients out of a total of six recurrences with only one patient having clearly invasive recurrence.
Based on these data, organ preservation should be a priority in the setting of surgical resections for non-invasive IPMN (Table 2). The possibly higher rates of recurrences in the pancreatic remnant do not justify an initially aggressive surgical resection with possible total pancreatectomy unless diffuse high-grade dysplasia is encountered.
Invasive IPMN
The aim of surgical intervention is a margin negative resection for high-grade dysplasia or invasive cancer in good-surgical risk patients diagnosed with invasive IPMN. This has to balance against the high risk of systemic recurrence in the setting of invasive IPMN resulting in poor survival (Table 3). When compared to node negative disease, in the presence of node positive disease, the driver of final outcome seems to be the development of extra pancreatic disease [15,39,40].

Utilizing the Surveillance, Epidemiology, and End Results Program, Wasif et al. [39] reported a five-year survival of 22% (median survival 21 months) that was highly influenced by the node status. In patients with nodenegative disease five-year survival was 35% for invasive IPMN (median survival 34 months).
Poultsides et al. [41] analyzed 312 patients with IPMN undergoing pancreatectomy. The authors found that invasive carcinoma arising in the setting of IPMN had a better outcome compared to standard pancreatic carcinoma with an overall median survival of 43 months versus 19 months and a five-year survival of 42% versus 19% (p<0.001). This significant survival difference persisted when comparing patients without nodal metastasis but disappeared in patients with nodal metastasis. Similar findings where reported by Schnelldorfer et al. [14].
Follow Up
Currently there is only limited evidenced-based data available to guide clinicians in the follow up of patients with pancreatic IPMN. The intervals at which imaging studies are obtained are highly influenced by the presence of residual macroscopic IPMN and microscopic margin status of the pancreatic remnant. In addition, patient age, family history, symptoms, comorbidities, perceived pancreatic cancer risk, and patient preferences all play an important role.
Surveillance after resection is critical considering that recurrence has been described to occur even 10 years after resection [35]. Residual IPMN can be left in place at the time of the planned surgical resection with relatively low risk of these lesions developing into lesions requiring a surgical resection later on, as long as they have low risk criteria [6]. Commonly this scenario is due to the presence of a branch-duct IPMN or multifocal branch-duct IPMNs that did not meet initial criteria for resection. A retrospective analysis by Moriya et al. [17] focused on residual lesions in the pancreatic remnant. They identified 31 patients with recurrences after a median follow up of 40 months. These lesions were either left in the remnant at the time of resections (14 patients) or identified by imaging during follow-up (new lesions). The authors noted that the 14 residual lesions were consistent with branch-duct-type IPMN that were less than three cm, none of these lesions changed in size or caused any symptoms.
Some studies also reported an increased risk of extrapancreatic malignancies (24-52%) that were identified prior, at the time or after the index surgery [14,42-46]. There are no existing guidelines for screening for possible secondary malignancies, although some data suggest that surveillance should be pursued.
Residual Not Resected IPMN
According to the most recent international consensus patients with residual (not resected) IPMN should be followed according to the presence or absence of “high risk stigmata” [6]. In patients without “high risk stigmata” a short interval (three to six months) pancreatic MRI/MRCP (or CT) should be obtained to establish the stability of the lesion. In stable lesions, following this initial assessment, subsequent imaging studies should be dictated by size stratifications. For lesions less than one cm a CT/MRI is obtained in two to three years. For lesions between one and two cm a CT/MRI is obtained yearly for two years and then at lengthened intervals if no change. Lesions between two and three cm should undergo EUS in three to six months, then lengthen interval alternating MRI with EUS as deemed appropriate by physician and patients. Lesions greater than three cm should undergo close surveillance every three to six months, alternating MRI/CT with EUS, however surgery should be considered in these patients if feasible. Recently, several reports identified a yearly risk of 0.7–0.9 % of pancreatic ductal adenocarcinoma arising from side branch IPMN [47]. These residual synchronous or metachronous IPMNs could represent genetically independent lesions and the same criteria for resectability and follow-up dictated by the International Consensus statement should apply [37]. Some authors continue to recommend serial follow up with CT or MRCP every six months.
Negative Margin Resections (Including Non Dysplastic Changes)
There are no clear guidelines on the type and frequency of follow-up studies [25,48]. Some authors are recommending CT/MRI every six-twelve months for an initial period of two years in the setting of resected non-invasive IPMN followed by a yearly surveillance thereafter.
Positive Margins of Resection for Low-Grade or Moderate-Grade Dysplasia
There are no definitive recommendations in the literature to guide the type or the intervals of imaging following resections of IPMN with positive margins for low or moderate dysplasia. The 2012 IAP suggests that history/ physical examination and CT/MRCP be performed twice a year for the first two to three years [6].
IPMN with Foci of Invasive Adenocarcinoma
This group of patients should be followed with a strategy identical to that currently in use for pancreatic ductal adenocarcinoma. Some authors recommend imaging every three months for two years for the detection of recurrent disease in the setting of invasive IPMN with decreasing the frequency of follow-up studies to every six months afterwards in the setting of resected invasive IPMN. Worrisome lesions developing in the pancreatic remnant during surveillance imaging should be assessed with EUS with or without sampling [6].
Type of Surgical Resection for Recurrent IPMN in the Pancreatic Remnant
Little to no data exist on the type and extent of secondary resections for patients with IPMN. Moriya et al. [17] described a total of five patients, three with completion pancreatectomy, one with mass excision from the body of pancreas, and one with unresectable disease. Histology evaluation following re-resections revealed two cases of invasive cancer, one carcinoma in situ and two cases with adenomas. Predictably, both patients with invasive disease had disease recurrence/persistence following second surgery with short survival.
The Mayo Clinic series described a total of three re-resections in a study with a mean follow-up of 3.2 years [14]. All three patients underwent completion pancreatectomy, with details on recurrent disease histology being reported in only one patient who was found to have recurrent adenoma. Only two repeat resections were performed in the study by Ohtsuka et al. [36], both being completion pancreatectomies. Both patients were originally operated on for high-risk main-duct IPMN and both were found to have non-invasive IPMN in the pancreatic remnant upon final histologic exam (Figure 1).

Figure 1. Recurrent main-duct IPMN following partial pancreatectomy. This series of images illustrate the clinical evolution of a main-duct Intraductal
Papillary Mucinous Neoplasm (IPMN) in a 66-year-old female who presented with multiple episodes of pancreatitis. (a.). Focal dilation of the pancreatic
duct in the head of the pancreas (thin arrowhead) with normal caliber duct in the body and tail. (b.). Pancreatoscopy: fish egg lesion (thin arrow) consistent with focal main-duct IPMN. The patient underwent an uncomplicated pancreaticoduodenectomy with negative resection margins (R0). Final pathology revealed a three cm main-duct IPMN with low-grade dysplasia in the pancreatic head. (c & d.). Routine follow-up computed tomography revealed
progressively worsening dilation of the main pancreatic duct (from four mm up to 25 mm) in the body (block arrowhead in the coronal plane) and tail
(block arrow in the axial plane). Three years after her original surgery she underwent an uncomplicated completion pancreatectomy. Final pathology
analysis revealed extensive high-grade dysplasia without any evidence of invasive cancer nor metastatic lymph nodes (0/36). The patient is currently
disease free at approximately 50 months following her initial partial pancreatectomy.
No clear recommendations can be made to guide the extent of surgical re-resections in the few patients who are candidates for reoperation for locally recurrent IPMN. All described patients above, except one, underwent a completion pancreatectomy, likely for concern of these recurrences representing a field defect.
Adjuvant Treatment Following Resection for Invasive IPMN
To our knowledge, few studies in the current surgical literature address the risks and benefits of adjuvant chemo and/or radiation therapy in the setting of resected invasive IPMN [1,49]. Only a limited number of studies ever compared the risk of local/systemic recurrence for patients with invasive IPMN versus pancreas ductal adenocarcinoma not arising from IPMN [14,39]. The risk of developing systemic disease seems to be high, with overall survival curves being quite poor in both disease entities (five-year survival 20-30%), especially for node positive disease.
Raut et al. [1] described six patients receiving postoperative adjuvant therapy for invasive IPMN and five patients receiving intraoperative radiotherapy. Histologic re-review determined that there was no invasive cancer in nearly half of these patients. No treatment details were described.
In the absence of better clinical evidence, administration of adjuvant treatment protocols used for invasive pancreas ductal adenocarcinoma seems reasonable for patients with invasive IPMN secondary to the high risk of systemic disease recurrence. However, the exact benefits of such treatment protocols remain questionable.
CONCLUSIONS AND FINAL RECOMMENDATIONS
Current knowledge of the natural history, management and prognosis of IPMN derives from retrospective series and is limited by small sample size and short follow-up. There are even less evidenced-based data available to guide clinicians in the management of the residual pancreas and its subsequent follow up. IPMNs meeting current guidelines for surgical resection should be completely removed, with appropriate lymph node dissection. Pancreatic transection margins should be assessed intraoperatively and further resection should be considered for cases of high-grade dysplasia or invasive cancer at the margins. Pancreas preservation should be a priority. Adenoma or low-grade dysplasia at the pancreatic transection margin does not affect long-term outcome and does not require further pancreatic resection in our opinion. The rate of systemic recurrence is high with invasive IPMN especially in the setting of node positive disease. The role of adjuvant therapy in the setting of resected invasive IPMN is unclear. Since node positive invasive IPMN has a high risk of systemic recurrence, administration of adjuvant therapy similar to pancreatic adenocarcinoma seems reasonable. Pancreatic remnants should be followed for concerns of developing new lesions with at least yearly pancreatic protocol computed tomography or magnetic resonance imaging. Lesions not meeting resection criteria in the remnant of the pancreas and intentionally left behind are less likely to progress during follow-up. The current recommendations in the evolving field of IPMN management are likely to change with larger clinical studies and longer follow-up as more detailed information becomes available on the natural history and recurrence pattern of IPMN lesions.
Conflict of Interest
Authors declare to have no conflict of interest
References
- Raut CP, Cleary KR, Staerkel GA, et al. Intraductal papillary mucinous neoplasms of the pancreas: effect of invasion and pancreatic margin status on recurrence and survival. Ann SurgOncol2006;13:582-594. [PMID: 16523362]
- Fritz S, Fernández-del Castillo C, Mino-Kenudson M, et al. Global Genomic Analysis of Intraductal Papillary Mucinous Neoplasms of the Pancreas Reveals Significant Molecular Differences Compared to Ductal Adenocarcinoma. Annals of surgery 2009;249:440-447. [PMID: 19247032]
- Adsay NV, Fukushima N, Furukuwa T, et al. "Intraductal neoplasm of the pancreas," in World Health Organization Classification of Tumours of the Digestive System, Bosman F, Carneiro F, Hruban R, Thiese N (Eds), 304-311, IARC Press, Lyon, France 2010.
- Kato Y, Kloppel G, Longnecker DS. An illustrated consensus on the classification of pancreatic intraepithelial neoplasia and intraductal papillary mucinous neoplasms.Amer J Surg2004. [PMID: 15252303]
- Furukawa T, Klöppel G, VolkanAdsay N, et al. Classification of types of intraductal papillary-mucinous neoplasm of the pancreas: a consensus study. Virchows Arch2005;447:794-799. [PMID: 16088402]
- Tanaka M, Castillo CF-D, Adsay V, et al. International consensus guidelines 2012 for the management of IPMN and MCN of the pancreas. Pancreatology2012;12:183-197. [PMID: 22687371]
- Khannoussi W, Vullierme MP, Rebours V, et al. The long term risk of malignancy in patients with branch duct intraductal papillary mucinous neoplasms of the pancreas.Pancreatology2012;12:198-202. [PMID: 22687372]
- Levy P, Barthet M, Mollard BR, Amouretti M, Marion-Audibert A-M, Dyard F. Estimation of the prevalence and incidence of chronic pancreatitis and its complications. GastroenterolClinBiol2006;30:838-844. [PMID: 16885867]
- Sahora K, Fernández-del Castillo C, Dong F, et al. Not all mixed-type intraductal papillary mucinous neoplasms behave like main-duct lesions: implications of minimal involvement of the main pancreatic duct. Surgery2014;156:611-621. [PMID: 25081232]
- Ohno E, Hirooka Y, Itoh A, et al. Intraductal papillary mucinous neoplasms of the pancreas: differentiation of malignant and benign tumors by endoscopic ultrasound findings of mural nodules. Annals of surgery2009. [PMID: 19300203]
- Kang MJ, JANG J, KIM SJ, et al. Cyst growth rate predicts malignancy in patients with branch duct intraductal papillary mucinous neoplasms. Clinical Gastroenterology and Hepatology2011;9:87-93. [PMID: 20851216]
- Jang J-Y, Kim S-W, Lee SE, et al. Treatment guidelines for branch duct type intraductal papillary mucinous neoplasms of the pancreas: when can we operate or observe? Ann SurgOncol2008;15:199-205. [PMID: 17909912]
- Weinberg BM, Spiegel BMR, Tomlinson JS, Farrell JJ. Asymptomatic pancreatic cystic neoplasms: maximizing survival and quality of life using Markov-based clinical nomograms. Gastroenterology2010;138:531-540. [PMID: 19818780]
- Schnelldorfer T, Sarr MG, Nagorney DM, et al. Experience with 208 resections for intraductal papillary mucinous neoplasm of the pancreas. Arch Surg2008;143:639-646. [PMID: 18645105]
- Salvia R, Fernández-del Castillo C, Bassi C, et al. Main-duct intraductal papillary mucinous neoplasms of the pancreas: clinical predictors of malignancy and long-term survival following resection. Annals of surgery2004;239:678-685. [PMID: 15082972]
- Wada K, Kozarek RA, Traverso WL. Outcomes following resection of invasive and noninvasive intraductal papillary mucinous neoplasms of the pancreas.Amer J Surg2005;189:632-636. [PMID: 15862510]
- Moriya T, Traverso W. Fate of the pancreatic remnant after resection for an intraductal papillary mucinous neoplasm: a longitudinal level II cohort study. Arch Surg2012;147:528-534. [PMID: 22351878]
- Crippa S, Boninsegna L, Partelli S, Falconi M. Parenchyma-sparing resections for pancreatic neoplasms. Journal of hepato-biliary-pancreatic sciences2010;17:782-787. [PMID: 22911124]
- Crippa S, Bassi C, Salvia R, Falconi M, Butturini G, Pederzoli P. Enucleation of pancreatic neoplasms. Br J Surg2007;94:1254-1259. [PMID: 17583892]
- Chari ST, Yadav D, Smyrk TC, et al. Study of recurrence after surgical resection of intraductal papillary mucinous neoplasm of the pancreas. Gastroenterology2002;123:1500-1507. [PMID: 12404225]
- Hruban RH, Adsay NV, Albores-Saavedra J, et al. Pancreatic intraepithelial neoplasia: a new nomenclature and classification system for pancreatic duct lesions. Am J SurgPathol2001;25:579-586. [PMID: 11342768]
- Couvelard A, Sauvanet A, Kianmanesh R, et al. Frozen sectioning of the pancreatic cut surface during resection of intraductal papillary mucinous neoplasms of the pancreas is useful and reliable: a prospective evaluation. Annals of surgery2005;242:774-778. [PMCID: 1409870]
- Eguchi H, Ishikawa O, Ohigashi H, et al. Role of intraoperative cytology combined with histology in detecting continuous and skip type intraductal cancer existence for intraductal papillary mucinous carcinoma of the pancreas. Cancer2006;107:2567-2575. [PMID: 17054109]
- Tanaka M, Chari S, Adsay V, et al. International consensus guidelines for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas. Pancreatology2006;6:17-32. [PMID: 16327281]
- He J, Cameron JL, Ahuja N, et al. Is It Necessary to Follow Patients after Resection of a Benign Pancreatic Intraductal Papillary Mucinous Neoplasm? Journal of the American College of Surgeons2013;216:657-665. [PMID: 23395158]
- Miller JR, Meyer JE, Waters JA, et al. Outcome of the pancreatic remnant following segmental pancreatectomy for non-invasive intraductal papillary mucinous neoplasm. HPB (Oxford)2011;13:759-766. [PMID: 21999588]
- White R, D'Angelica M, Katabi N, et al. Fate of the remnant pancreas after resection of noninvasive intraductal papillary mucinous neoplasm. Journal of the American College of Surgeons2007;204:987-993. [PMID: 17481526]
- 28.Leng K-M, Wang Z-D, Zhao J-B, Cui Y-F, Zhong X-Y. Impact of pancreatic margin status and lymph node metastases on recurrence after resection for invasive and noninvasive intraductal papillary mucinous neoplasms of the pancreas: a meta-analysis. Digestive surgery2012;29:213-225. [PMID: 22677789]
- Bassi C, Sarr MG, Lillemoe KD, Reber HA. Natural history of intraductal papillary mucinous neoplasms (IPMN): current evidence and implications for management. Journal of gastrointestinal surgery: official journal of the Society for Surgery of the Alimentary Tract2008;12:645-650. [PMID: 18097728]
- Levy P, Jouannaud V, O'Toole D, et al. Natural history of intraductal papillary mucinous tumors of the pancreas: actuarial risk of malignancy. ClinGastroenterolHepatol2006;4:460-468. [PMID: 16616351]
- 31.Stauffer JA, Nguyen JH, Heckman MG, et al. Patient outcomes after total pancreatectomy: a single centre contemporary experience. HPB2009;11:483-492. [PMID: 19816612]
- BendixHolme J, Jacobsen NO, Rokkjaer M, Kruse A. Total pancreatectomy in six patients with intraductal papillary mucinous tumour of the pancreas: the treatment of choice. HPB2001;3:257-262. [PMID: 18333027]
- Fujii T, Kato K, Kodera Y, et al. Prognostic impact of pancreatic margin status in the intraductal papillary mucinous neoplasms of the pancreas. Surgery2010;148:285-290. [PMID: 20434746]
- Frankel TL, LaFemina J, Bamboat ZM, et al. Dysplasia at the surgical margin is associated with recurrence after resection of non-invasive intraductal papillary mucinous neoplasms. HPB (Oxford) 2013: 15:814-821. [PMID: 23782351]
- Marchegiani G, Mino-Kenudson M, Ferrone CR, et al. Patterns of Recurrence After Resection of IPMN: Who, When, and How? Annals of surgery2015:1. [PMID: 25793719]
- Ohtsuka T, Kono H, Tanabe R, et al. Follow-up study after resection of intraductal papillary mucinous neoplasm of the pancreas; special references to the multifocal lesions and development of ductal carcinoma in the remnant pancreas. Amer J Surg2012;204:44-48. [PMID: 21996346]
- Matthaei H, Norris AL, Tsiatis AC, et al. Clinicopathological characteristics and molecular analyses of multifocal intraductal papillary mucinous neoplasms of the pancreas. Annals of surgery2012;255:326-333. [PMID: 22167000]
- Pelaez-Luna M, Chari ST, Smyrk TC, et al. Do consensus indications for resection in branch duct intraductal papillary mucinous neoplasm predict malignancy? A study of 147 patients.The American journal of gastroenterology2007;102:1759-1764. [PMID: 17686073]
- Wasif N, Bentrem DJ, Farrell JJ, et al. Invasive intraductal papillary mucinous neoplasm versus sporadic pancreatic adenocarcinoma: a stage-matched comparison of outcomes. Cancer2010;116:3369-3377. [PMID: 20564064]
- Sohn TA, Yeo CJ, Cameron JL, et al. Intraductal papillary mucinous neoplasms of the pancreas: an updated experience. Annals of surgery2004;239:788-797. [PMID: 15166958]
- Poultsides GA, Reddy S, Cameron JL, et al. Histopathologic basis for the favorable survival after resection of intraductal papillary mucinous neoplasm-associated invasive adenocarcinoma of the pancreas. Annals of surgery2010;251:470-476. [PMID: 20142731]
- Benarroch-Gampel J, Riall TS. Extrapancreatic malignancies and intraductal papillary mucinous neoplasms of the pancreas.World J Gastrointest Surg. 2010;2:363-367. [PMID: 19844152]
- Choi M-G, Kim S-W, Han S-S, Jang J-Y, Park Y-H.High incidence of extrapancreatic neoplasms in patients with intraductal papillary mucinous neoplasms.Arch Surg2006;141:51-56. [PMID: 16415411]
- Larghi A, Panic N, Capurso G, et al. Prevalence and risk factors of extrapancreatic malignancies in a large cohort of patients with intraductal papillary mucinous neoplasm (IPMN) of the pancreas. Ann Oncol2013;24:1907-1911. [PMID: 23676419]
- Reid-Lombardo KM, Mathis KL, Wood CM, Harmsen WS, Sarr MG. Frequency of extrapancreatic neoplasms in intraductal papillary mucinous neoplasm of the pancreas: implications for management. Annals of surgery2010;251:64-69. [PMID: 19858708]
- 46.Sugiyama M, Atomi Y. Extrapancreatic neoplasms occur with unusual frequency in patients with intraductal papillary mucinous tumors of the pancreas. The American journal of gastroenterology1999;94:470-473. [PMID: 10022648]
- Khannoussi W, Vullierme MP, Rebours V, et al. The long term risk of malignancy in patients with branch duct intraductal papillary mucinous neoplasms of the pancreas.Pancreatology2012;12:198-202. [PMID: 22687372]
- Nair RM, Barthel JS, Centeno BA, Choi J, Klapman JB, Malafa MP. Interdisciplinary management of an intraductal papillary mucinous neoplasm of the pancreas.Cancer Control2008;15:322-333. [PMID: 18813200]
- Swartz MJ, Hsu CC, Pawlik TM, et al. Adjuvant chemoradiotherapy after pancreatic resection for invasive carcinoma associated with intraductal papillary mucinous neoplasm of the pancreas.International journal of radiation oncology, biology, physics2010;76:839-844. [PMID: 19647950]
- D'Angelica M, Brennan MF, Suriawinata AA, Klimstra D, Conlon KC. Intraductal papillary mucinous neoplasms of the pancreas: an analysis of clinicopathologic features and outcome. Annals of surgery2004;239:400-408. [PMID: 15075659]
- Schnelldorfer T, Sarr MG, Nagorney DM, et al. Experience with 208 resections for intraductal papillary mucinous neoplasm of the pancreas. Arch Surg2008;143:639-646. [PMID: 18645105]

