Keywords
Diabetes Mellitus; Hypertension; Pancreatitis
INTRODUCTION
Exocrine pancreatic disease is known to be associated with the onset of diabetes mellitus (DM), classified as type 3c [1]. Ewald et al. [2], found that of 1868 subjects diagnosed with DM, 172 (9.2%) had type 3c. The etiology of type 3c DM was chronic pancreatitis in 78.5% of cases, hereditary hemochromatosis in 7%, pancreatic cancer in 8%, and cystic fibrosis in 4%. Interestingly, the study did not address acute pancreatitis. According to the recent meta-analysis of Das et al. [3], including 936 patients with new-onset DM after an episode of acute pancreatitis, the pooled prevalence of DM was 23%, rising to 40% when prediabetes (pre-DM) was present prior to the pancreatitis.
The pathophysiology of DM following acute pancreatitis is poorly understood, and research is scarce. One study of 83 patients after an episode of acute pancreatitis found that 36% had abnormal glucose metabolism [4]. Insulin resistance was significantly associated with postpancreatitis DM owing to impaired removal of insulin from the circulation [4]. Another large-scale cohort study found that after an episode of pancreatitis, the risk of DM doubled [5].
Risk factors affecting the association between acute pancreatitis and subsequent DM have not been identified. The aim of the present study was to determine the prevalence of DM in patients after a first episode of acute pancreatitis and to identify risk factors for its development.
METHODS
Patients and Setting
A retrospective cohort design was used. The database of the emergency department of a tertiary universityaffiliated medical center was screened for patients aged 18 years or more who presented with a first episode of acute pancreatitis in 2010-2016. The diagnosis of acute pancreatitis was based on the presence of two of the following three criteria [6, 7] acute onset of persistent, severe, epigastric pain, often radiating to the back; serum lipase or amylase levels at least 3 times the upper limit of normal; characteristic findings of acute pancreatitis on computed tomography or magnetic resonance imaging. Patients with recurrent acute pancreatitis were excluded. Biliary pancreatitis was defined as pancreatitis with evidence of gallstone disease on any imaging modality [8]; alcoholic pancreatitis was defined as pancreatitis with a clinical history of alcohol abuse; and drug-induced pancreatitis was defined as pancreatitis associated with the use of class 1a drugs, as defined by Badalov et al. [9]. The pancreatitis was attributed to hypertriglyceridemia when admission triglyceride levels were more than 1000 mg/dL [8].
Patients in whom DM was diagnosed on follow-up after the acute pancreatitis episode were identified. The diagnosis of DM was based on accepted clinical criteria [10]: fasting plasma glucose >126 mg/dL (7.0 mmol/L) or 2-hour plasma glucose >200 mg/dL (11.1 mmol/L) during an oral glucose tolerance test (performed with a glucose load containing the equivalent of 75 gram anhydrous glucose dissolved in water) or HbA1C >6.5% (48 mmol/mol) or random plasma glucose levels >200 mg/dL (11.1 mmol/L) in a patient with classic symptoms of hyperglycemia or hyperglycemic crisis. The diagnosis of pre-DM was based on the following clinical criteria10: fasting plasma glucose 100–125 mg/dL or 2-hour plasma glucose level 140–199 mg/dL or HbA1c 5.7–6.4%.
Study Procedure
The cohort was divided into four groups: diagnosis of DM prior to onset of acute pancreatitis; diagnosis of DM after the episode of acute pancreatitis; diagnosis of pre-DM after the episode of acute pancreatitis; and normal glucose level throughout hospitalization for acute pancreatitis and follow-up. Clinical and laboratory data recorded during and after the index hospitalization period, both in-hospital and in the community setting, were collected from the medical files. The DM/pre-DM groups were compared with the normal-glucose group for age (>60 years), sex distribution, and vital signs in the emergency department (ED) and other clinical and laboratory parameters evaluated on presentation to the ED and during the first 24 hours thereafter. For evaluate the severity of AP we used the Bedside Index for Severity in Acute Pancreatitis (BISAP) [11], which includes: blood urea nitrogen (>25 mg/dL to >8.9 mmol/L) - 1 point, Glasgow coma score (<15) – 1 point, evidence of systemic inflammatory response syndrome - (SIRS is present when two or more of the following are found: 1) Temperature <36°C or >38°C 2) Respirations >20/min or PaCO2 <32 mmHg 3) Heart rate >90/min 4) WBC <4,000/mm(3) or WBC >12,000/mm(3) or more than 10% bands found on blood )– 1 point , evidence of pleural effusion on chest X ray - 1 points.
BISAP score predicts mortality - score of 0 to 2 Points: Lower mortality (<2 %) and score of 3 to 5 points: higher mortality (>15 %) [11].
Other parameters included etiology of the pancreatitis, length of hospitalization, intensive care unit admission, and mortality. If data were unclear or missing, the patient was contacted by telephone.
Statistical Analysis
The statistical analysis was generated using Statistical Analysis Software (SAS, version 9.4). Continuous variables are presented as mean and standard deviation, and categorical variables as number and percent. Continuous variables were compared between groups with Student t-test, and categorical variables were compared with Fischer exact test. A general linear model (GLM) was used for multivariate analysis. Two-sided p values <0.05 were considered statistically significant. As only patients with detailed information were included in the study, we did not account for invalid or missing information. For comparison of multiple groups, we used ANOVA calculation.
RESULTS
The study cohort consisted of 500 patients who presented with acute pancreatitis. They included 41 (8.2%) patients subsequently diagnosed with DM, 29 (5.6%) patients subsequently diagnosed with pre-diabetes, and 312 (62.4%) patients with normal glucose levels before and after the acute episode; the remaining 118 (23.6%) patients had a pre-existing diagnosis of DM. The demographic characteristics of the groups are shown in Table 1. The mean duration of follow-up was 6.7±3.1 years, and the mean interval from diagnosis of acute pancreatitis to diagnosis of DM was 1.46±1.4 years.
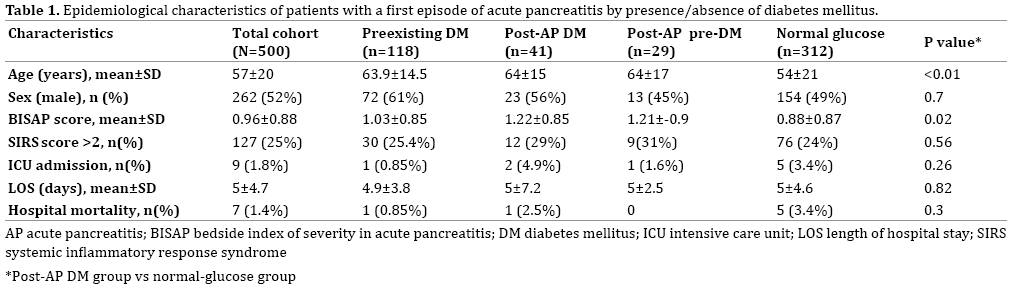
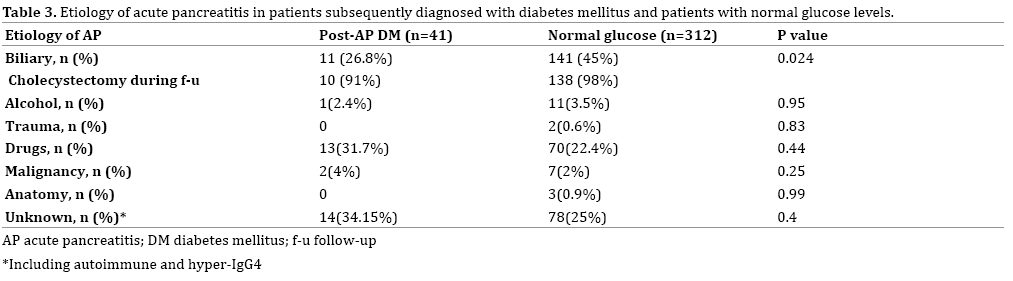
The patients with newly diagnosed post-pancreatitis DM were significantly older than the patients with normal glucose levels (64±15 years vs. 54±21 years p<0.01), and they had a significantly higher BISAP score (1.22±0.85 vs. 0.88±0.87, p=0.02) (Figure 1). The BISAP score was also significantly higher in the pre-DM group compared to the normal-glucose group (1.21±0.87 vs. 0.88±0.87, p<0.01). Although gallstones were the most common cause of pancreatitis overall (Table 2), non-biliary causes were significantly more common in the post-DM group than in the group with normal glucose levels (45% vs. 26.8%, p=0.02). None of the other clinical parameters or laboratory tests performed during or after hospitalization was found to be associated with the post-pancreatitis development of DM or pre-DM.
Figure 1. The BISAP score for patients with AP.
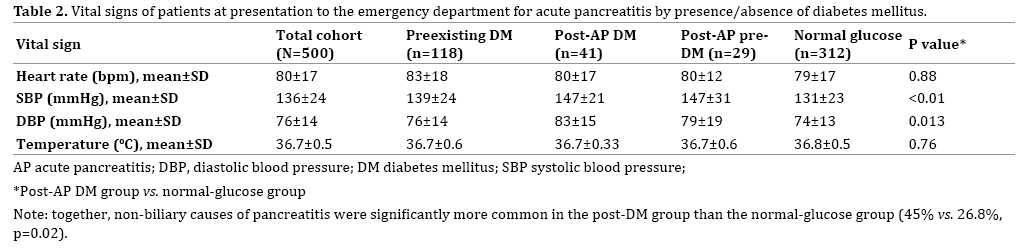
The patients’ vital signs at presentation to the emergency department for acute pancreatitis are shown in Table 3. Compared to the normal-glucose group, the patients subsequently diagnosed with DM had significantly higher values of systolic blood pressure (147±21 mmHg vs. 131±23 mmHg, p<0.01) and diastolic blood pressure (83±15 mmHg vs. 74±13 mmHg, p=0.013).
Multivariate analysis of the combined effects of sex, age, BISAP score, and etiology of pancreatitis yielded a significant interaction between age (p=0.06) and BISAP score (p=0.08) with post-pancreatitis DM/pre-DM.
DISCUSSION
The aim of the present study was to evaluate the rate and risk factors of DM diagnosed after a first episode of acute pancreatitis in a large cohort of patients presenting to the emergency department over a 5-year period. Given that acute pancreatitis may result in the destruction of some pancreatic tissue, the subsequent occurrence of diabetes is not unexpected. However, it has been demonstrated that DM following acute pancreatitis is associated with hyperinsulinemia [6], which suggests that acute pancreatitis and insulin resistance/hyperinsulinemia may have a common underlying mechanism.
Our analysis yielded an 8.2% rate of DM among patients with acute pancreatitis, which rose to 13.6% with the inclusion of patients with pre-DM. Interestingly, we found that pancreatitis due to causes other than biliary disease was significantly more common in the patients who acquired DM or pre-DM than in the patients with normal glucose levels. Although DM is considered a risk factor for the development of gallstones [12], none of the patients in the DM/pre-DM groups was so diagnosed before the pancreatitis episode. Therefore, it is possible that acute pancreatitis due to causes other than gallstones results in more extensive damage to beta cells. An analysis of insulin levels by cause of acute pancreatitis was beyond the scope of this study.
The patients who acquired DM after acute pancreatitis had a significantly higher blood pressure at presentation than patients with normal glucose levels. Of course, a single elevated blood pressure measurement in the emergency department does not establish a diagnosis of hypertension. However, a previous study of patients with gallstones reported that a significant proportion of those found to have elevated blood pressure at the emergency department visit acquired hypertension during follow-up [13]. Thus, it is possible that increased blood pressure in the emergency department signifies a tendency toward hypertension, with hypertension being associated with the development of DM or pre-DM as part of the metabolic syndrome.
The BISAP score is an easy-to-use validated tool for the assessment of the severity of acute pancreatitis, and it is amenable for use in the emergency department setting [14]. In the present study, a higher BISAP score was significantly associated with the development of DM. This finding suggests that patients presenting to the emergency department with more severe acute pancreatitis are at particularly high risk of the later development of DM. They should therefore be carefully monitored so DM can be diagnosed at an early stage, thereby preventing or delaying its complications. It is noteworthy that the major factor found to affect the association between BISAP score and diabetes development was patient age.
This study is limited by the retrospective design. Furthermore, the cohort was restricted to patients with a first episode of acute pancreatitis, and the conclusions may not be generalizable to patients with recurrent disease. As the glucose tolerance test was not performed routinely in all patients following the diagnosis of acute pancreatitis, the incidence of DM may have been underestimated. The severity and complications of DM were not evaluated.
CONCLUSIONS
According to the findings in the present study, about 8% of patients diagnosed with acute pancreatitis in the emergency room will go on to acquire DM. Several clinical variables are associated with the development of DM in this setting, including elevated blood pressure at presentation for acute pancreatitis, a non-biliary etiology of the pancreatitis, and a high BISAP score. Clinician awareness of these factors, particularly the BISAP score, may help them identify patients at risk for the future development of DM.
Conflict of Interest
The authors have no conflicts of interests to declare.
References
- Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Report of the expert committee on the diagnosis and classification of diabetes mellitus. Diabetes Care 2003; 26 Suppl 1:S5-S20. [PMID:12502614]
- Ewald N, Kaufmann C, Raspe A, Kloer HU, Bretzel RG, Hardt PD. Prevalence of diabetes mellitus secondary to pancreatic diseases (type 3c). Diabetes Metab Res Rev 2012; 28:338-342. [PMID: 22121010]
- Das SLM, Singh PP, Phillips ARJ, Murphy R, Windsor JA, Petrov MS. Newly diagnosed diabetes mellitus after acute pancreatitis: a systematic review and meta-analysis. Gut 2014; 63:818–831. [PMID: 23929695]
- Pendharkar SA, Asrani VM, Xiao AY, Yoon HD, Murphy R, Windsor JA, et al. Relationship between pancreatic hormones and glucose metabolism: A cross-sectional study in patients after acute pancreatitis. Am J Physiol Gastrointest Liver Physiol 2016; 311:G50-G58. [PMID: 27173509]
- Shen HN, Yang CC, Chang YH, Lu CL, Li CY. Risk of diabetes mellitus after first-attack acute pancreatitis: A national population-based study. Am J Gastroenterol 2015; 110:1698-1706. [PMID: 26526084]
- Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, et al. Classification of acute pancreatitis - 2012: revision of the Atlanta classification and definitions by international consensus. Gut 2013; 62:102-111. [PMID: 23100216]
- Greenberg JA, Hsu J, Bawazeer M, Marshall J, Friedrich JO, Nathens A, et al. Clinical practice guideline: management of acute pancreatitis. Can J Surg 2016; 59:128-140. [PMID: 27007094]
- Forsmark CE, Vege SS, Wilcox CM. Acute pancreatitis. N Engl J Med 2016; 375:1972-1981. [PMID: 27959604]
- Badalov N, Baradarian R, Iswara K, Li J, Steinberg W, Tenner S. Drug-induced acute pancreatitis: an evidence-based review. Clin Gastroenterol Hepatol 2007; 5:648-661. [PMID: 17395548]
- American Diabetes Association. Standards of medical care in diabetes-2016. Diabetes Care 2016; 39 (Suppl 1):S1-S106. [PMID: 26696680]
- Papachristou GI, Muddana V, Yadav D, O'Connell M, Sanders MK, Slivka A, et al. Comparison of BISAP, Ranson's, APACHE-II, and CTSI scores in predicting organ failure, complications, and mortality in acute pancreatitis. Am J Gastroenterol 2010; 105:435-441. [PMID: 19861954]
- Shiber-Ofer S, Shohat A, Grossman A. Elevated diastolic, not systolic, blood pressure measured in the emergency department predicts future development of hypertension in normotensive individuals. J Clin Hypertens 2015; 17:359-363. [PMID: 25706051]
- De Santis A, Attili AF, Ginanni Corradini S, Scafato E, Cantagalli A, De Luca C, et al. Gallstones and diabetes: a case-control study in a free-living population sample. Hepatology 1997; 25:787-790. [PMID: 9096577]
- Wu BU, Johannes RS, Sun X, Tabak Y, Conwell DL, Banks PA. The early prediction of mortality in acute pancreatitis: a large population-based study. Gut 2008; 57:1698-1703. [PMID: 18519429]


