Keywords
Acute malnutrition; Under five children; Refugee camp
Abbreviations
AOR: Adjusted Odds Ratio; ARRA: Administration for Refugee-Returnee Affairs; UNHCR: United Nations High Commission for Refugees; WHO: World Health Organization; WHZ: Weight-for-Height
Background
The government of Ethiopia opens door to refugees, hosting the largest refugee in Africa. The country is home to more than 676,000 refugees mainly from South Sudan, Somalia and Eritrean. More than 260,000 refugees are South Sudanese most of who arrived since conflict erupted in the world’s youngest nation in December 2013 [1,2].
Refugees in Africa and Asia live in a unique harsh environment for extended periods often confined to camps while being heavily dependent on continuous international food and other forms of assistance [3]. The dreadful situation of refugee camps in Kenya and Ethiopia makes the life of refugees very miserable. They face incredible daily hardships to meet their basic needs of life and rights to food, water, shelter, non-food items, education and health [4].
The in-kind food aids supplied by the United Nations High Commission for Refugees (UNHCR) comprised of wheat grain, rice, blended food, vegetable oil, pulses, sugar and salt, is provided to meet the daily 2,100 Kcal energy needs and essential/basic micronutrient requirements – food ration. A portion of the ration is usually sold for a variety of reasons: surplus, lack of essential nonfood items and purchase of complimentary foods [4-6].
Malnutrition among children in refugee is a critical public health concern due to the heightened vulnerability. The rate of malnutrition in refugees’ camp needs to be viewed as not just a health issue but as a serious protection and access to basic rights failure [4,7]. The magnitude of acute malnutrition among refugee camps in Ethiopia is relatively well-documented. A nutritional survey done in 2014 among south Sudanese refugee camps showed that the prevalence of acute malnutrition was almost two fold the emergency threshold of 15% [8,9].
Acute malnutrition is not only a condition that kills but also has a long term health and developmental consequences among recovered children after receiving an appropriate treatment. These long term consequences include an increased risk of stunted growth, impaired cognitive development and a greater chance of developing non-communicable diseases in adulthood. This demonstrates that it is of utmost importance to invest not only in the treatment of acute malnutrition but also in its prevention [9-11].
The problem as well as the solution of malnutrition is multi-faceted. In addition to an actual shortage of food; poor sanitation, a lack of available portable water, caring practices and insufficient health services are all significant factors contributing to the population’s overall nutritional status and health [4,7,12-14]. There is no a single silver bullet that will instantly eradicate malnutrition from the refugee camps but only through a holistic approach and strong group effort. Effective policies and programs to alleviate malnutrition require an understanding of the determinants of acute malnutrition in the refugee camps [4]. However; little information is known about the determinant of acute malnutrition in refuge setting of Ethiopia. Hence, this study identified the determinants of acute malnutrition in Tierkidi refugee camp, south west Ethiopia.
Methods
Study setting
The study was conducted in Tierkidi refugee camp in Gambella region, western Ethiopia from February to March, 2015. The camp is home to nearly 50,000 refugees who fled from the ongoing war in South Sudan.
Study design
A camp based case-control study was conducted. Cases were 6-59 months old children with acute malnutrition, weight-for-height Z-score (WHZ) below -2 based on WHO reference population while 6-59 months old children without malnutrition, WHZ ≥ -2 based WHO reference populations were control. Cases with known chronic illnesses like TB and HIV were excluded. In addition, a child who had lived in the camp for less than 6 months was excluded.
Sample size determination and sampling procedure
Sample size was calculated using EpiInfo software version 7 by assuming: 95% confidence interval, 80% power, control to case ratio of 2, an estimated proportion of timely initiation of complementary feeding (at 6 months after birth) among controls to be 6.9% and odds ratio of 3.39 [15]. The calculated sample size was 254 (85 cases and 169 controls). Considering non-response rate of 10% the total sample size became 281 (94cases and 187 controls).
Firstly, households were selected by systematic sampling. Secondly, anthropometric measurements were done for all the under five children in the selected households to select acutely malnourished children. When more than one under five children was acutely malnutrition in a household, the youngest child was included in the study. After recruiting of the cases, two controls were selected from the right and left neighbors of each case. If no control was found in the right and left immediate neighbors, the next households were used.
Data collection procedures and measurement
Anthropometric data of the children was measured based on the World Health Organization (WHO) standardized procedures. Weight and recumbent length/height was taken according to WHO standardized techniques [10]. Undressed or with minimal dressed children was weighed to the nearest 0.1 kg using 25 kg portable Salter spring scales, recumbent length/height was measured to the nearest 0.1 cm. The anthropometric measurements were done by trained nurses at home. Validation of measurements and random auditing were done on a daily basis.
Data on exposure variables were collected by face to face interview using structured questionnaire. The exposure variables were socio-demographic, child and maternal characteristics, child caring, history of childhood illness and heath seeking behaviors. Environmental factors were considered as constant to assess the childhood illness; the mothers were asked whether their children had been affected by diarrhea, fever and upper respiratory infection in the past two weeks. Diarrhea is defined as having three or more loose or watery stool in a 24 h’s period the two weeks period prior to the survey. Pre-lacteal feeding was assessed by asking a mother whether the child had been given anything to drink other than breast milk in the first three days after delivery. Exclusive breast feeding was assessed by asking a mother for how long the child fed breast exclusively.
Data processing and analysis
Data were checked, cleaned and entered in to EpiData software version 3.1, then exported to SPSS version 20. Data was analyzed by SPSS software. Anthropometric data was analyzed in WHO Anthro software.
Summary statistics were computed. Then, associations between independent variables and dependent variable were analyzed first using bivariate analysis to identify candidate variables factors with P-value<0.20. Multivariable logistic regression was applied using backward elimination method to identify factors independently associated with acute malnutrition at P-value<0.05. The crude and adjusted odds ratios together with their corresponding 95% Confidence Intervals (CI) were computed. A P-value<0.05 was considered to declare a result as statistically significant in this study. The result was presented in text, tables and graphs based on the types of data.
Ethical clearance was obtained from Institutional Review Board of Jimma University. Permission was obtained from administration for Refugee-Returnee Affairs (ARRA). Before starting the interview, oral informed consent was obtained from each respondent, care givers of the children. Respondents were assured that individual information would be kept confidential.
Results
A total of 94 cases and 187 controls were included in this study. All of study participants were singleton except one twin child in case group. The mean age of the cases and controls were 20.7 and 27.93 months, respectively. From cases and control groups 51 (54.3%) and 89 (47.6%) were male, respectively (Table 1). About 40% of cases and 25% of controls lived in household with more than one under five children (Figure 1).
| Variable |
Case |
Control |
| No (%) |
No (%) |
| Marital status |
|
|
| Married |
68 (72.3) |
164 (87.7) |
| Widowed and divorced |
26 (27.7) |
23 (12.3) |
| Family size |
|
|
| ≤ 5 |
34 (40.8) |
88 (47.1) |
| >5 |
60 (53.2) |
99 (52.9) |
| Sex of children |
|
|
| Female |
43 (45.7) |
98 (52.4) |
| Male |
51 (54.3) |
89 (47.6) |
| Age of children |
|
|
| 6-11 month |
18 (19.1) |
7 (3.7) |
| 12-23 month |
35 (37.2) |
51 (27.3) |
| 24-59 month |
41 (43.6) |
129 (69.0) |
| Birth order |
|
|
| ≤ 5 birth order |
55 (58.5) |
121 (64.7) |
| >5 birth order |
39 (41.5) |
66 (35.3) |
| Birth interval |
|
|
| ≥ 24 month |
49 (52.1) |
148 (79.1) |
| <24 month |
45 (47.9) |
39 (20.9) |
| Place of delivery |
|
|
| Health institution |
6 (6.4) |
16 (8.6) |
| Home |
88 (93.6) |
171 (91.4) |
| Birth planning |
|
|
| Yes |
68 (72.3) |
147 (78.6) |
Table 1: Sociodemographic characteristics of study participants in Terkidi Refugee camp, Ethiopia, 2015.
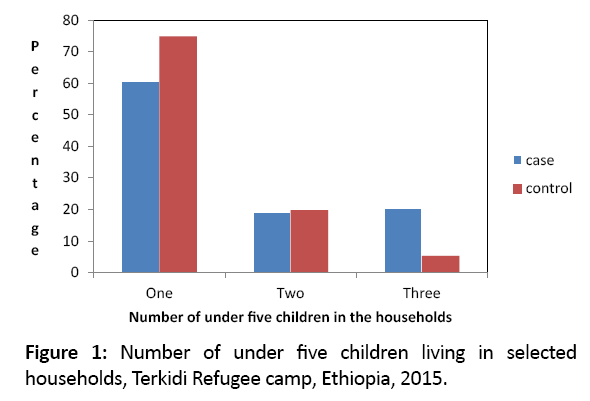
Figure 1: Number of under five children living in selected households, Terkidi Refugee camp, Ethiopia, 2015.
In the bivariate analysis, factors which showed an association at P-value<0.20 with acute malnutrition were family size, child age, diarrhea, fever, birth interval, pre-lacteal feeding, breast feeding practice and prompt health seeking behavior (Table 2).
| Variable |
Case |
Control |
P-value |
COR (95% CI) |
| No (%) |
No (%) |
| Marital status |
|
|
|
|
| Married |
68 (72.3) |
164 (87.7) |
|
1 |
| Widowed and Single |
26 (27.7) |
23 (12.3) |
0.002 |
2.72 (1.45, 5.11) |
| Family size |
|
|
|
|
| <=5 |
34 (40.8) |
88 (47.1) |
|
1 |
| >5 |
60 (53.2) |
99 (52.9) |
0.083 |
1.56 (0.94, 2.61) |
| Child age |
|
|
|
|
| 6-11 months |
18 (19.1) |
7 (3.7) |
0.000 |
8.09 (3.15, 20.73) |
| 12-23 months |
35 (37.2) |
51 (27.3) |
.007 |
2.159 (1.23, 3.76) |
| 24-59 months |
41 (43.6) |
129 (69.0) |
|
1 |
| Birth interval |
|
|
|
|
| ≥ 24 months |
49 (52.1) |
148 (79.1) |
|
1 |
| < 24 months |
45 (47.9) |
39 (20.9) |
0.000 |
3.48 (2.03, 5.96) |
| Diarrheal |
|
|
|
|
| No |
66 (70.2) |
168 (89.8) |
|
1 |
| Yes |
28 (29.8) |
19 (10.2) |
0.000 |
3.75 (1.96, 7.17) |
| Fever |
|
|
|
|
| No |
77 (86.0) |
180 (81.3) |
|
1 |
| Yes |
17 (18.1) |
7 (3.7) |
0.000 |
5.67 (2.26, 14.24)* |
| Pre-lacteal food |
|
|
|
|
| No |
28 (29.8%) |
71 (38.0%) |
|
1 |
| Yes |
66 (70.2%) |
116 (62.9%) |
0.177 |
1.44 (0.84, 2.45) |
| Exclusive BF |
|
|
|
|
| Yes |
20 (21.3) |
85 (45.5) |
|
1 |
| No |
74 (78.7) |
102 (54.5) |
0.000 |
4.44 (2.50, 7.86) |
| Time taken after the onset of Symptoms |
|
|
|
|
| Within 24 h |
48 (51.1) |
152 (81.3) |
|
1 |
| After 24 h |
46 (48.9) |
35 (18.7) |
0.000 |
4.16 (2.41, 7.18) |
Table 2: Candidate variables for multivariable logistic regression analysis.
After controlling for confounding, age of the child, breast feeding practice, birth interval and health seeking practice for sick child were found to significant association with acute malnutrition.
Age of the child was statistically significant association with acute malnutrition. Younger children (6-11 months) were 10 times more likely to be acutely malnourished than children in the age group of 24-59 months (AOR=9.81; 95% CI: 2.69, 35.75). Diarrheal disease in the last 2 weeks preceding the survey was also seen as one of the determinant of acute malnutrition among under five children. Acute malnutrition was 4 times more likely to occur in children who had diarrhea compared to children who hadn’t diarrhea (AOR=3.77; 95% CI: 1.55, 9.17). However, morbidity status of the child by fever in the last 2 weeks preceding the survey was not associated with wasting in the current study. Breast feeding practice was associated with acute malnutrition. The odd of acute malnutrition among non-exclusively breastfed children was 4 compared with children who exclusively breastfed in the first 6 months of life (AOR=3.70: 95% CI: 1.64, 8.33). Birth interval showed significant association with acute malnutrition. The odd of acute malnutrition among children with shorter birth interval was 6.7 compared with children with longer birth interval, more than 2 years (AOR=6.70; 95% CI 2.89, 15.54). Children who were not taken to clinic within 24 h of the onset of illness were 6 times more likely to be wasted than those children who were taken within 24 h of the onset of illness (AOR=5.89; 95% CI 2.49, 13.94) (Table 3).
| Variable |
Case(n=94)
No. (%) |
Control(n=187)
No. (%) |
COR (95% CI) |
AOR (95% CI) |
| Diarrhea |
|
|
|
|
| No |
66 (70.2) |
168 (89.8) |
1 |
1 |
| Yes |
28 (29.8) |
19 (10.2) |
3.75 (1.96, 7.17) |
3.77 (1.55, 9.17) |
| Child age |
|
|
|
|
| 6-11 months |
18 (19.1) |
7 (3.7) |
8.09 (3.15, 20.73) |
9.81 (2.69, 35.75) |
| 12-23 months |
35 (37.2) |
51 (27.3) |
2.15 (1.23, 3.76) |
1.24 (0.54, 2.86) |
| 24-59 months |
41 (43.6) |
129 (69.0) |
1 |
1 |
| Birth interval |
|
|
|
|
| ≥ 24 months |
49 (52.1) |
148 (79.1) |
1 |
1 |
| <24 months |
45 (47.9) |
39 (20.9) |
3.48 (2.03, 5.96) |
6.70 (2.89, 15.54) |
| Exclusive BF |
|
|
|
|
| Yes |
20 (21.3) |
85 (45.5) |
1 |
1 |
| No |
74 (78.7) |
102 (54.5) |
4.44 (2.50, 7.86) |
3.70 (1.64, 8.33) |
| Health care seeking |
|
|
|
|
| Prompt |
48 (51.1) |
152 (81.3) |
1 |
1 |
| Delayed |
46 (48.9) |
35 (18.7) |
4.16 (2.41, 7.18) |
5.89 (2.49, 13.94) |
Adjusted for marital status, family size, fever and pre-lacteal feeding
Table 3: Independent predictors of acute malnutrition among south Sudanese under five children in Terkidi Refugee camp, Ethiopia 2015.
Discussion
In this study, acute malnutrition among under five children in the refugee camp was significantly associated with age of the child, exclusive breast feeding practice, birth interval and health seeking practice for sick child.
Moreover, the presence of diarrhea was associated with acute malnutrition. Similarly studies amongst refugees in Sudan and Uganda showed that the risk of acute malnutrition increased with increasing communicable disease burden including malaria, diarrhea and pneumonia [16-18]. There are several mechanisms through which communicable diseases predispose to poor nutrition including poor appetite, malabsorption and chronic ill health.
Initiation of additional foods before 6 months of age increased wasting among children. The same result was observed in other similar studies [10,18,19]. Exclusive breastfeeding is recommended because breast milk is uncontaminated and contains all the nutrients necessary in the first few months of life. In addition, the mother’s antibodies in breast milk provide the infant with immunity to disease. Early supplementation exposes infants to pathogens and thus increases the risk of infection, especially diarrheal disease. It decreases infants’ intake of breast milk and therefore suckling, which in turn reduces breast milk production [14,17].
Short birth interval increased the likely hood of acute malnutrition. This finding is similar with evidence from studies in Bangladesh and Eastern rural Ethiopia [20,21]. Short birth intervals are closely associated with poor health of children, especially during infancy. Children born too soon after a previous birth are at increased risk for health problems and death at an early age. Longer birth intervals improve the health status of both mother and child [22].
This study could have the following limitations. One is that the nutritional surveys are prone to technical error of anthropometric measurement, which could result in misclassification of children’s nutritional status. The study‘s findings could also be affected by recall bias due to the backward inquiry of exposure variables. Furthermore, maternal autonomy in decision making of donations was not assessed.
Conclusion
In this study short birth interval, younger child age, and inappropriate infant and young child caring practices were determinants of acute malnutrition in refugee camp. The implication of this finding is that food ration alone is not enough to prevent malnutrition in refugee camps. Like in general population, promoting appropriate infant and young child feeding practice and providing family planning in refugee camps is crucial to alleviate the level of malnutrition in refugee camps.
Acknowledgement
We would like to thank ARRA, Tierkidi refugee camp administration, study participants, community health workers of Tierkidi camp for their cooperation during data collection and Goal Ethiopia for supporting by material and human resource.
Authors’ Contributions
YG participated in the design of the study, data collection, performed statistical analysis and drafted the first manuscript. WK participated in design of the study and helped in draft preparation and reviewed the manuscript. LD participated in design of the study and helped in draft preparation and reviewed the final manuscript. All authors have read and approved the final manuscript.
References
- UNECA. Executive secretary visits south Sudanese refugees in Ethiopia 2015.
- European commission humanitarian aid and civil protection. ECHO Factsheet, Ethiopia 2014; 1-3.
- International Organization for Migration. Nutrition surveillance reports: Health assessment programme 2011; 1-10.
- Corbett M, Oman A. Acute malnutrition in protracted refugee situations: A global strategy. NHCR/WFP Global Nutrition Strategy 2006.
- Doocy S, Tappis H, Haskew C, Wilkinson C, Spiegel P. Performance of UNHCR nutrition programs in post-emergency refugee camps. Confl Health 2011; 5: 23.
- NRC/CMP Camp Management Tool kit. Food distribution and nonfood items. Norwegian Refugee Council, the Camp Management Project, Oslo, Norway 2008.
- Young H, Jaspars S. The meaning and measurement of acute malnutrition in emergencies humanity. Pract Netw 2006; 44.
- Generation Nutrition. Acute malnutrition: An everyday emergency. 2014; 1-32.
- Center for disease control and prevention. Notes from the field : Malnutrition and elevated mortality among refugees from South Sudan, Ethiopia 2014; 1-6.
- UNICEF, WHO, The World Bank. Levels and trends in child malnutrition 2012; 1-35.
- Black R, Victora C, Walker S, Bhutta Z, Christian P, et al. Maternal and child under nutrition and overweight in low-income and middle-income countries. Lancet Matern Child Nutr Series 2014; 1-12.
- Habtom K, Bezatu M, Tadesse A, Damtew B. Prevalence of acute malnutrition and its associated factors among children aged 6-59 months in Mai-Aini Eritrean Refugees’ Camp. Nutr Food Sci 2014; 5: 1-7.
- Cronin AA, Shrestha D, Abdalla C, Ezard N, Aramburu C. A review of water and sanitation provision in refugee camps in association with selected health and nutrition indicators the need for integrated service provision. J Water Health 2008; 6.
- Lapping K, Schroeder D, Marsh D, Albalak R, Jabarkhil M. Comparison of a positive deviant inquiry with a case-control study to identify factors associated with nutritional status among Afghan refugee children in Pakistan. Food Nutr Bull 2012; 23.
- Solomon A, Zemene T. Risk factors for severe acute malnutrition in children under the age of five: A case-control study. Ethiop J Health Dev 2008; 22: 1-5.
- Olwedo M, Hanifa M, OrachC. Factors associated with malnutrition among children in internally displaced person’s camps, northern Uganda. Afr Health Sci 2008; 8.
- Shears P, Berry AM, Murphy R, Nabil MA. Epidemiological assessment of the health and nutrition of Ethiopian refugees in emergency camps in Sudan 1985. Br Med J 1987; 295: 314-318.
- Orach GC. Morbidity and mortality amongst southern Sudanese in Koboko refugee camps, Arua district, Uganda. East Afr Med J 1999; 74: 195-199.
- Bantamen G, Belaynew W, Dube J. Nutrition and food assessment of factors associated with malnutrition among under five years age children at Machakel Woreda, Northwest Ethiopia : A case control study. Nutr Food Sci 2014; 4: 1-7.
- Dereje N. Determinants of severe acute malnutrition among under five children in Shashogo Woreda, Southern Ethiopia: A community based matched case control study. Nutr Food Sci 2014; 4.
- Rayhan I, Khan MS. Factors causing malnutrition among under five children in Bangladesh. 2006; 5: 558-562.
- Ethiopian Central Statistical Agency. Ethiopia demographic and health survey. ICF International Calverton, Maryland 2011; 1-452.

