Dionysios Dellaportas1, Nikolaos Arkadopoulos2, Panagis Michael Lykoudis3, Despoina Myoteri4, Amanda Psyrri5, Pantelis Vassiliu2, Panagiotis Athanasopoulos6, Andreas Polydorou1, Ioannis Vassiliou1, Vassilios Smyrniotis2
12nd Department of Surgery and 24th Department of Surgery, Attikon University Hospital, Athens 124 62, Greece
3Division of Surgery and Interventional Science, University College London, London WC1E 6BT, UK
4Histopathology Department, ‘Tzaneion’ General Hospital, Piraeus 185 36, Greece
52nd Department of Internal Medicine, Propedeutic, Oncology Section, Attikon University Hospital, Athens 124 62, Greece
6Department of Hepatobiliary and Pancreatic Surgery, Royal Free London Hospital NHS Foundation Trust, London NW3 2QG, UK
- *Corresponding Author:
- Dionysios Dellaportas
2nd Department of Surgery
Aretaieion University Hospital
Athens 115 28, Greece
Tel + 00306947718723
Fax +00302107286128
E-mail dellapdio@gmail.com
Received October 04th, 2016 - Accepted November 11th, 2016
Keywords
Pancreaticoduodenectomy; Pancreatic Neoplasms
Abbreviations
ELND extended lymph node dissection; IVC; inferior vena cava; PD pancraticoduodenectomy; PV portal vein; SMA superior mesenteric artery
INTRODUCTION
Pancreaticoduodenectomy (PD) is in vast majority the optimal surgical approach for patients with what collectively are called periampullary tumors, such as malignancies of the pancreatic head, distal bile duct, ampulla of Vater and second part of duodenum [1]. Although PD is a surgically demanding procedure, thanks to several technological innovations it is considered a routine operation for specialized centres. Such innovations are mostly focused in the reconstruction of alimentary tract and have led to decreased morbidity [2]. On the other hand, the survival benefit of PD has not been improved as tangibly as postoperative morbidity. In this context, the extent of regional lymphadenectomy is another field of dispute, considering the poor overall survival of patients who Undergo PD with curative intent. A substantial number of studies already addressed the theoretical benefit of extended lymph node dissection in PD, failing to prove any survival benefit, with the downside of increased postoperative complications [3].
The aim of this study was to evaluate the effect of extended lymphadenectomy in a subgroup of patients with early stage periampullary cancer based on the assumption that cancer cells might be still confined into the resection field of lymphatic drainage, and also record the intraoperative parameters, the postoperative complications and overall survival in these patients.
METHODS
This was a prospective cohort study. From January 2005 until December 2010, 152 consecutive patients underwent PD in a single institution for periampullary adenocarcinoma. Half of these patients were subjected to standard PD, and comprised the control group of this study (n=76) while the other half underwent standard PD with concomitant meticulous resection of the lymphatic tissue of the hepatoduodenal ligament, the superior mesenteric artery lymph nodes and the paracaval lymph nodes above the renal artery, between the aorta and the inferior vena cava (IVC), comprising the study group (n=76). All recruited patients were operated with curative intention and written informed consent was obtained. All operations were carried out by the same surgical team and primary operating surgeon (VS). None of the patients had received neoadjuvant chemoradiation. Only cases with histological confirmation of R0 resection were included in this study. Preoperative evaluation of resectability was obtained with computed tomography scan with pancreatic protocol (CT pancreas) and in equivocal cases with the aid of magnetic resonance imaging (MRI) of the upper abdomen and magnetic resonance cholangiopancreatography (MRCP).
Surgical Technique
Patients were positioned supine, and following standard prep, the abdominal cavity was accessed through a bilateral subcostal (rooftop) incision. The tumour resectability was assessed and the pancreaticoduodenal resection was carried out in the standard fashion. Namely, the pancreaticoduodenal specimen was taken out with the common hepatic duct as the cranial border of the operation, the duodenum was divided 1-2 cm distally to the pylorus and the jejunum was divided 10-15 cm distally to the ligament of Treitz, while the pancreas was divided at the neck of the organ after dissection of the portal vein (PV). The uncinate process of the pancreas was dissected, up to the right and posterior aspect of the superior mesenteric artery (SMA), with careful ligation of branches to the right side of the PV. Restoration of the continuity of the alimentary tract was achieved in the same manner in all cases. Briefly, an isolated short loop of jejunum was prepared and mobilized for an end-to-side, duct-to-mucosa pancreatico-jejunal anastomosis using polydioxanone 4-0 interrupted sutures, and the duodeno-jejunal anastomosis was performed in the same loop with interrupted absorbable 3-0 sutures. A hepatico-jejunal end-to-side anastomosis was carried out with polydioxanone 4-0 interrupted or continuous suture, and the above short jejunal limb with the pancreaticojejunal and duodeno-jejunal anastomosis was finally anastomosed 30-40cm distally to the hepaticojejunostomy in an end-to-side fashion using absorbable 3-0 suture material. It is worthwhile to emphasize that dilatation of the pyloric sphincter was consistently carried out before the duodenal-jejunum joint.
For the extended lymph node dissection (ELND) group, the resection of the above described standard specimen included also: a) all lymphatic tissue of the hepatoduodenal ligament, starting at the origin of the common hepatic artery and extending upwards towards the hilar plate; b) retroperitoneal lymph nodes extending from the right renal hilum to the left lateral border of the aorta in the horizontal axis, and from the portal vein till below the third portion of the duodenum in the vertical axis. In order to achieve the latter, right colon mobilization was essential, similar to Cattell-Braasch maneuver, standardized for emergency retroperitoneal trauma approach [4], which gives excellent exposure to the root of superior mesenteric vessels and right retroperitoneal space. The lymphatics between SMA and aorta, as well as the uncinate process of the pancreas were visualized and easily removed with the above described maneuvers. Great care was taken to avoid any damage to any aberrant hepatic artery arising from the SMA. For both groups, the operation was finalized using a 30 French silastic drain close to the pancreaticojejunostomy site. The drain was removed on postoperative day three if drain output was less that 30 mL over 24 hours and drain amylase was normal.
Follow-up of all patients was carried out by an independent colleague; equally, long-term outcomes were monitored by an oncologist and a surgeon.
STUDY DESIGN
The subjects of each surgical technique group were divided in two subgroups according to the size of the primary tumor. Group I, including the standard PD patients, was subdivided into subgroup Ia (n=34), where tumor size was ≤2 cm, and Ib (n=42) for tumors with maximum diameter >2 cm. On the other hand, group II patients, representing the ELND cases, were assigned into subgroup IIa (n=37) and IIb (n=39), using again the 2 cm tumor size as threshold respectively. Primary end point of this study was the comparison of the postoperative morbidity and mortality of the two groups and secondarily the assessment of long term survival. The role, if any, of the ELND technique might be related to tumor size, rationalized by the assumption that smaller tumors may be contained into local lymphatic basins, and more aggressive surgical resections might be beneficial.
ETHICS
Written informed consent was obtained from each patient and the study protocol conforms to the ethical guidelines of the "World Medical Association Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects" adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964 and amended by the 59th WMA General Assembly, Seoul, South Korea, October 2008, as reflected in a priori approval by the hospital’s research ethics committee.
STATISTICS
Sample size was estimated to be thirty patients per each subgroup in order to detect clinically significant difference at least 30% between the two groups with a power 0.8 and a (alpha) error 0.05, aiming to achieve statistical validity. Comparison between groups was analyzed using Chi-square and Mann-Whitney tests as appropriate. Significance was accepted in the 0.05 level as applicable. Statistical analysis was conducted using IBM SPSS Statistics v.20 software (IBM Corp, USA). A survival analysis was performed using the Kaplan–Meier method.
RESULTS
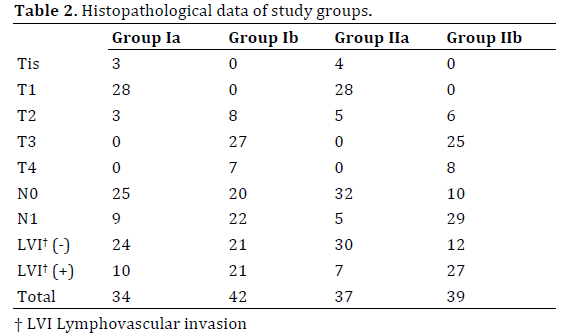
Demographics, operative and postoperative data are shown in Table 1. The median patients’ age was 61 and 62 years respectively in the two groups and male gender was predominant in both groups (65.8% vs. 60.6% male in standard PD and ELND group respectively). There were no major differences in age and gender distribution among study groups. Finally, there was no significant difference between study groups regarding the histological type and stage of the tumor (Table 2). Moreover, in both groups the vast majority of final histopathology revealed primary pancreatic adenocarcinoma.
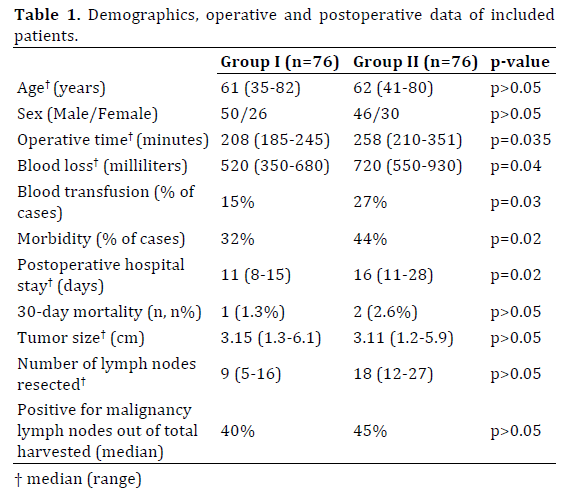
Considering the intraoperative parameters, the median operative time was clearly lower in the standard PD patients, with difference of median values of 50 minutes as demonstrated in Table 1, while the operative blood loss was substantially higher in the ELND. These results of course were expected since the surgical field becomes larger and lymph nodes harvesting is more time-consuming resulting usually in increased blood loss. In accordance with the above observations is the fact that ELND group patients tended to have longer hospital stay postoperatively, with a median difference of 5 days.
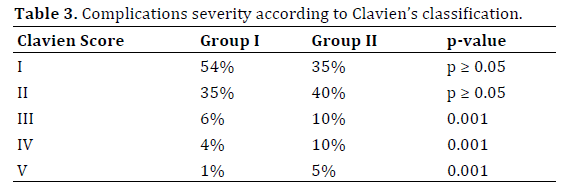
Complications were grouped in categories according to Clavien-Dindo classification system (Table 3). One patient in the first group died on the 13th postoperative day due to myocardial infraction and two patients in the ELND group died on the 10th and 9th postoperative day of uncontrollable pancreatic fistula and intra-abdominal collections, which did not respond to interventional radiology drainage and finally developed sepsis, with multiorgan failure forbidding surgical intervention. Pancreatic fistula rate was higher (10%) in group II again compared to a 6% in standard PD patients that developed this complication. Six patients in the ELND group also were re-admitted with large chylous collections for investigations and interventional radiology drainage was performed in those with early signs of infection. Delayed gastric emptying was not significantly different between groups, and as emphasized above, dilatation of the pylorus before performing the duodenojejunal anastomosis is strongly advised as a preventive measure of that condition, at least for the immediate postoperative period.
Actuarial survival analysis is shown in Figures 1 and 2, comparing groups Ia to IIa and Ib to IIb respectively. As it is demonstrated in Figure 2 there are no significant differences in survival among patients with larger tumors, neither with the standard nor with the ELND surgical approach. In addition, the main aim to investigate if there was any difference in survival for patients with small tumors and ELND yielded no statistically significant difference in the aforementioned groups. Given that the null hypothesis could not be rejected, an attempt for further assessment with multivariate analysis was deemed not necessary.
Figure 1. Kaplan-Meier survival analysis and comparison of groups Ia and IIa.
Figure 2. Kaplan-Meier survival analysis and comparison of groups Ib with IIb.
DISCUSSION
The aim of this prospective cohort study was to evaluate the extended lymphadenectomy in periampullary cancer patients and especially in those with small size and presumably earlier stage tumors. The theoretical background of this long standing question in surgical oncology of periampullary malignancies is that an earlier tumor might have not spread systematically and aggressive locoregional resection and lymph nodal clearance could mitigate that metastatic potential. As it is shown in this study's results, there is no significant survival difference between the groups of ELND and classic PD patients either in patients with smaller or in patients with larger primary tumors. The analysis did not detect any difference between the two groups, with the expense of excess operative time, blood loss, hospital stay and obviously postoperative complications for the ELND patients.
These results and conclusions are in accordance with previous studies trying to assess this complex issue as well as meta-analyses addressing similar questions [5, 6, 7]. Even large randomized trials did not show any survival benefit for more radical procedures [8], also emphasizing the increased complication rate in patients, who are usually malnourished and sometimes with additional comorbidities undergoing an already major procedure [9]. On a recent meta-analysis, including five randomized clinical trials addressing the matter of extended lymphadenectomy, final conclusion is that standard pancreaticoduodenectomy has less morbidity and equivalent long-term benefits [10]. It is admittedly difficult to standardize the technique of extended lymph node dissection and variations are reported among studies addressing this issue, nevertheless none of those demonstrated a solid survival benefit yet. Some authors proposed larger pancreatic resections as removing more pancreatic tissue would result in less local recurrence rates and possibly better control of the locoregional disease again failing to demonstrate significant benefits, yet further increasing the rates of postoperative diabetes and malabsorption [11, 12].
The role of genetics is becoming more important in provision of new insights in periampullary cancer biology, and systemic therapies are probably the main field that promises improved survival for these patients. Imaging modalities are becoming more sensitive and premalignant lesions can be detected and managed by minimally invasive approaches, preventing thus progress to malignancy in relevant cases. Surgical efforts will continue to aim towards technical refinement, and in future extended resections could possibly be reconsidered along with chemotherapy improvements.
In conclusion, pancreaticoduodenectomy is an extensive operation and despite improvements in postoperative complications management and continuous technical advances, there is still no evidence in favour of extension of the operation for increased lymph node harvesting. This study did not detect any significant benefit deriving from an extensive lymph node clearance approach. Further studies in genetics and oncological innovations are needed in the treatment of this morbid malignant disease, which arises in an abdominal site requiring complex operative manoeuvers.
Conflict of Interest
All authors declare having no conflict of interests or financial disclosures.
References
- Yeo CJ, Cameron JL, Lillemoe KD, Sohn TA, Campbell KA, Sauter PK, Coleman J, et al. Pancreaticoduodenectomy with or without distal gastrectomy and extended retroperitoneal lymphadenectomy for periampullary adenocarcinoma, part 2: randomized controlled trial evaluating survival, morbidity, and mortality. Ann Surg 2002; 236:355-66; discussion 66-8. [PMID: 12192322]
- Vollmer CMJr, Sanchez N, Gondek S, McAuliffe J, Kent TS, Christein JD, Callery MP, et al. A root-cause analysis of mortality following major pancreatectomy. J Gastrointest Surg 2012; 16:89-102; discussion-3. [PMID: 22065319]
- Xu X, Zhang H, Zhou P, Chen L. Meta-analysis of the efficacy of pancreatoduodenectomy with extended lymphadenectomy in the treatment of pancreatic cancer. World J Surg Oncol 2013; 11:311. [PMID: 24321394]
- Zhang J, Qian HG, Leng JH, Cui M, Qiu H, Zhou GQ, Wu JH, et al. Long mesentericoportal vein resection and end-to-end anastomosis without graft in pancreaticoduodenectomy. J Gastrointest Surg 2009; 13:1524-8. [PMID: 19082669]
- Pedrazzoli S, DiCarlo V, Dionigi R, Mosca F, Pederzoli P, Pasquali C, Klöppel G, et al. Standard versus extended lymphadenectomy associated with pancreatoduodenectomy in the surgical treatment of adenocarcinoma of the head of the pancreas: a multicenter, prospective, randomized study. Lymphadenectomy Study Group. Ann Surg 1998; 228:508-17. [PMID: 9790340]
- Farnell MB, Aranha GV, Nimura Y, Michelassi F. The role of extended lymphadenectomy for adenocarcinoma of the head of the pancreas: strength of the evidence. J Gastrointest Surg 2008; 12:651-6. [PMID: 18085343]
- Michalski CW, Kleeff J, Wente MN, Diener MK, Buchler MW, Friess H. Systematic review and meta-analysis of standard and extended lymphadenectomy in pancreaticoduodenectomy for pancreatic cancer. Br J Surg 2007; 94:265-73. [PMID: 17318801]
- Kennedy EP, Yeo CJ. Pancreaticoduodenectomy with extended retroperitoneal lymphadenectomy for periampullary adenocarcinoma. Surg Oncol Clin N Am 2007; 16:157-76. [PMID: 17336242]
- Reddy SK, Tyler DS, Pappas TN, Clary BM. Extended resection for pancreatic adenocarcinoma. Oncologist 2007; 12:654-63. [PMID: 17602057]
- Dasari BV, Pasquali S, Vohra RS, Smith AM, Taylor MA, Sutcliffe RP, Muiesan P, et al. Extended Versus Standard Lymphadenectomy for Pancreatic Head Cancer: Meta-Analysis of Randomized Controlled Trials. J Gastrointest Surg 2015; 19:1725-32. [PMID: 26055135]
- Manabe T, Ohshio G, Baba N, Miyashita T, Asano N, Tamura K, Yamaki K, et al. Radical pancreatectomy for ductal cell carcinoma of the head of the pancreas. Cancer 1989; 64:1132-7. [PMID: 2547508]
- Glanemann M, Shi B, Liang F, Sun XG, Bahra M, Jacob D, Neumann U, et al. Surgical strategies for treatment of malignant pancreatic tumors: extended, standard or local surgery? World J Surg Oncol 2008; 6:123. [PMID: 19014474]



