Keywords
Abdominal Pain; CA-19-9 Antigen; Endosonography; Pancreatitis, Chronic; Pancreatic Neoplasms
INTRODUCTION
Radial endoscopic ultrasonography has become a technique used worldwide [1] and is very useful in bilio-pancreatic diseases [2]. Its ongoing development has led to a change in the clinical management of patients with these pathologies [3]. However, this technique should be more frequently used by endoscopists, due to its clinical usefulness in the correct management of patients [4]. It has also been shown that EUS is effective in the study of benign pathologies such as acute pancreatitis [5], chronic pancreatitis [6], and biliary lithiasis [7]. EUS permits the detection of small intrapancreatic tumors [8], and some authors advocate the use of this technique for an initial study of suspected small intrapancreatic tumors, avoiding the use of other diagnosing techniques [9]. This consideration is very important as this neoplasia has a poor prognosis [10]. CA 19-9 has been identified as a tumoral marker [11] having a high sensitivity [12] in patients with pancreatic neoplasia, but having a low specificity. CA 19-9 levels are also elevated in other benign pathologies [13] such as digestive pathologies (including acute pancreatitis, pancreatic pseudocyst, cholangitis, cholecystitis, hepatitis, or cirrhosis), respiratory processes (including bronchiectasis, tuberculosis, asbestosis, bronchial asthma, fibrosis of the lung and idiopathic interstitial pneumonia), renal cysts and rheumatologic disorders (such as Sjögren’s syndrome, rheumatoid arthritis, Sharp’s syndrome, arteritis of giant cells, dermatopolymyositis and rheumatic polymyalgia). This marker is also elevated in other malignant pathologies of the gastrointestinal tract [14]. Considering the usefulness of EUS in assessing the biliopancreatic area both in benign and malignant pathologies, our aims were to determine the most frequent pathologies in patients with an asymptomatic elevation of CA 19-9 and to assess the usefulness of EUS in diagnosing patients with idiopathic abdominal pain and elevation of CA19-9.
MATERIALS AND METHODS
Patients
A retrospective descriptive study was performed and data on patients who came to our Gastroenterology Department from October 1st, 2004 to September 30th, 2005 were collected in a setting involving a 600 bed hospital which serves 250,000 inhabitants.
All patients who were sent to our department for EUS on the basis of suspected biliopancreatic disease and who presented an elevation of CA 19-9 (equal to or greater than 37 U/mL) in the week before EUS were included in the study. Patients with acute pancreatitis, with a dilated bile duct or a biliopancreatic space-filling lesion on US or helical CT were excluded. Twenty-two patients met the inclusion criteria. The patients were subdivided into two categories: patients with an asymptomatic elevation of serum CA 19-9 and patients with abdominal pain of unknown etiology and an elevation of CA 19-9.
Methods
Patients included in our study underwent EUS and helical CT. EUS was performed with an Olympus UM160 endoscope. The biliopancreatic area was explored using frequencies of 5 and 7.5 MHz which allowed for a deeper exploration, but sectorial EUS fine needle aspiration and endoscopic retrograde cholangiopancreatography were not performed.
Data Recorded
Serum CA 19-9 was evaluated in the week before EUS using the ARCHITECT 12000 CA 19-9 XR kit (Abbott, Abbott Park, North Chicago, IL, USA). Serum bilirubin values were also recorded since it is widely known that high bilirubin levels might interfere with the determination of CA 19-9 [15]. The field of the specialist who had previously seen the patients and the findings of both the abdominal ultrasonography (US) and the helical computerized tomography (CT) were recorded. Finally, the results of the EUS examination are described.
ETHICS
The study was approved by the Ethics Committee of the Complexo Hospitalario de Pontevedra, Pontevedra, Spain. All the patients were managed according to the usual accepted standards of clinical practice.
RESULTS
Out of the 22 patients enrolled in this study, 15 patients had an asymptomatic elevation of CA 19-9 while 7 patients had elevated CA 19- 9 levels as well as abdominal pain.
Patients with Asymptomatic Elevation of serum CA 19-9
The EUS findings and the final attributable cause of the elevation of CA 19-9 in the 15 patients who were referred due to an asymptomatic elevation of CA 19-9 are shown in Table 1. None of them showed bilio-pancreatic neoplastic pathology at EUS. In these patients, chronic pancreatitis was considered when they showed the following parameters: lobulation of the pancreatic border (Figure 1), presence of intrapancreatic echogenic foci and irregularity of Wirsung’s duct 2) parenchymal criteria plus 1 ductal criteria) [16]. Liver cirrhosis was diagnosed when lobulation of the hepatic lobe border was present, visualized from the stomach and the duodenal bulb [17]. Choledocholithiasis was diagnosed when hyperechogenic imaging inside the choledochus showed posterior acoustic shadowing [18]. Microlithiasis (Figure 2) was diagnosed when an intravesicular starry-sky pattern was observed. Renal cysts were visualized as anechoic images with dorsal acoustic accentuation inside the renal parenchyma. In the other referred patients, we attributed the elevation of CA 19-9 to other pathologies such as Sjögren’s syndrome or drug-induced hepatitis with eosinophilia. In one patient, we could not establish a definitive etiology of the asymptomatic elevation of serum CA 19-9.
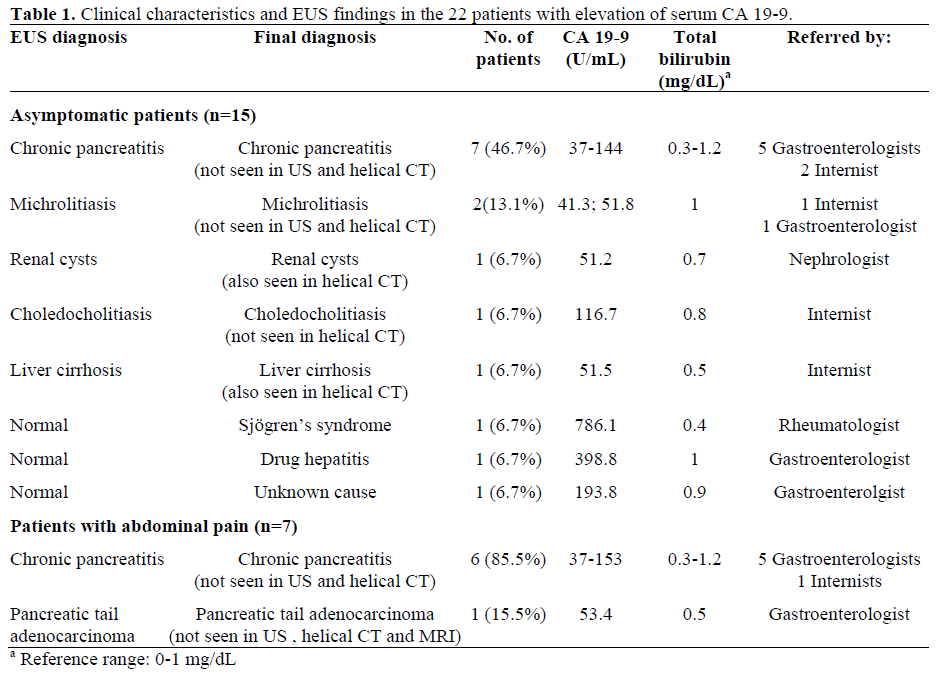
Figure 1. Chronic pancreatitis.
Figure 2. Microlithiasis.
Patients with Abdominal Pain and Elevation of serum CA 19-9
The patients referred mild epigastric and left hypochondrium abdominal pain. No abdominal lesions were detected at US and helical CT (Table 1). An early pancreatic neoplasia (a 12 mm mass in the pancreatic tail) was detected at EUS in one patient with a serum CA 19-9 level of 53.4 U/mL (Figure 3). In this patient, an MRI also failed to show any pancreatic lesions. The patients underwent surgery; the tumor was classified as pT1, N0, M0 and the pathological study confirmed the diagnosis of ductal adenocarcinoma with perineural infiltration in the pancreatic exocrine portion and an adjacent desmoplastic reaction (Figure 4).
Figure 3. Pancreatic tail adenocarcinoma.
Figure 4. Pathologic findings of pancreatic tail cancer.
DISCUSSION
Asymptomatic elevation of serum CA 19-9 is not considered an indication for EUS [19]. However, because this tumor marker is used frequently, its positive results usually lead to further investigation, which might include EUS. No case of pancreatic neoplasia was found in patients who were referred with an asymptomatic elevation of CA 19-9, which seems to be in agreement with previous published studies [20]. Furthermore, it has been reported in the literature that the sensitivity of EUS is better than that of helical CT in the detection of early morphological changes in chronic pancreatitis [21]. Pancreatic gland changes related to chronic pancreatitis were detected in about 50% of the patients. It has been reported that there may be a slight increase in serum CA 19-9 levels in patients with chronic pancreatic disease without an associated neoplasia [22]. A cutoff level of 300 U/mL has been established to differentiate this entity from an associated neoplasia, although the determination of this marker in pancreatic juice may be more accurate [23]. Cases diagnosed in our study as chronic pancreatitis had values of CA 19-9 which ranged from 38 to 144 U/mL. The use of EUS together with other biochemical parameters has been pointed out for an early diagnosis of chronic pancreatitis , considering the high alcohol intake in our country [24]. Liver cirrhosis may also slightly increase the levels of CA 19-9 and, therefore, 50% of the patients with chronic pancreatitis had also presented a morphology suggestive of cirrhosis on previous helical CT. At this point, a correct clinical history is necessary in order to exclude other extrapancreatic causes in the elevation of CA 19-9, such as rheumatic disease or kidney cysts which have been described as other causes of an altered serum CA 19-9 level.
Less aggressive procedures such as US are preferably used as a first step in investigating the bilio-pancreatic area. Recently, EUS has become an important addition in the study of these patients [25]. For a long time, ERCP was considered to be the gold standard in establishing a final diagnosis of chronic pancreatitis (Cambridge classification) [26]. Nowadays, EUS can be compared to ERCP alone or associated with analysis of pure pancreatic juice obtained after secretin stimulation [27].
In spite of the small number of cases, EUS disclosed diseases which were not seen using other imaging methods and ruled out pancreatic cancer in all of them. This observation suggested that EUS should be used more frequently which implies agreement with former studies where the importance of pancreatic cancer exclusion was stressed [9].
Our study shows no cases of neoplastic pathology and it shows that the most prevalent pathology is chronic pancreatitis in patients with an asymptomatic elevation of CA 19-9.
On the other hand, a frequent clinical problem is patients suffering from abdominal pain where a bilio-pancreatic origin is suspected. Less aggressive procedures such as US are preferably used as a first step in the diagnosis. Recently, EUS has become an important addition in the study of these patients [25]. The agreement between CT and endoscopic ultrasound studies revealed EUS to be more accurate in diagnosing benign and malignant pathologies [28].
Nevertheless, with the forthcoming multidetector CT, this difference may disappear [29], although it should be considered that the cost of EUS is lower than that of helical CT [30].
In our study, 86% of the patients with abdominal pain (6/7) had chronic pancreatitis with CA 19-9 levels ranging from 38 to 153 U/mL. Clinical symptoms showed mild epigastric pain. Considerations related to the value of EUS diagnosis in chronic pancreatitis patients are similar to those that are shown above. In none of the cases was serum IgG4 determined to exclude autoimmune pancreatitis [31] since, in all cases, an elevated alcoholic intake was prevalent in the population studied [24]. It is important to point out the detection of an early adenocarcinoma of the pancreatic tail in a 75-year-old woman with two negative imaging studies (US and helical CT), a patient with mild abdominal pain irradiating to the back and a slight CA 19-9 elevation (53.4 U/mL). MRI was also performed on this patient, since this technique allows a noninvasive assessment of the pancreas [32]. Notwithstanding the fact that no pancreatic pathology was demonstrated and the fact that the results of the EUS were suspicious, a distal pancreatectomy was performed, showing the presence of a well-differentiated 12 mm adenocarcinoma with a free surgical edge and no adenopathies in the anatomopathologic exam. Currently, this patient is asymptomatic and shows no signs of recurrence. Nevertheless, it has been reported that some patients cannot synthesize the antigen (negative Lewis’ genotype) and, therefore, they show low levels of CA 19-9 in the presence of an adenocarcinoma. Consequently, the normality of the serum level of CA 19-9 cannot exclude the presence of a pancreatic adenocarcinoma [33].
Our conclusions, according to the study objectives, are as follows: 1) in patients with an asymptomatic elevation of CA 19-9, the most prevalent pathology was chronic pancreatitis and no case showed a neoplastic pathology; 2) in patients with unexplained abdominal pain and an elevation of serum CA19-9, EUS is helpful inasmuch as chronic pancreatitis is the most frequent disease due to high alcohol intake. EUS with a slight elevation of CA 19-9 allowed us to detect an early pancreatic tail adenocarcinoma in a patient who had been suffering from a backache for several months and had notable weight and appetite loss. The combination of clinical data, a careful interpretation of serum CA19-9 determination and EUS leads to the correct management of bilio-pancreatic pathologies.
References
- DiMagno EP, Buxton JL, Regan PT, Hattery RR, Wilson DA, Suarez JR, Green PS. Ultrasonic endoscope. Lancet 1980; 1:629-31. [PMID 6102631]
- Inui K, Kida M, Fujita N, Maguchi H, Yasuda K, Yamao K. Standard imaging techniques in the pancreatobiliary region using radial scanning endoscopic ultrasonography. Digestive Endoscopy 2004; 16(Suppl):S118-33.]
- Chong AK, Caddy GR, Desmond PV, Chen RY. Prospective study of the clinical impact of EUS. GastrointestEndosc 2005; 62:406-10. [PMID 16111959]
- Fujita N. Obstacles to widespread USE of endoscopic ultrasonography in the diagnosis of biliopancreatic diseases. Digestive Endoscopy 2002; 14:S30-1. ]
- Frossard JL, Sosa-Valencia L, Amouyal G, Marty O, Hadengue A, Amouyal P. Usefulness of endoscopic ultrasonography in patients with "idiopathic" acute pancreatitis. Am J Med 2000; 109:196-200. [PMID 10974181]
- Thuler FP, Costa PP, Paulo GA, Nakao FS, Ardengh JC, Ferrari AP. Endoscopic ultrasonography and alcoholic patients: can one predict early pancreatic tissue abnormalities? JOP. J Pancreas (Online) 2005; 6:568-74. [PMID 16286707]
- Tse F, Barkun JS, Barkun AN. The elective evaluation of patients with suspected choledocholithiasis undergoing laparoscopic cholecystectomy.GastrointestEndosc 2004; 60:437- 48. [PMID 15332044]
- Ikeda M, Sato T, Ochiai M, Morozumi A, Ainota T, Fujino MA. Diagnosis of small pancreatic tumor by endoscopic ultrasonography. Bildgebung 1993; 60:209- 14. [PMID 8118187]
- Klapman JB, Chang KJ, Lee JG, Nguyen P. Negative predictive value of endoscopic ultrasound in a large series of patients with a clinical suspicion of pancreatic cancer. Am J Gastroenterol 2005; 100:2658- 61. [PMID 16393216]
- Birk D, Beger H. Neoadjuvant, adjuvant, and palliative treatment of pancreatic cancer. CurrGastroenterol Rep 2001; 3:129-35. [PMID 11276380]
- Koprowski H, Steplewski Z, Mitchell K, Herlyn M, Herlyn D, Fuhrer P. Colorectal carcinoma antigens detected by hybridoma antibodies. Somatic Cell Genet 1979; 5:957-71. [PMID 94699]
- Clave P, Boadas J, Gonzalez-Carro P, Mora J, Perez C, Martinez A, et al. Accuracy of imaging techniques and tumor markers in the diagnosis ofpancreatic cancer. GastroenterolHepatol 1999; 22:335-341. [PMID 10535205]
- Akdogan M, Sasmaz N, Kayhan B, Biyikoglu I, Disibeyaz S, Sahin B. Extraordinarily elevated CA19-9 in benign conditions: a case report and review of the literature. Tumori 2001; 87:337-9. [PMID 11765186]
- Takahashi Y, Takeuchi T, Sakamoto J, Touge T, Mai M, Ohkura H, et al. The usefulness of CEA and/or CA19-9 in monitoring for recurrence in gastric cancer patients: a prospective clinical study. Gastric Cancer 2003; 6:142-5. [PMID 14520526]
- Halm U. Perioperative CA19-9 levels can predict stage and survival in patients with resectable pancreatic adenocarcinoma. J ClinOncol 2006; 24:5610. [PMID 17158548]
- Lankisch PG. The problem of the diagnosing chronic pancreatitis.Dig Liver Dis 2003; 35:131-4. [PMID 12779064]
- Hsieh JS, Jan CM, Lu CY, Chen FM, Wang JY, Huang TJ. Preoperative evaluation of endoscopic ultrasonography and portography in selecting devascularization surgery for esophagogastricvarices. Am Surg 2005; 71:439-44. [PMID 15986978]
- Sgouros SN, Bergele C. Endoscopic ultrasonography versus other diagnostic modalities in the diagnosis of choledocholithiasis. Dig Dis Sci 2006; 51:2280-6. [PMID 17080253]
- Yusuf TE, Harewood GC, Clain JE, Levy MJ. International survey of knowledge of indications for EUS.GastrointestEndosc 2006; 63:107-11. [PMID 16377326]
- Chang CY, Huang SP, Chiu HM, Lee YC, Chen MF, Lin JT. Low efficacy of serum levels of CA 19-9 in prediction of malignant diseases in asymptomatic population in Taiwan. Hepatogastroenterology 2006; 53:1-4. [PMID 16506366]
- Draganov P, Toskes PP. Chronic pancreatitis. CurrOpinGastroenterol 2002; 18:558-62. [PMID 17033333]
- Kayhan B, Kayhan B, Akdogan M. Can IL-2R alpha be a valuable marker along with CA 19-9 in the diagnosis of chronic pancreatitis and pancreatic cancer.Int J Biol Markers 2004; 19:196-202. [PMID 15503821]
- Nouts A, Levy P, Voitot H, Bernades P. Diagnostic value of serum Ca19.9 antigen in chronic pancreatitis and pancreatic adenocarcinoma. GastroenterolClinBiol 1998; 22:152-9. [PMID 9762189]
- Guallar-Castillon P, Rodriguez-Artalejo F, DiezGanan LD, BanegasBanegas JR, LafuenteUrdinguio PL, Herruzo Cabrera RH. Consumption of alcoholic beverages and subjective health in Spain. J Epidemiol Community Health 2001; 55:648-52. [PMID 11511643]
- Sung JJ. Endoscopic ultrasonography and magnetic resonance cholangiopancreatography in abdominal pain: what makes sense? Endoscopy 2001; 33:668-75. [PMID 11490389]
- Axon AT, Classen M, Cotton PB, Cremer M, Freeny PC, Lees WR. Pancreatography in chronic pancreatitis: international definitions. Gut 1984; 25:1107-112. [PMID 6479687]
- Wiersema MJ, Hawes RH, Lehman GA, Kochman ML, Sherman S, Kopecky KK. Prospective evaluation of endoscopic ultrasonography and endoscopic retrograde cholangiopancreatography in patients with chronic abdominal pain of suspected pancreatic origin.Endoscopy 1993; 25:555-64. [PMID 8119204]
- Minniti S, Bruno C, Biasiutti C, Tonel D, Falzone A, Falconi M, Procacci C. Sonography versus helical CT in identification and staging of pancreatic ductal adenocarcinoma. J Clin Ultrasound 2003; 31:175-82. [PMID 12692824]
- Horton KM. Multidetector CT and threedimensional imaging of the pancreas: state of the art. J GastrointestSurg 2002; 6:126-8. [PMID 11992794]
- Ainsworth AP, Rafaelsen SR, Wamberg PA, Pless T, Durup J, Mortensen MB. Cost-effectiveness of endoscopic ultrasonography, magnetic resonance cholangiopancreatography and endoscopic retrograde cholangiopancreatography in patients suspected of pancreaticobiliary disease. Scand J Gastroenterol 2004; 39:579-83. [PMID 15223684]
- Hughes DB, Grobmyer SR, Brennan MF. Preventing pancreaticoduodenectomy for lymphoplasmacyticsclerosing pancreatitis: cost effectiveness of IgG4. Pancreas 2004; 29:167. [PMID 15257110]
- Schima W. MRI of the pancreas: tumours and tumour-simulating processes. Cancer Imaging 2006; 6:199-203. [PMID 17208676]
- Tempero MA, Uchida E, Takasaki H, Burnett DA, Steplewski Z, Pour PM. Relationship of carbohydrate antigen CA 19.9 and Lewis antigens in pancreatic Cancer. Cancer Res 1987; 47: 5501-3. [PMID3308077]





