Maikel Bakens1, Bengt van Rijssen2, Victor van Woerden3, Marc Besselink2, Djamila Boerma4,
Olivier Busch2, Kees Dejong3,5,10, Michael Gerhards6, Jeanin van Hooft11, Yolande Keulemans7,
Joost Klaase8, Misha Luyer1, Quintus Molenaar9, Jelmer Oor4, Erik Schoon12, Willemijn Steen6,
Dorine Tseng9, Dirk Jan Gouma2, Ignace de Hingh1
1Department of Surgery, Catharina Hospital, Eindhoven, the Netherlands
2Department of Surgery, Cancer Center Amsterdam, Academic Medical Center Amsterdam, the
Netherlands
3Department of Surgery, Maastricht University Medical Center, Maastricht, the Netherlands
4Department of Surgery, Sint Antonius, Nieuwegein, the Netherlands
5NUTRIM School for Nutrition Toxicology and Metabolism, and GROW School for Oncology &
Developmental Biology, Maastricht, the Netherlands
6Department of Surgery, Onze Lieve Vrouwe Gasthuis, Amsterdam, the Netherlands
7Department of Gastroenterology, Maastricht University Medical Center, Maastricht, the Netherlands
8Department of Surgery, Medical Spectrum Twente, Enschede, the Netherlands
9Department of Surgery, Utrecht Medical Center, Utrecht, the Netherlands
10Department of Surgery, Universitätsklinikum Aachen, Aachen, Germany
11Department of Gastroenterology, Academic Medical Center Amsterdam, the Netherlands
12Department of Gastroenterology, Catharina Hospital, Eindhoven, the Netherlands
- *Corresponding Author:
- Ignace de Hingh
Department of Surgery
Catharina Hospital Eindhoven
Michelangelolaan 2
5623 EJ Eindhoven, the Netherlands
Tel: +31 40 2399111
Fax: +31 40 2455035
E-mail: ignace.d.hingh@catharinaziekenhuis.nl
Received October 29th, 2017 - Accepted January 10th, 2018
Keywords
Pancreatoduodenectomy; Pancreatic Neoplasms
Abbreviations
PBD preoperative biliary drainage;
PD pancreatoduodenectomy
INTRODUCTION
Most patients with a pancreatic and periampullary
tumor present with obstructive jaundice. Elevated bilirubin
levels are known to result in coagulation disorders,
impaired cell-mediated immunity, impaired anastomotic
healing and a higher risk for developing sepsis [1, 2, 3].
For these reasons, preoperative biliary drainage (PBD) to
lower bilirubin levels prior to pancreatoduodenectomy
(PD) was routinely used for decades to improve the patients’ general condition and to decrease the chance
of postoperative morbidity and mortality. Since the PBD
introduces a risk for complications by itself (e.g. post-
ERCP pancreatitis and cholangitis), it has been a matter
of debate whether PBD should be performed routinely
or only on indication [4, 5, 6, 7, 8, 9, 10, 11]. In a Dutch
randomized controlled multicenter trial which compared
PBD with plastic endoprothesis to early surgery (within
one week of diagnosis) [12], patients with obstructive
jaundice in periampullary tumors with bilirubin levels
below 250 μmol/l at the time of randomization appeared
to have a significantly higher rate of complications
after PBD. Therefore, in the Netherlands the preferred
treatment in these patients is currently early surgery,
preferably performed within one week after diagnoses
and without PBD [13]. The aim of this study was to
investigate the current practice of PBD in the Netherlands
in patients operated for suspected periampullary tumors.
Furthermore, we aimed to gain insight in the reasons for
PBD prior to pancreatoduodenectomy.
METHODS
Data Collection
Data were retrospectively collected from medical
patient charts in seven Dutch high-volume (≥20 PDs
for pancreatic cancer/year) centers (Academic Medical
Center, Amsterdam; Catharina Cancer Institute,
Eindhoven; Medical Spectrum Twente, Enschede;
Maastricht University Medical Center, Maastricht;
OLVG, Amsterdam; Sint Antonius Hospital, Nieuwegein;
University Medical Center, Utrecht) and included
patient characteristics, preoperative diagnostic and
treatment procedures and tumor characteristics.
The aim of the study was to determine the proportion of
PBD in patients with obstructive jaundice with bilirubin
levels lower than 250 μmol/l. Furthermore, documented
reasons for drainage were collected as well as differences
in the proportion of patients undergoing PBD in high
volume centers.
Patient Selection
All patients undergoing PD for suspected-periampullary
malignancy in 2013 and 2014 were analyzed. Patients
undergoing PD in an emergency setting were excluded.
Preoperative bilirubin levels were recorded and only
patients presenting with jaundice and bilirubin levels
between 21.0 μmol/l and 250 μmol/l were included for
further analysis. The cut-off point of 250 μmol/l was
chosen since only patients with bilirubin levels lower than
250 μmol/l were included in the RCT demonstrating the
negative impact of pre-operative biliary drainage [12].
In patients with bilirubin levels above 250 μmol/l the
decision whether or not to perform pre-operative drainage
is still under debate.
Preoperative Biliary Drainage
PBD was defined as preoperative biliary drainage
performed by endoscopic retrograde cholangiography (ERCP) or percutaneous transhepatic bile duct drainage
(PTCD). The type of drainage and type of stent (plastic or
metal) that was used was recorded.
Indications for PBD
All hospital charts of patients undergoing PBD were
scrutinized to identify the main reason of the treating
physicians to perform a PBD. In total 6 categories could be
identified: ‘diagnostic’ (if PBD was performed after contrast
injection in the bile duct during ERCP for diagnostic reasons),
“cholangitis / pancreatitis”, “suspicion of choledocholithiasis”,
“waiting list” (if early surgery could not be provided in the
expert center), “neo-adjuvant therapy” and “no medical
reasons” (if none of the previous reasons were identified).
Ethics
All methods were carried out in accordance with
the Helsinki Declaration of 1964 and later versions.
The medical ethical committee was consulted and they
concluded that according to the Dutch law on Medical
Research in Humans and given the retrospective design,
the current study did not require informed consent by
involved patients. According to Good Clinical Practice, all
patient derived data were anonymised.
Statistical Analysis
Statistic analyses were performed by using IBM SPSS
statistics version 22. P-values lower than 0.05 were
considered statistically significant.
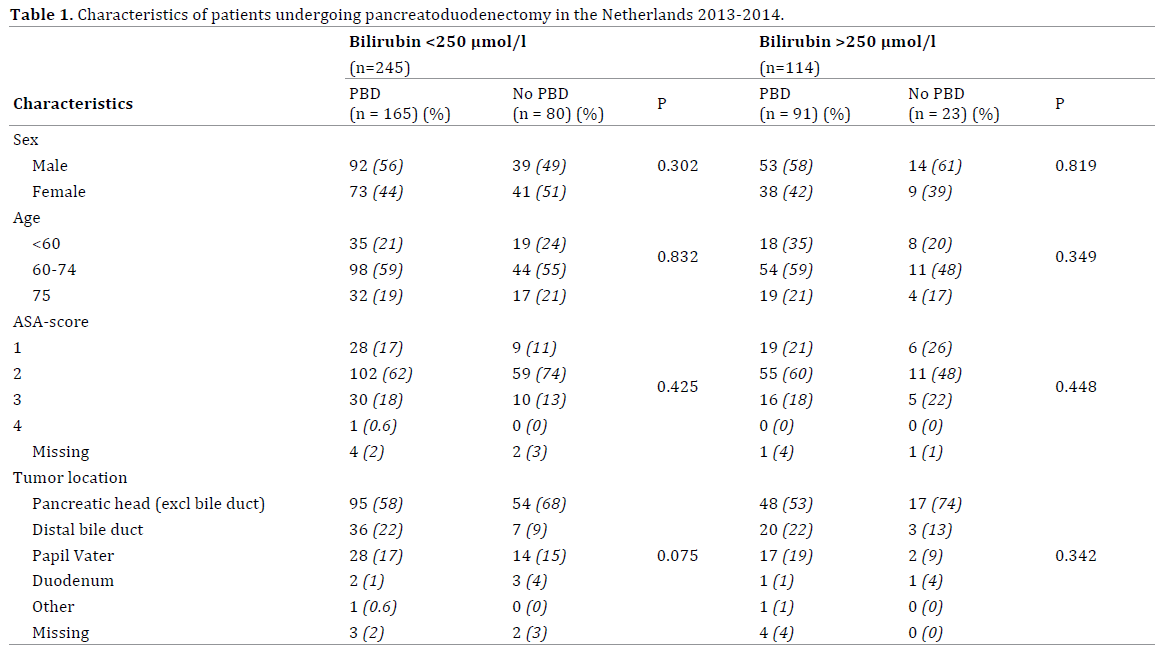
RESULTS
In total, 609 patients underwent a PD for suspected
pancreatic or periampullary cancer. Elevated bilirubin levels
were present in 401 (66%) of these patients: below 250
μmol/l in 245 (61%) patients and above 250 μmol/l in 114
patients (28%). In 42 (11%) patients pre-operative bilirubin
levels were missing and these patients were excluded from
further analysis. The 245 jaundiced patients were further
analysed. Baseline characteristics of the patients included in
this study are presented in Table 1.
In 80 (33%) patients presenting with bilirubin
levels below 250 μmol/l early surgery without PBD
was performed. The remaining patients (n=165, 67%)
underwent PBD prior to surgery. In the majority of patients,
no medical reason to justify a PBD could be retrieved from
the medical charts (n=102, 62%), Table 2. More than half
of the stented patients were already stented in the hospital
of diagnosis prior to referral to an expert center (n=88,
53%). Another 61 patients (37%) underwent PBD in the
expert center after referral. The total proportion of PBD
differed significantly between pancreatic centers (Table
3). Also the proportion of PBD performed after referral
differed significantly between centers ranging from 13% to
58% (p<0.001) (Figure 1). PBD was most often performed
by using a plastic stent (n=112, 68%).
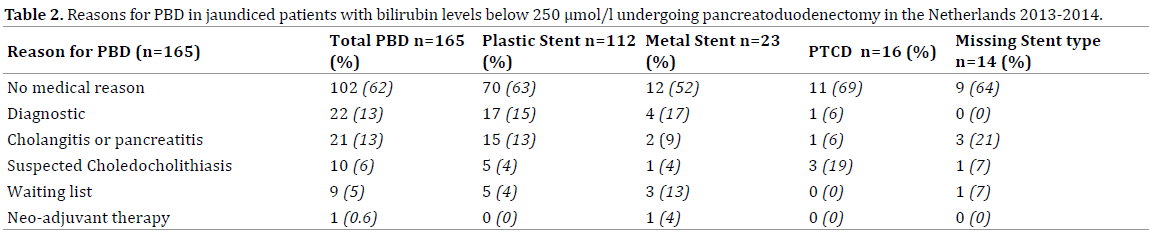
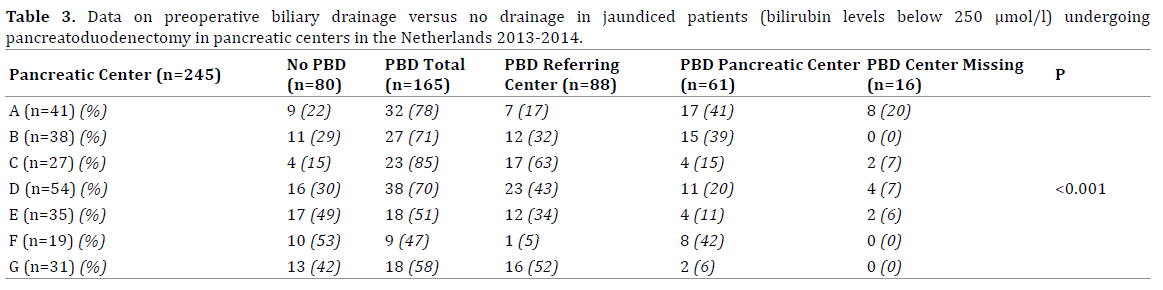
Figure 1. Proportion of PBD performed in pancreatic centers after referral of jaundiced patients (bilirubin levels below 250 μmol/l) undergoing
pancreatoduodenectomy in the Netherlands 2013-2014.
DISCUSSION
The current study revealed that the vast majority of
jaundiced patients with a pancreatic or periampullary cancer still undergo PBD prior to surgery in the
Netherlands. In total 66% of patients with bilirubin levels
<250 μmol/l underwent PBD and in most of them, no
obvious medical reason to justify a PBD could be retrieved
from the medical charts. In most patients, PBD was
performed already before referral to a surgical unit in an
expert center. However, a relevant proportion of patients
underwent PBD prior to surgery in pancreatic centers after
referral. The proportion of patients being stented in expert
centers varied significantly between centers.
PBD has been subject of debate for many years. In 2010
Van der Gaag et al. published the results of the Dutch RCT
that randomized patients with a bilirubin below 250 μmol/l to undergo PBD prior to surgery with plastic endoprothesis
versus early surgery alone. Early surgery was defined, as
‘preferably within one week after randomization’. The
reason to have a maximum waiting time in the early surgery
group is that at randomization a maximum bilirubin level
of 250 μmol/l was accepted and by waiting longer than a
week, bilirubin levels may become to high for safe surgery.
The RCT showed that a higher proportion of patients in the
PBD-group suffered postoperative and drainage-related
complications compared to patients in the early surgery
group without PBD [12]. Severe complications occurred in
73.5% of the drainage group, compared to 39.4% the early
surgery group [12]. This difference was mainly caused by post PBD complications such as cholangitis (26%). Since
then, the recommendation in the Netherlands has been to
perform early surgery without PBD whenever bilirubin
levels are <250 μmol/l. This recommendation was accepted
by all expert centers in the Netherlands, as they had all
been participating in the RCT. However, adhering to this
recommendation was anticipated to be challenging, as the
interval of only one week between diagnosis and surgery
may be difficult to achieve, especially as most patients are
diagnosed in hospitals that do not perform surgery.
The current study investigated the daily clinical
practice in the Netherlands 3-4 years after publication
of the RCT. Rather surprisingly it was revealed that the
majority of patients with bilirubin levels below 250 μmol/l
still underwent PBD prior to surgery. In the majority of
patients, no urgent medical reason could be retrieved
from the medical charts. Although “waiting list / inability
to operate within one week” was specifically mentioned in
a small proportion of the patients, this may have played
a major role in the patients in whom no specific medical
reason was noted. In the RCT, the median time to surgery
was already 9 days in the surgery group without PBD,
hinting towards difficulties to perform surgery within one
week [12].
The proportions of PBD after referral performed in
pancreatic centers differed considerably between centers,
varying between 13 and 58 percent for patients with
bilirubin levels below 250 μmol/l. As referral to expert
centers is based upon regional patterns, it is unlikely
that case-mix variations within patients account for this
difference in the amount of patients undergoing PBD.
Therefore, it may well be assumed that this difference
is caused by logistical hurdles within the expert centers
themselves to realize surgical treatment within one week
after referral.
If PBD by ERCP seems to be indicated, the type of
stent that will be used, plastic vs. metal, should also be
considered. The use of plastic stents has been one of the
criticisms on the Dutch RCT [12]. PBD is still indicated
in case of extreme hyperbilirubinemie, cholangitis,
and the necessity for nutritional support or if it is not
possible to perform early surgery because of logistical
hurdles. Furthermore, PBD can be indicated in patients
who undergo neo-adjuvant treatment [14]. A recent
study by Tol et al. showed that the use of a covered
metal stent instead of plastic stent reduces stent related
complications (metal 6% vs. plastic 30%) and is costeffective
in spite of the higher costs of the metal stent
itself [14, 15, 16].
Although it might have been interesting, the current study
does not describe postoperative complications after PBD as
compared to early surgery since the retrospective design of
this study does not allow a reliable collection of these data.
CONCLUSION
The current study should raise awareness in pancreatic
centers that in spite of the well-investigated and published
beneficial effects of early surgery without PBD, this is not
yet achieved in the majority of patients. In the absence
of obvious medical reasons in the charts to justify PBD,
logistic problems to perform early surgery in the expert
centers are the most likely explanation for this practice.
Therefore, improving logistics within expert centers, as
well as within the referring hospitals is needed to improve
the outcome of these patients.
Acknowledgements
The authors thank all participating hospitals and the
Dutch pancreatic cancer group.
This study was funded by a grant from the Dutch Cancer
Society (KWF) (grant number 2013-649). The funding
source had no role in the study design, data collection and
analysis, the writing of the manuscript or the submission
for publication.
Author Contribution Statement
M. Bakens initiated the study with D. Gouma and I. de
Hingh. M. Bakens collected data, performed analyses and
wrote the main manuscript and prepared figures and
tables.
L. van Rijssen, V. van Woerden, M. Besselink D. Boerma,
O. Busch. C. Dejong, M. Gerhards, J. van Hooft, Y. Keulemans,
J. Klaase, M. Luyer, I. Molenaar, J. Oor, E. Schoon, W. Steen,
D. Tseng, D. Gouma and I. de Hingh collected data in
participating hospitals. Furthermore they improved the
main manuscript text.
Conflict of Interest
The authors declare no conflict of interest.
References
- Katz SC, Ryan K, Ahmed N, Plitas G, Chaudhry UI, Kingham TP, et
al. Obstructive jaundice expands intrahepatic regulatory T cells, which
impair liver T lymphocyte function but modulate liver cholestasis and
fibrosis. J Immunol 2011; 187:1150-1156. [PMID: 21697460]
- Kawarabayashi N, Seki S, Hatsuse K, Kinoshita M, Takigawa
T, Tsujimoto H, et al. Immunosuppression in the livers of mice
with obstructive jaundice participates in their susceptibility to
bacterial infection and tumor metastasis. Shock 2010; 33:500-506.
[PMID: 19823116]
- Chowdhury AH, Camara M, Martinez-Pomares L, Zaitoun AM, Eremin
O, Aithal GP, et al. Immune dysfunction in patients with obstructive jaundice
before and after endoscopic retrograde cholangiopancreatography. Clin
Sci (Lond) 2016; 130:1535-1544. [PMID: 27252406]
- Moole H, Bechtold M, Puli SR. Efficacy of preoperative biliary drainage
in malignant obstructive jaundice: a meta-analysis and systematic review.
World J Surg Oncol 2016; 14:182. [PMID: 27400651]
- Liu C, Lu JW, Du ZQ, Liu XM, Lv Y, Zhang XF. Association of
Preoperative Biliary Drainage with Postoperative Morbidity after
Pancreaticoduodenectomy. Gastroenterol Res Pract 2015; 796893.
[PMID: 26798333]
- Sugiyama H, Tsuyuguchi T, Sakai Y, Mikata R, Yasui S, Watanabe Y, et
al. Current status of preoperative drainage for distal biliary obstruction.
World J Hepatol 2015; 7:2171-2176. [PMID: 26328029]
- Arkadopoulos N, Kyriazi MA, Papanikolaou IS, Vasiliou P, Theodoraki
K, Lappas C, et al. Preoperative biliary drainage of severely jaundiced
patients increases morbidity of pancreaticoduodenectomy: results of a
case-control study. World J Surg 2014; 38:2967-2972. [PMID: 24952079]
- Lai EC, Mok FP, Fan ST, Lo CM, Chu KM, Liu CL, et al. Preoperative
endoscopic drainage for malignant obstructive jaundice. Br J Surg 1994;
81:1195-1198. [PMID: 7741850]
- Fang Y, Gurusamy KS, Wang Q, Davidson BR, Lin H, Xie X, et al.
Meta-analysis of randomized clinical trials on safety and efficacy of
biliary drainage before surgery for obstructive jaundice. Br J Surg 2013;
100:1589-1596. [PMID: 24264780]
- Sewnath ME, Karsten TM, Prins MH, Rauws EJ, Obertop H, Gouma DJ.
A meta-analysis on the efficacy of preoperative biliary drainage for tumors
causing obstructive jaundice. Ann Surg 2002; 236:17-27. [PMID: 12131081]
- Scheufele F, Aichinger L, Jäger C, Demir IE, Schorn S, Sargut M, et al. Effect
of preoperative biliary drainage on bacterial flora in bile of patients with
periampullary cancer. Br J Surg 2017; 104:e182-e188. [PMID: 28121036]
- van der Gaag NA, Rauws EA, van Eijck CH, Bruno MJ, van der Harst E,
Kubben FJ, et al. Preoperative biliary drainage for cancer of the head of
the pancreas. N Engl J Med 2010; 362:129-137. [PMID: 20071702]
- Oncoline. Pancreascarcinoom 2011. <https://www.oncoline.nl/pancreascarcinoom>
- Tol JA, van Hooft JE, Timmer R, Kubben FJ, van der Harst E, de Hingh
IH, et al. Metal or plastic stents for preoperative biliary drainage in
resectable pancreatic cancer. Gut 2015; 65:1981-1987. [PMID: 26306760]
- Song TJ, Lee JH, Lee SS, Jang JW, Kim JW, Ok TJ, et al. Metal versus
plastic stents for drainage of malignant biliary obstruction before
primary surgical resection. Gastrointest Endosc 2016; 84:814-821.
[PMID: 27109456]
- Gardner TB, Spangler CC, Byanova KL, Ripple GH, Rockacy MJ,
Levenick JM, et al. Cost-effectiveness and clinical efficacy of biliary
stents in patients undergoing neoadjuvant therapy for pancreatic
adenocarcinoma in a randomized controlled trial. Gastrointest Endosc
2016; 84:460-466. [PMID: 26972022]


