Keywords
Percutaneous Transluminal Coronary Angioplasty (PTCA); ST segment elevation myocardial infarction; Learning curve; Trans-radial PTCA; Trans-femoral PTCA
Introduction
Percutaneous transluminal coronary angioplasty (PTCA) through femoral route was first successfully done in 1977 and only 12 years later [1], in 1989, Campeau first reported a series of 100 diagnostic coronary angiography by radial approach using 5 F catheters [2]. In early 1990, Kiemeneij and Laarman performed balloon angioplasty and stenting through radial artery [3] and in the access study, Kiemeneij et al. showed that there are no significant differences between any of the three tested approaches in terms of success of coronary angiography or angioplasty or duration of procedure [4]. But, despite wide recognition trans-radial artery PTCA has not received greater acceptance compared to femoral access. Several reasons have been cited for this, of which most common is the challenges encountered during the learning curve of the trans-radial approach.
With the growing evidence of mortality benefit in patients of Acute Coronary Syndrome (ACS) undergoing primary PCI [5-8], it may be considered necessary for all interventional cardiologist to perform angioplasty through trans-radial approach in the future.
However, with the advent of better guiding catheters and insight into the procedure we hypothesized that any trained femoral access operator can easily perform angiography and coronary interventions by trans-radial route and probably the learning curve for radial approach may not be as steep as generally thought.
Methods
Study design
The present study is a prospective, 6 months longitudinal study with 30 days follow up outcomes conducted in the Department of Cardiology, All India Institute of Medical Sciences, New Delhi, India. The study duration was from August 2015 to January 2016. A total of 30 consecutive patients of acute STEMI were enrolled to participate in the study. All patients were thoroughly evaluated for indication of primary PTCA and were offered primary PTCA within the window period. The aim of the study was to assess the difficulties associated with learning of the trans radial coronary PCI by operators who are trained and regularly performing trans femoral coronary PCI in terms of procedural success rate, cross over rate to femoral route, 30 days mortality and procedural complication rate.
Study population
We enrolled patients (>18 years of age) who presented in AIIMS emergency department with complaints of chest pain (window period of 12 hours) and a primary diagnosis of Acute ST Elevation Myocardial Infarction (STEMI). Patients who presented to us after >12 hours were included only when if they have one the following features–ongoing chest pain, development of new electrocardiographic changes or development of hemodynamic compromise. Patients who have already received thrombolytic therapy for STEMI were excluded from the study. All patients were taken for primary PCI after taking an informed consent. The procedure was well explained to the relatives and the patients.
Study procedure
Right radial artery was selected as the access in all cases of primary PTCA of the study. Modified Allen’s test was performed prior to radial artery access. Radial artery access was achieved with transradial kit (AVANTI®+of Cordis containing 21 G metal puncture needle with a compatible short metallic straight tip guide-wire and introducer sheath of 6 F in diameter) under local aesthesia. Right radial artery access was successful in all cases except in one case that was in cardiogenic shock and was crossed over to the femoral artery route. Vasodilator cocktail in the form of 200 micrograms of nitro-glycerine with 5000 units of unfractionated heparin along with 5 mg of Diltiazem were used intra-arterially through the accessed radial artery to prevent radial artery spasm.
ECG was used to localize infarct related artery (IRA) and the first coronary catheter selected was that left or right coronary guiding catheter which was suggested by ECG. All patients were given drug eluting stents (Endeavor sprint). Unfractionated heparin was used during the procedure with monitoring of activated clotting time. Use of GpIIb/IIIa inhibitors was with compelling indications only. After completion of PTCA of IRA, left or right diagnostic coronary catheter was used for angiogram of non- IRA. An 0.35 teflon coated exchange length guide-wire was used for exchange of coronary catheters to minimize the radial artery spasm and injury related to catheter manipulation. Sheaths were removed immediately after the completion of the procedure and haemostasis was achieved with radial artery band. Patients were monitored thoroughly during and after the procedure. Procedural success was defined as achievement of TIMI 2 or TIMI 3 flow in the infarct related artery after PTCA.
Study outcomes
Patients were evaluated for improvement in symptoms and TIMI flow pre-and post-procedure. Note was made for any complication during and after the procedure and also at follow up at 1 month. Radial artery color doppler was done if any access site complication noted. We also recorded mortality at 0 and 30- day post procedure.
Statistical analysis
Data was collected on structured proforma and managed on Microsoft Excel spread sheet. The correctness of entries was checked and mistakes and omission were rectified. Descriptive statistic was used and the results were presented as numbers, percentage, mean and SD (standard deviation). Statistical processing and analysis were performed using SPSS v22.0 software.
Ethical consideration
Written informed consent was obtained from the patients at the time of enrolment. This study was part of ongoing primary PCI registry in department of cardiology of All India Institute of Medical Sciences, New Delhi, India which is already ethically approved by institutional ethical committee.
Results
The study was done on 30 patients who presented in emergency department with a diagnosis of STEMI and who underwent primary PCI via radial artery access. Baseline characteristics of patients are shown in Table 1. Out of 30 patients there were 20 males and 10 females with a mean age of 56 ± 11.87 years. Major risk factor consisted of hypertension (43.3%), smoking (27%), obesity (27%), diabetes (20%) and dyslipidaemia (20%). Mean window period at the time of presentation was 6.87 ± 1.97 hrs, 23 of 30 patients (77%) were in Killip class I and 6 patients were in class II (20%). Only 1 patient (3%) was in cardiogenic shock who required an IABP insertion and was later cross over to femoral access PCI.
| Characteristics |
Values |
| Total number of patients (n) |
30 |
| Mean Age (in years) |
56 ± 11.87 |
| Sex ratio (M:F) |
20:10 |
| Hypertension (n) |
13 (44.33%) |
| Smokers (n) |
8 (27%) |
| Obesity (n) |
8 (27%) |
| Diabetes (n) |
6 (20%) |
| Dyslipidemia (n) |
6 (20%) |
| Window Period (hrs) |
6.87 ± 1.97 |
| Killip class |
| Class I |
23 (77%) |
| Class II |
6 (20%) |
| Class III |
0 |
| Class IV |
1 (3%) |
Table 1: Baseline patient characteristics.
Most of the patients suffered an anterior wall STEMI (57%) and rest had an inferior wall MI (43%) (Figure 1) (Table 2). Patients with anterior STEMI had left anterior descending coronary artery (LAD) as IRA and patients with inferior wall STEMI was involved of either right coronary artery (RCA) (27%) or left circumflex (LCx) coronary artery (17%) as IRA (Figure 2) (Table 2). Average Door to balloon time was 35.33 ± 5.89 minutes. Most of the patients on presentation had TIMI 0/1 flow in IRA (27/30; 90%) (Figure 3).
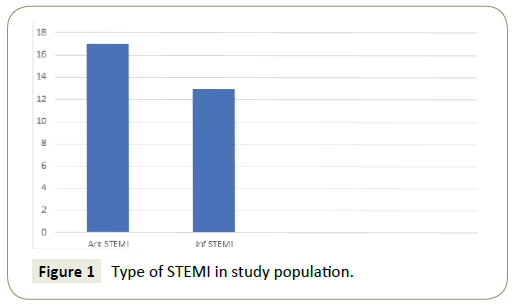
Figure 1: Type of STEMI in study population.
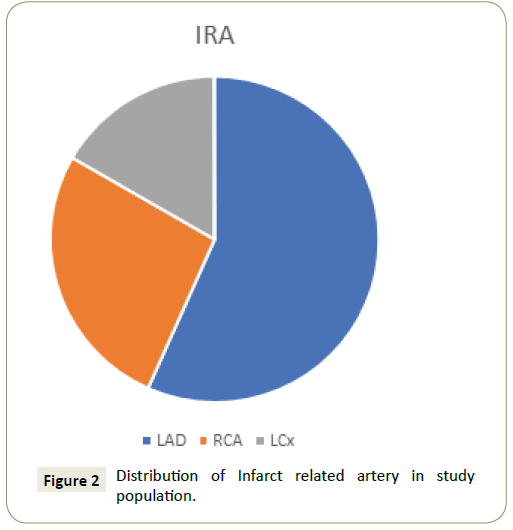
Figure 2: Distribution of Infarct related artery in study population.
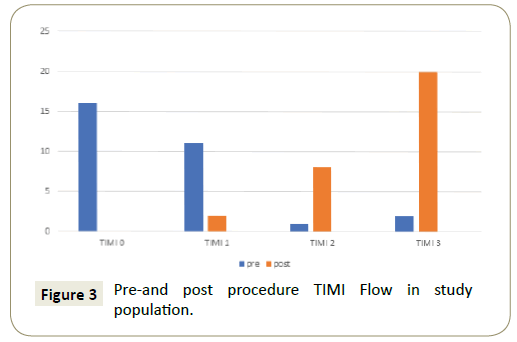
Figure 3: Pre-and post procedure TIMI Flow in study population.
| Characteristics |
n (%) |
| Anterior STEMI (n) |
17 (57%) |
| Inferior STEMI (n) |
13 (43%) |
| Infarct related artery |
| LAD (n) |
17 (57%) |
| RCA (n) |
8 (27%) |
| LCx (n) |
5 (16%) |
| TIMI flow (Pre-PTCA) |
| 0 |
16 (53%) |
| 1 |
11 (37%) |
| 2 |
1 (3%) |
| 3 |
2 (7%) |
| Mean no. of stents used per case |
1 |
| Mean diameter of stent used (in mm) |
3.05 ± 0.3 |
| Mean length of stent used (in mm) |
27.13 ± 3.11 |
Table 2: Procedure related characteristics.
PTCA was done successfully through trans-radial route in all the patients except one who was in cardiogenic shock and required IABP insertion. Most of the patients achieved a TIMI 2/3 flow (28/30; 93%) (Figure 3) (Table 3).
| Characteristics |
Values |
| Door-to-Balloon time (minutes) |
35.33 ± 5.89 |
| Procedural success |
93.40% |
| MI |
0 |
| Stroke |
0 |
| Number of deaths |
1 |
| Local site complications |
0 |
| Cross-over from radial to femoral |
1 |
| Bleeding complications |
0 |
| Radial artery stenosis |
1 (3.33%) |
| TIMI flow (Post-PTCA) |
| 0 |
0 |
| 1 |
2 (6.7%) |
| 2 |
8 (26.7%) |
| 3 |
20 (66.7%) |
| Duration of hospitalization (in days) |
4.3 ± 0.81 |
| 30-day mortality |
0 |
Table 3: Procedural outcomes.
There was one death due to cardiogenic shock and not related to the procedure. None of the patient developed local site complications or bleeding complications. As we routinely hospitalize patients of acute STEMI for 4-5 days, the total duration of hospitalization was 4.3 ± 0.81 days in the study (Table 3) (Figure 4).
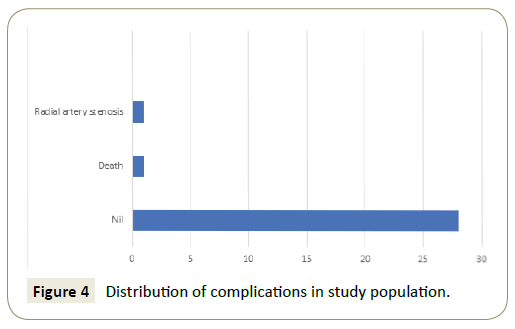
Figure 4: Distribution of complications in study population.
There was no mortality at 30-day follow-up in the study.
Discussion
Choice of arterial access site is an important debatable issue while performing percutaneous trans-luminal coronary angioplasty. Those practicing trans-femoral approach feel to remain attached to it as they see no major advantage of transradial interventions. Also, the steep learning curve described for trans-radial interventions make them comfortable with femoral approach.
The major huddles that have been considered as contributors towards steep learning curve for operators are difficulty in having access of radial artery, radial artery spasm, loops and bends in the course of catheter, prolongation of procedure time and associated increased radiation exposure.
The major advantage of avoiding the trans-femoral route is the freedom from local site complications which may prolong hospitalization because of blood transfusion or some additional diagnostic and therapeutic procedures. Trans-radial route has major advantage in this regard as it avoids the journey of coronary wires and catheters through the mysterious abdominal magic box.
Over and above that, some recent trials and meta-analysis have shown mortality benefit of trans-radial coronary angioplasty in setting of acute ST elevation myocardial infarction.
In our current study, we tried to evaluate the difficulties and problems faced by operators and team performing trans-radial primary coronary angioplasty in acute STE-MI that were trained and experienced in trans-femoral coronary angioplasty in both elective and primary situation.
We studied 30 patients of acute STE-MI over a period of 6 months and performed trans-radial primary coronary angioplasty. Studies evaluating radial artery approach for primary PCI in early part of last decade demonstrated excellent success rates with no access site complications [9-12].
We achieved 93.4% procedural success rate that was based on achievement of TIMI grade II to III flow. Moreover, subgroup analysis from the largest randomized trial comparing trans-radial and trans-femoral approach demonstrated significant reduction in primary end point (the composite end point of death, MI, stroke, or non-CABG bleeding at 30 days) and most importantly, reduction in mortality as well [13].
A meta-analysis showed that access site crossover rates were higher with trans-radial approach and with trends towards higher failure rates observed among less experienced interventionists highlighting the importance of learning curve and experience for trans-radial procedures [14]. However, we encountered only one cross-over from radial to femoral route along with one death that occurred in same patient that presented to us in cardiogenic shock. Only one patient presented to us with asymptomatic radial artery stenosis detected by color Doppler at follow-up. Mean duration of hospitalization was 4.3% ± 0.81%.
Inadequate arterial puncture and radial artery spasm have accounted for most failures during the initial cases [15]. During the entire study duration, we did not face any difficulty in negotiating the catheters one after the other through the trans-radial route. This could be because of 0.35 teflon coated exchange length guide-wire that we used in every case as a novel step. This might have avoided the radial artery spasm. We also selected only two catheters (one guiding and one diagnostic) for the whole procedure in each case. This was the novel step that we planned to minimize the Door-to-Balloon time and radial artery spasm. Studies have demonstrated variable learning curves with an early study showing lower procedure time and fluoroscopy time with higher success rates for operators after first 20 cases [16]. The threshold for overcoming learning curve based on data from NCDR registry has been proposed to be ~30- 50 cases [17]. However, no guidelines specify minimum numbers of trans-radial procedures for technical proficiency. Here we describe high success rates for trans-radial interventions right from the beginning for operators traditionally trained in transfemoral interventions. More remarkable is the fact that technical proficiency was achieved in high risk cases of acute myocardial infarction which have traditionally been associated with steep learning curve.
Total all cause in hospital mortality for primary PCI through transfemoral route in our center is 12.9%. Those who have STEMI with cardiogenic shock had in hospital mortality of 66.7% and those who have STEMI without cardiogenic shock had in hospital mortality of 2.6% when primary PCI was done through transfemoral route in our center. Local vascular complication and MACCE rates were 2.7% and 13.5% when primary PCI through transfemoral route is done our center for STEMI [18].
One of the major limitations of our study was that it was performed in the patients of STEMI undergoing primary PTCA but this could be advantage of the study because there are emerging evidences of mortality benefit in this group with trans-radial PTCA as compared to trans-femoral PTCA.
Also, we have not documented the procedure time, radiation exposure and contrast volume used. However retrospective analysis showed that they were not different from their contemporary trans-femoral route primary PTCA. And, as the study was done in emergency primary PTCA group of STEMI, we should not compare these variables with the routine trans-radial or trans-femoral route PTCA.
We hope that data from present study will promote the mindset of an interventional cardiologist for a “radial first” strategy even in high risk situations of acute myocardial infarction.
Conclusion
We concluded that the percutaneous transluminal coronary angioplasty (PTCA) through radial route is not difficult for operators trained and practicing with trans-femoral route. Although our data is exclusively from primary PTCA in STEMI but can be applicable to the routine elective PTCA also.
The low cost needed to treat patients with bifurcation coronary lesions using one stent is of utmost importance in developing countries, where hospitals have limited financial resources.
In the developing countries with limited financial resources; we can cut the cost by using one stent for many bifurcation coronary artery lesions without sacrificing the best outcome.
Conflict of Interest
The authors report no relationships that could be constructed as conflict of interest.
References
- King SB III, Schlumpf M, Spencer B (1993) Ten year completed follow-up of percutaneous transluminal coronary angioplasty: The early Zurich experience. J Am Coll Cardiol 22: 353-360.
- Campeau L (1989) Percutaneous radial artery approach for coronary angioplasty. Cathet Cardiovasc Diagn 16: 3-7.
- Kiemeneij F, Laarman GJ (1993) Percutaneous transradial approach for coronary stent implantation. Cathet Cardiovasc Diagn 30: 173-178.
- Kiemeneij F, Laarman GJ, Odekerken D, Slagboom T, Van der WR (1997) A randomized comparison of percutaneous transluminal coronary angioplasty by the radial, brachial and femoral approaches. The access study. J Am Coll Cardiol 29: 1269-1275.
- Romagnoli E, Zoccai GB, Sciahbasi A, Luigi P, Stefano R, et al. (2012) The RIFLE-STEACS (Radial versus femoral randomized investigation in ST-segment elevation acute coronary syndrome) study. J Am Coll Cardiol 60: 481-489.
- Bernat I, Horak D, Stasek J, Mates M, Pesek J, et al. (2014) ST-segment elevation myocardial infarction treated by radial or femoral approach in a multicenter randomized clinical trial. The STEMI-RADIAL trial. J Am Coll Cardiol 63: 964-972.
- Valgimili M, Gagnor A, Calabro P, Frigoli E, Leonardi S, et al. (2015) Radial versus femoral access in patients with acute coronary syndrome undergoing invasive management: A randomized multicentre trial. Lancet 385: 2465-2476.
- Ando G, Capodanno D (2015) Radial versus femoral access in invasively managed patients with acute coronary syndrome: A systematic review and meta-analysis. Ann Intern Med 163: 932-940.
- Kim MH, Cha KS, Kim HJ, Kim SG, Kim JS, et al. (2000) Primary stenting for acute myocardial infarction via the trans-radial approach: A safe and useful alternative to the trans-femoral approach. J Invasive Cardiol 12: 292-296.
- Mulukutla SR, Cohen HA (2002) Feasibility and efficacy of transradial access for coronary interventions in patients with acute myocardial infarction. Catheter Cardiovasc Interv 57: 167-171.
- Louvard Y, Ludwig J, Lefevre T, Schmeisser A, Bruck M, et al. (2002) Transradial approach for coronary angioplasty in the setting of acute myocardial infarction: A dualcenter registry. Catheter Cardiovasc Interv 55: 206-211.
- Valsecchi O, Musumeci G, Vassileva A, Tespili M, Guagliumi G, et al. (2003) Safety, feasibility and efficacy of transradial primary angioplasty in patients with acute myocardial infarction. Ital Heart J 4: 329-334.
- Jolly SS, Yusuf S, Cairns J, Niemelä K, Xavier D, et al. (2011) Radial versus femoral access for coronary angiography and intervention in patients with acute coronary syndromes (RIVAL): A randomized, parallel group, multicentre trial. Lancet 377: 1409-1420.
- Jolly SS, Amlani S, Hamon M, Yusuf S, Mehta SR (2009) Radial versus femoral access for coronary angiography or intervention and the impact on major bleeding and ischemic events: A systematic review and metaanalysis of randomized trials. Am Heart J 157: 132-140.
- Ball WT, Sharieff W, Jolly SS, Hong T, Kutryk MJ, et al. (2011) Characterization of operator learning curve for transradial coronary interventions. Circ Cardiovasc Interv 4: 336-341.
- Hildick-Smith DJ, Lowe MD, Walsh JT, Ludman PF, Stephens NG, et al. (1998) Coronary angiography from the radial artery-experience, complications and limitations. Int J Cardiol 64: 231-239.
- Hess CN, Peterson ED, Neely ML, Dai D, Hillegass WB, et al. (2014) The learning curve for transradial percutaneous coronary intervention among operators in the united states: A study from national cardiovascular data registry. Circulation 129: 2277-2286.
- Dubey G, Verma SK, Bahl VK (2017) Primary percutaneous intervention for acute ST elevation myocardial infarction: Outcomes and determinants of outcomes: A tertiary care center study from north India. Indian Heart J 69: 294-298.

