Keywords
Guideline; Pancreatitis
Abbreviations
AIP autoimmune pancreatitis; ERCP endoscopic
retrograde cholangio-pancreatography; ICDC International Consensus
Diagnostic Criteria; JPS Japanese Pancreatic Society
INTRODUCTION
Autoimmune Pancreatitis (AIP) is a form of chronic
pancreatitis that often is difficult to distinguish from
malignancy of the pancreas. Unlike pancreatic malignancies however, AIP may respond to therapy with corticosteroids,
and has a strong association with other immune mediated
diseases and increased levels of immunoglobulin subclass
4 (IgG-4) [1]. AIP has been further classified as either type
1 or type 2 by the International Consensus Diagnostic
Criteria (ICDC), primarily by histological features [2].
Although AIP is primarily a pathologic diagnosis,
attempts have been made to clinically diagnose AIP using
criteria including the Japanese Pancreas Society (JPS-2006
[3], JPS-2011 [4]), Korean Criteria [5], Asian Criteria [6], and
Histology Imaging & Serology Other organ involvement and
Response to therapy (HISORt) [7]. The ICDC [2] represents
a consensus set of criteria produced by a multinational
group that could be used in both clinical and research
practice. The ICDC [2] describes five cardinal features of AIP including (1) pancreatic imaging of the parenchyma (P)
with computerized tomography scan/magnetic resonance
imaging (CT/MRI) or pancreatic ductal imaging (D) with
endoscopic retrograde cholangiopancreatography/
Magnetic resonance cholangiopancreatography (ERCP/
MRCP), (2) serology (S) with (serum IgG-4 levels), (3) other
organ involvement (OOI), (4) histology of the pancreas (H),
and (5) response to corticosteroid therapy (Rt).
Unlike older criteria (JPS-2006 [3], Korean Criteria [5],
Asian Criteria [6], HISORt [7], ICDC [2] does not require
typical pancreatic imaging (CT/MRI/ERCP/MRCP) in order
to make the diagnosis of AIP. Instead, multiple avenues can
be taken to make the diagnosis, depending on available
histology, response to corticosteroid therapy, or pancreatic
imaging. Typically, parenchymal imaging is reviewed and
categorized as either typical (level 1) or atypical (level 2)
for AIP. Depending on which level of evidence is present,
the requirements for supporting data vary.
The real world clinical utility of ICDC [2] remains
unclear, especially when analyzing patient information
retrospectively, as all the clinical-radiological components
necessary to confirm a diagnosis may not be available
[8]. A recent large multicenter evaluation of the ICDC [2]
guidelines favorably validated their use, but used data
from clinical centers that were initially involved in the
development of the guidelines, possibly contributing to a
study bias [9]. A separate validation study that compared
Asian [6], HISORt [7], and ICDC [2] guidelines in diagnostic
capabilities however concluded that these guidelines
should not be used as the gold standard in diagnosis of AIP
[10].
In our independent validation study, we aim to apply
the criteria set forth by the ICDC [2] to a cohort of patients
with AIP from a single institution who had been diagnosed
and managed as having AIP in routine clinical practice
during the decade leading up to the implementation of
ICDC [2] guidelines. We aim to identify the accuracy, ease
of application, and potential shortcomings of the ICDC [2].
For comparison, this same patient cohort is also evaluated
using other diagnostic criteria (JPS 2006 [3], Korean
Criteria [5], Asian Criteria [6], HISORt [7], and JPS 2011
[4]) to identify factors that may contribute to increased
accuracy for the diagnosis of AIP, with focus on patients
who were unclassifiable per ICDC [2] guidelines.
MATERIALS AND METHODS
We enrolled 51 patients who were evaluated and
treated with the clinical diagnosis of AIP, between 2001
and 2012 at a single institution Pancreas Clinic prior to
the development and publication of the ICDC guidelines.
AIP diagnosis was made based on a combination of clinical
features including obstructive jaundice and abdominal
pain, and where available, serological evidence including
increased levels of IgG-4, radiology with CT or MRI findings
demonstrating diffuse or focal enlargement of the pancreas,
and histological specimens (both surgical resection and
pancreatic biopsy), as per the evolving understanding of this disease during this time period. Enrollment in the
AIP cohort was made based on a combination of clinical
evaluation, histology, and also included multidisciplinary
review with gastroenterology, radiology, and surgery
subspecialties. While acknowledging the presence of
incomplete clinical and investigative studies available
during each patient’s workup, we then evaluated each
patient who was enrolled in this cohort using the ICDC
guidelines. Using the ICDC, our cohort of patients was
diagnosed and categorized with as either definitive
type 1 AIP, probable type 1 AIP, definitive type 2 AIP,
or unclassifiable. We sought to apply the ICDC criteria
to our cohort in the least invasive method, preferring to
use parenchymal imaging and serology where possible
to make the diagnosis. Radiology films were formally rereviewed
by a team of radiologists who read each film as a
group, allowing for discussion of each radiographic finding
and whether or not it met diagnostic criteria for AIP [11].
The patients who were unclassifiable according to
ICDC were then identified. Clinical and investigative data
available for each of these unclassifiable patients was
assessed to see if the inability to confirm the diagnosis
of AIP was related to unavailable information. These
unclassifiable patients were then re-evaluated using other
diagnostic guidelines, to identify clinical-radiological
factors which allowed the diagnosis to be made with
certain criteria but not others.
We compared type 1, type 2, and unclassifiable
patients based on demographics (age, gender), clinical
presentation (obstructive jaundice, acute pancreatitis, or
any combination) and radiologic imaging (focal or diffuse
pancreatic involvement). T-test and chi-square analysis was
used with a p-value less than 0.05 being significant (SPSS
20, SPSS Inc, Chicago, IL). This study was approved by the
local Institutional Review Board.
RESULTS
Up to the time of publication of the ICDC guidelines
we enrolled 51 patients with a working diagnosis of AIP,
including 30 men and 21 women, with a mean age of 55.9
and range of 8-81 years (Table 1). After applying the ICDC
guidelines to this cohort we obtained the following results.

AIP Definitive Type 1 (Table 2 and Figure 1), from our
cohort of 51 patients, 33 patients (64.7%) were diagnosed
with definitive type 1 AIP. All 33 patients had level 1
pancreatic parenchymal imaging on CT; defined by the
ICDC as diffuse enlargement with delayed enhancement
sometimes associated with rim-like enhancement, or
presence of low-density mass within the pancreas. With
level 1 parenchymal imaging, patients require one other
type of evidence (either level 1 or level 2) from any of the
following: serology, histology, or other organ involvement.
Of the 33 patients, 28 were diagnosed with definitive
type 1 AIP with the addition of serological evidence, with
5 patients meeting level 1 serology (>2x upper limit of
normal value for serum IgG-4) and 23 patients meeting
level 2 serology (1-2x upper limit of normal value for serum
IgG-4). Of these 28 patients with level 1 parenchymal imaging and serological evidence, 10 patients also met OOI
criteria, and 12 patients had level 1 histology to confirm
their diagnosis of definitive type 1 AIP.
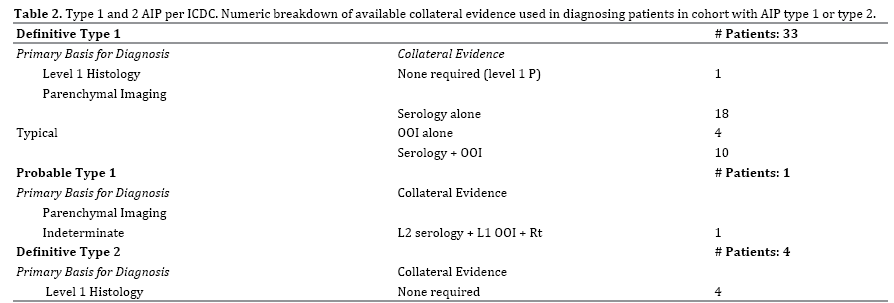
Figure 1. Evidence seen in patients with definitive type 1 AIP per ICDC. Venn diagram illustrating distribution of histology, other organ involvement, and
serology in patients with level 1 parenchymal imaging N=33.
H Histology; OOI Other Organ Involvement; S Serology
Four patients with level 1 pancreatic parenchymal
imaging had other organ involvement (OOI) alone to meet
diagnostic criteria. Other organ involvement includes
evidence based on radiology or histology. Three of the
four met level 1 evidence with radiological evidence:
segmental/multiple proximal (biliary/intrahepatic) bile
duct stricture, and the remaining one patient with level 2
radiological evidence: symmetrically enlarged salivary/
lacrimal glands. One patient was diagnosed with definitive
type 1 AIP with level 1 histology alone. The features met
by this patient on pancreatic core biopsy were periductal
lymphoplasmacytic infiltration without granulocytic
infiltration, obliterative phlebitis, and storiform fibrosis.
AIP Probable Type 1 (Table 2), one patient from our
cohort met ICDC diagnosis of probable type 1 AIP. To
be diagnosed with probable type 1 AIP a patient with
indeterminate/level 2 parenchymal imaging requires
a measurable response to steroids, defined as definite
improvement in imaging abnormalities or decrease in
Cancer Antigen 19-9 (CA 19-9 levels) plus level 2 evidence
from either serology, OOI, or histology. Our patient had level 2 parenchymal imaging (segmental/focal enlargement
of head and body of pancreas); along with a response to
steroids (rapid radiologically demonstrable resolution
and marked improvement in pancreatic/extrapancreatic
manifestations) plus level 2 serology. This same patient
also had level 1 other organ involvement (typical
radiological evidence: segmental/multiple proximal hilar/
intrahepatic bile duct stricture).
AIP Definite Type 2 (Table 2), ICDC diagnosed 4
patients from our cohort with definitive type 2 AIP. Unlike
type 1 AIP, the diagnosis of type 2 AIP using ICDC requires
histological confirmation. All 4 patients demonstrated level
1 histology confirmed IDCP (granulocytic infiltration of
duct wall with or without granulocytic acinar inflammation
plus absent or scant IgG-4-positive cells).
Clinical Features of Unclassifiable Patients by ICDC
From the original cohort of 51 patients, 13 patients
(25.4%) were unclassifiable using ICDC. Of the 13 patients,
6 (46%) presented initially with obstructive jaundice,
5 (38%) with acute abdominal pain and biochemical
pancreatitis without obvious risk factors for pancreatitis
(such as gallstones or alcohol), and the remaining 2
(15%) presented with pancreatic mass (Table 3). After
malignancy was ruled out in these patients on initial
evaluation and long-term follow up, diagnosis of AIP was
considered.
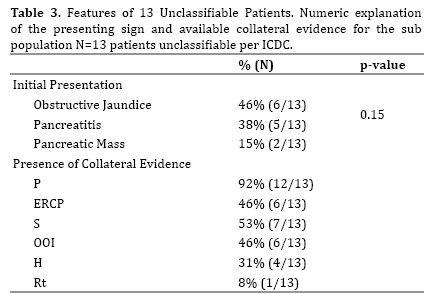
Parenchymal imaging was collected in 12 (92%)
patients (level 1: 1 patient, level 2/indeterminate: 10
patients, normal: 1 patient). ERCP was completed in 6
(46%) patients (level 1: 3 patients, level 2: 2 patients,
neither level: 1 patient). Serology was available in 7 (54%)
patients (level 1: 1 patient, level 2: 5 patients, normal:
1 patient). OOI was investigated in 6 (46%) patients,
with 5 meeting criteria based on radiological features
(level 1: 4 patients, level 2: 1 patient, neither: 1 patient).
A corticosteroid trial was completed in 1 (7%) patient
with documented improvement in parenchymal imaging.
Histology was available in 4 (30.7%) patients (level 2: 3
patients, neither level: 1 patient) (Table 3).
When the 13 unclassifiable patients were examined
using other diagnostic criteria, 6 (46%) patients could
be diagnosed with AIP by one or more of the non-ICDC
diagnostic criteria. JPS-2006 [3], Korean [5], and Asian
[6] guidelines classified the same 6 patients (46%) with
AIP. These three guidelines diagnosed patients with a
combination of imaging with serology or histology. The
HISORt [7] guidelines diagnosed 4 patients (31%) who
were unclassifiable per ICDC [2] by utilizing histological
features in 3 patients and combination of imaging and
serology in 1 patient. JPS-2011 [4] was able to diagnose 4
patients (31%) from the unclassifiable subset (Table 4).
In all 4 patients ERCP was paired with serology, OOI, or
histology.

Histology amongst Unclassifiable Patients
From our unclassifiable patients, 4 had histology data.
These 4 patients were initially evaluated for pancreatic malignancy given their initial clinical presentations of
obstructive jaundice, pancreatic mass, or acute pancreatitis.
Based on the 5 cardinal features outlined by the ICDC [2],
each of these 4 patients demonstrated features suggestive
of AIP.
Analysis of ICDC Unclassifiable Patients
Amongst unclassifiable patients Figure 2, we aimed
to identify whether patients did not meet ICDC [2]
diagnosis due to lack of available data or whether they had
available evidence and were still unable to meet ICDC [2]
requirements. We looked at the 13 unclassifiable patients
and compared the diagnostic ability of other criteria
(Table 4).
Figure 2. Comparison of Diagnostic Ability of Guidelines Applied to
Unclassified Patients. Venn diagram illustrating the diagnosis of patients
who were unclassifiable per ICDC N=13 using other diagnostic guidelines.
Using JPS-2006 [3], Korean [5], and Asian [6] guidelines,
6 of the unclassifiable patients (46%) could be diagnosed
with AIP. Combination of imaging (parenchymal or ductal)
plus serology was utilized to diagnose 4 of these patients.
Serology in these 4 patients met level 2 criteria (1 - 2x
the upper limit of normal IgG-4 level). The 2 remaining
patients could be diagnosed with combination of
imaging plus histology (periductal lymphoplasmacytic
infiltration). Histology is not differentiated between
level 1 and level 2 according to these guidelines, so
presence of lymphoplasmacytic sclerosing pancreatitis
(LPSP) without regard to additional features mentioned
by ICDC [2] (obliterative phlebitis, storiform fibrosis,
or presence of IgG-4 positive cells) fulfills histological
requirement.
The HISORt [7] guidelines diagnosed 4 patients
(31%) who were unclassifiable per ICDC [2]. Histology
alone was sufficient to diagnose 3 patients (periductal
lymphoplasmacytic infiltration without granulocytic
infiltrate). The remaining 1 patient was diagnosed with
combination of typical ductal imaging (long stricture of the
main pancreatic duct without upstream dilatation) plus
level 2 serology (IgG-4 level 1-2x upper limit normal). The
reason this patient did not meet ICDC [2] diagnosis is due
to indeterminate parenchymal imaging according to ICDC
[2] with absence of sufficient supporting evidence.
While JPS-2011 [4] could diagnose 4 patients in our
cohort that ICDC [2] could not, 3 of those cases (75%) necessitated ERCP as JPS-2011 [4] requires ERCP in all
patients with level 2 parenchymal imaging. The requirement
of ERCP in cases of indeterminate parenchymal imaging is
to avoid misdiagnosis of pancreatic cancer [4]. In these 3
patients, ERCP findings were paired with combination of
serology, OOI, or histological features to diagnose AIP. The
remaining 1 patient had no parenchymal imaging available,
however had typical ERCP findings for AIP along with level
2 histological features (periductal lymphoplasmacytic
infiltrate without granulocytic infiltration plus storiform
fibrosis). 7 patients (13.7%) were unable to be diagnosed
with AIP by any of the discussed criteria due to
unavailable data.
Statistical Analysis
There was no statistically significant difference
between both classifiable and unclassifiable patients in
terms of patient demographics, clinical presentation and
radiologic imaging. However, all patients who presented
with combination of acute pancreatitis, obstructive
jaundice, and pancreatic mass were diagnosed with AIP
per ICDC [12, 13].
DISCUSSION
We present a retrospective validation study for the
ICDC [2] guidelines using a prospectively collected cohort
of 51 North American patients followed clinically from
2000 - 2012 prior to the publication of ICDC [2]. Our patient
cohort has a similar age range and gender distribution
at diagnosis (56.4 years and 61.5 years for type 1 and
type 2, respectively) (Table 1) when compared to other
previously published large studies [9, 14]. A previously
published study that examined a North American cohort
reported a slightly older average age on presentation of 63
years for type 1 patients, with majority (83%) being male
[15].
A suggested benefit of the ICDC [2] guidelines is the
flexibility allowed in the diagnostic evaluation of patients;
the diagnosis of AIP can be made through a variety of
pathways. For example, typical pancreatic parenchymal
imaging can be paired with data from serology, radiology,
histology, or response to steroid therapy [16]. In the event
parenchymal imaging is atypical or indeterminate, the
diagnosis of AIP is still possible with a separate combination
of data. This is important because patient presentation is
not uniform and diagnostic criteria that allow for flexibility
are favorable in clinical practice, especially if designed
for use in primary care settings. Another advantage of
ICDC [2] is that unlike JPS-2011 [4], ICDC [2] does not
necessitate ERCP in cases with atypical parenchymal
imaging, further supporting the use of ICDC [2] amongst
primary care physicians. Though not required, ductal
imaging can serve a complementary role in the diagnosis
if available. However, as seen in our cohort, ERCP did not
assist in diagnosis of any patient in our cohort. ICDC [2]
also recognizes AIP as the pancreatic manifestation of
IgG-4-related disease and as such recognizes the other
organs associated with IgG-4-related disease as supportive
evidence for diagnosing AIP, such as biliary strictures,
retroperitoneal fibrosis, and sialadenitis. IgG-4-related
disease can involve nearly every organ system, and as
such recognition of AIP requires awareness of the possible
array of other organ involvement [17].
While several prior studies have found that ICDC [2]
had superior diagnostic sensitivity, this current study is
not as supportive of the utility and diagnostic capability of ICDC [2]. In one such study, five major diagnostic
guidelines (ICDC [2], Korean [5], Japanese-2011 [4], Asian
[6], and HISORt [7]) were evaluated using a Japanese
cohort of patients with AIP, revealing that ICDC [2] had
the greatest sensitivity [18]. Similarly, a Taiwanese [19]
cohort was analyzed using ICDC [2], HISORt [7], and Asian
[6] criteria, and again ICDC [2] was found to have superior
sensitivity. In a third study involving an Japanese cohort
of 110 Japanese patients with AIP treated between 1992
and 2013, ICDC [2] demonstrated superior accuracy (95%
diagnosis) compared to JPS 2006 [3], Asian [6], HISORt
[7], ICDC [2], and revised JPS 2011 criteria [4]. While ICDC
[2] had the highest accuracy for diagnosis, they concluded
that ICDC [2] was intended for experts of pancreatology
and JPS-2011 [4] on the other hand was more compatible
for general internists. The reasons cited against ICDC [2]
included the disregard for country specific diagnostic
criteria, given ICDC [2] was meant to be used globally. Also,
the use of different levels (level 1 and level 2) of evidence,
may result in complicating the process of diagnosis [4].
A North American cohort at a large U.S. center
evaluated 26 patients with AIP and reported that
diagnostic guidelines including HISORt [7], JPS 2006
[3], and Korean [5] guidelines were satisfied for the
diagnosis of AIP in 85% of cases, suggesting that various
guidelines serve complementary roles [20]. This study did
not compare the guidelines for superiority in diagnostic
capabilities. Similarly in a Dutch [10] study, 114 patients
with AIP were re evaluated using Asian [6], HISORt [7],
and ICDC [2] guidelines. In this study, 82% satisfactorily
met at least one of these guidelines for diagnosis of AIP
suggesting a complementary role amongst guidelines. The
remaining 18% unable to be diagnosed using any of the
three diagnostic guidelines. In another Italian study [21],
92 patients with AIP were re-evaluated with ICDC [2]. Of
the 92 patients, 15 patients (16%) were classified as not
otherwise specified. This study further concluded that
patients who were deemed not otherwise specified were
classified as such despite having many features that were
similar to patients classified as type 1 or type 2 AIP.
To our knowledge our study is the only North American
study to evaluate a cohort of patients with clinically
diagnosed AIP with application of multiple guidelines
including ICDC [2]. Unlike the international studies
discussed above [4, 18, 19], ICDC [2] sensitivity (74.5%)
was not superior (38/51 patients with either type 1 or
type 2 AIP) relative to clinical diagnosis, which served
as the gold standard. A significant barrier to diagnosis
using ICDC [2] guidelines amongst our cohort was the
distinction between level 1 and level 2 evidence. We often
encountered patients who clinically were diagnosed and
treated as having AIP, however could not be classified as
having level 1 histology or other organ involvement due to
the absence of a single feature. This detail also explains why
JPS 2006 [3], Korean [5], and Asian [6] guidelines could
each diagnose a larger proportion of our cohort, as these
guidelines do not distinguish between level 1 and level 2 evidence. When using all guidelines together, 44 patients
(86%) could be diagnosed with AIP, suggesting that using
multiple guidelines can serve a complementary function.
Ductal imaging is not required for the diagnosis of
AIP per ICDC [2] guidelines. Instead, ERCP can be used as
supportive evidence, especially when parenchymal imaging
is indeterminate. Though not mandatory, ductal imaging
can help to differentiate between AIP and pancreatic
cancer. In a comparison of ERCP features amongst AIP and
pancreatic cancer patients, it was noted that obstruction
of the main pancreatic duct and skipped main pancreatic
duct lesions were far more typical of AIP than pancreatic
cancer [22]. However, if parenchymal imaging is highly
suggestive of AIP then ductal imaging may not be necessary
at all. Amongst our cohort, 13 patients had parenchymal
imaging meeting indeterminate evidence for AIP, of which
8 underwent ERCP. Of these 8 patients, 3 demonstrated
significant strictures of the main pancreatic duct, which is
highly suggestive of AIP per multiple studies [2, 22]. The
inclusion of ERCP in the ICDC guidelines is unnecessary
as seen in our cohort, as all patients could be diagnosed
without ERCP. From our cohort of 51 patients with AIP, 34
(67%) patients underwent ERCP as part of their evaluation
and the ERCP findings in these patients did not contribute
to diagnosis in any patient. Furthermore, diagnostic
ERCP is used less frequently in North America and the
justification for performing pancreatic ductal imaging in
the evaluation of AIP is not clear in our cohort.
Histology is required in diagnosing type 2 AIP. Several
methods for obtaining tissue in evaluation of pancreatic
masses are available, including ERCP with papillary biopsy;
CT guided percutaneous core biopsy, and endoscopic
ultrasound (EUS) with fine needle aspiration (FNA), all of
which carry favorable safety and diagnostic profiles [23, 24]. However, the diagnostic utility and indications for
performing these studies remain unclear in evaluation
of patients with CT/MRI findings suggestive of AIP. Thus
unnecessary procedures are performed. In one European
study evaluating 29 patients with ICDC [2] diagnosed AIP,
it was noted that a total of 50 ERCP and 18 EUS procedures
were performed, with retrospective analysis concluding
that only 20 ERCPs and 4 EUS procedures could be
justified. Additionally, 8 patients (23%) were referred to
surgery that could not be justified [25].
EUS with FNA has been evaluated in several cohorts of
patients who had CT or MRI imaging findings suggestive of
AIP. In one such study, tissue collected using EUS with FNA
diagnosed 45 out of 78 patients (57.7%) with AIP using
ICDC guidelines [26]. There is disagreement however,
with additional studies either supporting or refuting the
use of EUS with FNA as an effective diagnostic tool, citing
favorable and unfavorable sensitivities [27, 28].
Histology, though mandatory for diagnosing type 2
AIP, provided no additional supportive data in our type
1 patients. Amongst type 1 patients, 27 of 34 patients
(79%) had histology available, with 20 cases yielding evidence (level 1: 13 patients, level 2: 7 patients). Amongst
unclassifiable patients, 4 out of 13 patients (31%) had
histology collected, with 3 patients yielding level 2
evidence. However, regardless of level 2 histology findings,
these patients remain unclassifiable per ICDC [2].
We believe that diagnostic guidelines including ICDC
[2] should acknowledge that spontaneous relapsing and
remitting symptoms or imaging features without steroid
therapy are characteristic of an inflammatory etiology and
favor the diagnosis of AIP over pancreatic malignancy. AIP
has been linked with high serum level of immune complexes
which favors the idea that complement activation is
involved at least during relapses [29]. Lack of consideration
of patients who show spontaneous improvement in
symptoms, imaging, or serology without corticosteroid
therapy became evident amongst our cohort when we
noted 1 patient who had this distinct feature. This patient,
who presented with obstructive jaundice and pancreatic
mass, was found to have typical parenchymal imaging
for AIP, level 1 OOI, and benign histology. Clinically this
patient was diagnosed and treated as AIP. However, the
patient showed spontaneous resolution in imaging and
symptoms without corticosteroid therapy, which lends
additional support against this patient having a malignant
process and instead more likely having an inflammatory
etiology. Had this patient been given steroids it may have
become difficult to distinguish whether remission was
spontaneous or corticosteroid induced.
There are several limitations to our current study. Our
study data was acquired during the clinical management
of each patient in the absence of the ICDC [2] guidelines.
Patients were diagnosed and treated with AIP based on
clinical evidence and without the utilization of ICDC [2],
and was thus free of selection bias. Given that our study
was retrospective, we utilized only the data that had been
collected during the course of clinical evaluation, which
may have been incomplete when applying the ICDC [2]
guidelines. For example, while IgG-4 levels were collected
in the majority of patients, they were not available for 11
patients (21.5%). The role of IgG-4 serology in patients
with AIP has been outlined to illustrate patients with AIP
have on average higher levels of serum IgG-4 compared
to unaffected patients [1]. Additional data not available
in all patients were ERCP and steroid trials, in 17 and 38
patients, respectively. With more data points available,
a more critical evaluation could be made regarding the
ICDC [2] guidelines. This limits the proper evaluation of
each cardinal feature of its contribution of the diagnostic
procedure in this cohort.
Another limitation of this type of study is the absence
of a gold standard pathologic diagnosis for all patients.
As such it is possible that some of our patients who were
unclassifiable using ICDC [2] may not have even had AIP, even
if more diagnostic data were available. While several studies
evaluating various diagnostic criteria have shown that ICDC
[2] has superior sensitivity [18, 19], up to 20% of patients
with AIP can be unclassified by any diagnostic criteria [10].
While the ICDC represents consensus understanding
and recommendations for diagnosing AIP, application in
our cohort provides an alternative impression [4, 18, 19].
We find that several features should be refined moving
forward including acknowledging that patients with AIP
can have waxing and waning of symptoms and clinical
features, identifying suitable justifications and indications
for invasive testing such as ERCP, and validation of
methods used for acquiring histologic data.
CONCLUSION
Furthermore, from our study it appears that utilizing
multiple diagnostic guidelines in complementary roles can
lead to more accurate diagnosis in patients with suspected
AIP. Future directions for study include comparison of
methods used to acquire histology and evaluation of the
utility of ERCP inclusion in the guidelines.
Conflict of Interest
The authors declare that they have no conflict of
interest.
References
- Hamano H, Kawa S, Horiuchi A, Unno H, Furuya N, Akamatsu T, et al. High serum IgG4 concentrations in patients with sclerosing pancreatitis. N Engl J Med 2001; 344:732-8. [PMID: 11236777]
- Shimosegawa T, Chari ST, Frulloni L, Kamisawa T, Kawa S, Mino-Kenudson M, et al. International consensus diagnostic criteria for autoimmune pancreatitis: guidelines of the International Association of Pancreatology. Pancreas 2011; 40:352-8. [PMID: 21412117]
- Okazaki K, Kawa S, Kamisawa T, Naruse S, Tanaka S, Nishimori I, et al. Clinical diagnostic criteria of autoimmune pancreatitis: revised proposal. J Gastroenterol 2006; 41:626-31. [PMID: 16932998]
- Maruyama M, Watanabe T, Kanai K, Oguchi T, Muraki T, Hamano H, et al. International Consensus Diagnostic Criteria for Autoimmune Pancreatitis and Its Japanese Amendment Have Improved Diagnostic Ability over Existing Criteria. Gastroenterol Res Pract 2013; 2013:456965. [PMID: 24348535]
- Kim KP, Kim MH, Kim JC, Lee SS, Seo DW, Lee SK, et al. Diagnostic criteria for autoimmune chronic pancreatitis revisited. World J Gastroenterol 2006; 12:2487-96. [PMID: 16688792]
- Otsuki M, Chung JB, Okazaki K, Kim MH, Kamisawa T, Kawa S, et al. Asian diagnostic criteria for autoimmune pancreatitis: consensus of the Japan-Korea Symposium on Autoimmune Pancreatitis. J Gastroenterol 2008; 43:403-8. [PMID: 18600383]
- Chari ST. Diagnosis of autoimmune pancreatitis using its five cardinal features: introducing the Mayo Clinic's HISORt criteria. J Gastroenterol 2007; 42:39-41. [PMID: 17520222]
- Frulloni L, Scattolini C, Falconi M, Zamboni G, Capelli P, Manfredi R, et al. Autoimmune pancreatitis: differences between the focal and diffuse forms in 87 patients. Am J Gastroenterol 2009; 104:2288-94. [PMID: 19568232]
- Hart PA, Kamisawa T, Brugge WR, Chung JB, Culver EL, Czakó L, et al. Long-term outcomes of autoimmune pancreatitis: a multicentre, international analysis. Gut 2013; 62:1771-6. [PMID: 23232048]
- van Heerde MJ, Buijs J, Rauws EA, de Buy Wenniger LJ, Hansen BE, Biermann K, Verheij J, et al. A comparative study of diagnostic scoring systems for autoimmune pancreatitis. Pancreas 2014; 43:559-64. [PMID: 24658319]
- Lee-Felker SA, Felker ER, Kadell B, Farrell J, Raman SS, Sayre J, et al. Use of mdct to differentiate autoimmune pancreatitis from ductal adenocarcinoma and interstitial pancreatitis. AJR Am J Roentgenol 2015; 205:2-9. [PMID: 26102377]
- Hart PA, Zen Y, Chari ST. Recent Advances in Autoimmune Pancreatitis. Gastroenterology 2015; 149:39-51. [PMID: 25770706]
- Ralli S, Lin J, Farrell J. Autoimmune pancreatitis. N Engl J Med 2007; 356:1586. [PMID: 17429095]
- Huggett MT, Tang K, Johnson GJ, Hatfield AR, Pereira SP, Webster GJ. Disease profile and long-term outcome of patients with autoimmune pancreatitis/IgG4 systemic disease. Gut 2011; 60:60.
- Chari ST, Smyrk TC, Levy MJ, Topazian MD, Takahashi N, Zhang L, et al. Diagnosis of autoimmune pancreatitis: the Mayo Clinic experience. Clin Gastroenterol Hepatol 2006; 4:1010-1016. [PMID: 16843735]
- Hart PA, Chari ST. Autoimmune pancreatitis. Pancreapedia: Exocrine Pancreas Knowledge Base 2013.
- Stone JH, Zen Y, Deshpande V. IgG4-related disease. N Engl J Med 2012; 366:539-51. [PMID: 22316447]
- Sumimoto K, Uchida K, Mitsuyama T, Fukui Y, Kusuda T, Miyoshi H, et al. A proposal of a diagnostic algorithm with validation of International Consensus Diagnostic Criteria for autoimmune pancreatitis in a Japanese cohort. Pancreatology 2013; 13:230-7. [PMID: 23719593]
- Chang MC, Liang PC, Jan IS, Yang CY, Tien YW, Wei SC, et al. Comparison and validation of International Consensus Diagnostic Criteria for diagnosis of autoimmune pancreatitis from pancreatic cancer in a Taiwanese cohort. BMJ Open 2014; 4:e005900. [PMID: 25138812]
- Raina A, Yadav D, Krasinskas AM, McGrath KM, Khalid A, Sanders M, et al. Evaluation and management of autoimmune pancreatitis: experience at a large US center. Am J Gastroenterol 2009; 104:2295-306. [PMID: 19532132]
- Ikeura T, Manfredi R, Zamboni G, Negrelli R, Capelli P, Amodio A, et al., Application of international consensus diagnostic criteria to an Italian series of autoimmune pancreatitis. United European Gastroenterol J 2013; 1:276-84. [PMID: 24917972]
- Takuma K, Kamisawa T, Tabata T, Inaba Y, Egawa N, Igarashi Y. Utility of pancreatography for diagnosing autoimmune pancreatitis. World J Gastroenterol 2011; 17:2332-7. [PMID: 21633599]
- Tyng CJ, Almeida MF, Barbosa PN, Bitencourt AG, Berg JA, Maciel MS, et al. Computed tomography-guided percutaneous core needle biopsy in pancreatic tumor diagnosis. World J Gastroenterol 2015; 21:3579-86. [PMID: 25834323]
- Voss M, Hammel P, Molas G, Palazzo L, Dancour A, O'Toole D, et al. Value of endoscopic ultrasound guided fine needle aspiration biopsy in the diagnosis of solid pancreatic masses. Gut 2000; 46:244-9. [PMID: 10644320]
- Manser CN, Gubler C, Müllhaupt B, Bauerfeind P. Unnecessary Procedures and Surgery in Autoimmune Pancreatitis. Digestion 2015; 92:138-46. [PMID: 26340740]
- Kanno A, Masamune A, Fujishima F, Iwashita T, Kodama Y, Katanuma A, et al. Diagnosis of autoimmune pancreatitis by EUS-FNA by using a 22-gauge needle based on the International Consensus Diagnostic Criteria. Gastrointest Endosc 2012; 76:594-602. [PMID: 22898417]
- Morishima T, Kawashima H, Ohno E, Yamamura T, Funasaka K, Nakamura M, et al. Prospective multicenter study on the usefulness of EUS-guided FNA biopsy for the diagnosis of autoimmune pancreatitis. Gastrointest Endosc 2016; 84:241-8. [PMID: 26777565]
- Jung JG, Lee JK, Lee KH, Lee KT, Woo YS, Paik WH, et al. Comparison of endoscopic retrograde cholangiopancreatography with papillary biopsy and endoscopic ultrasound-guided pancreatic biopsy in the diagnosis of autoimmune pancreatitis. Pancreatology 2015; 15:259-64. [PMID: 25891790]
- Muraki T, Hamano H, Ochi Y, Komatsu K, Komiyama Y, Arakura N, et al. Autoimmune pancreatitis and complement activation system. Pancreas 2006; 32:16-21. [PMID: 16340739]



