Keywords
Infant mortality; Health disparities; Community health education; Program evaluation
Introduction
Healthy People 2020 monitors Leading Health Indicators (LHIs) that reflect progress toward objectives pertaining to high-priority health issues in the United States [1]. The infant mortality rate is one such LHI. The Healthy People 2020 Objective for infant mortality is to improve the current national rate to 6.0 infant deaths per 1,000 live births. For progress to be made nationally, states must bring their infant mortality rates within reach of the HP2020 goals. Currently, the state of Mississippi experiences the highest infant mortality rate in the nation (9.3 infant deaths per 1,000 live births), a rate that reflects a 12.2% increase from the previous year, during a time when the nation’s rates are trending downward [2,3]. Furthermore, a large disparity exists in rates of infant mortality in Mississippi when stratified by race. The 12.2% increase over 2014 rates was due to a disparate 5.0% increase among Caucasian mothers and a 16.0% increase in infant mortality among African American mothers. The infant mortality rate among African Americans (13.0 infant deaths per 1,000 live births) was more than twice the infant mortality rate among Caucasians (6.2 infant deaths per 1,000 live births).
The determinants of infant mortality are well known (USDHHS, 2017) and include congenital malformations, preterm birth (infants born <37 weeks gestation) and low birth weight (infants born weighing <2500g), Sudden Unexplained Infant Death (SUID)/Sudden Infant Death Syndrome (SIDS), maternal pregnancy complications and accidents and injuries [4,5].
In Mississippi, 2015 data reflect that approximately one half of all infant deaths occur on the first day of life, one-fourth occur during the neonatal period (1-28 days of life) and the remaining one-fourth of deaths occur in the post-neonatal period (>28 days - 365 days of life) [2]. The leading cause of infant mortality in Mississippi is a combination of premature birth and low birth weight. Although only two percent of births are classified as Very Low Birth Weight (infants weighing <1500 g at birth), these premature infants represent one half of the infant mortality in the state. The second leading cause of infant mortality in Mississippi is SUID. Many of the risk factors associated with prematurity, low birth weight and SUID can be reduced or prevented by addressing gaps in knowledge and decreasing behavioral risks associated with these primary determinants of infant mortality.
The purpose of this project was to develop, pilot and evaluate an evidence-based curriculum that addressed knowledge gaps and behavioral risk factors related to determinants of infant mortality in low-income households in Mississippi.
Methods
The piloted curriculum, “Healthy Moms and Healthy Babies,” consisted of six topic areas including sessions that focused on increasing knowledge and awareness around prenatal and postnatal nutrition and physical activity, smoking, breastfeeding, safe infant sleep and maternal mental health and stress reduction. All sessions were taught by a certified health educator with a Masters of Public Health degree who was trained on the curriculum and informed consent procedures. Sessions were designed to increase participants’ knowledge of key messages in each of the six topic areas, to foster discussion about the participants’ behavioral intentions related to the topic area and provide a link to resources if the participant needed further information about a topic area.
Instruments were developed that included a comprehensive survey that collected demographic information; current access to prenatal care; behavioral information concerning intention to breastfeed, smoking habits, smoking cessation intention, fruit and vegetable consumption; and knowledge of key messages in each of the six areas of content. Participant satisfaction surveys were developed to capture feedback on the content and delivery method of all session materials. Each session had at least one knowledge, skill, behavioral and/or resource objective that was evaluated post intervention (Table 1). After the curriculum, session materials and assessment instruments were developed, a human subjects review application was presented to the Institutional Review Board of the University of Southern Mississippi and was approved prior to participant enrollment (Project Number: 16022504).
| Session Topic |
Evaluation Objectives |
| Pre- and Postnatal Nutrition |
K: Upon completion of the health education program, 90% of participants will know the recommended number of servings per day for fruits and vegetables.
S: Upon completion of the health education program, 75% of participants will be able to demonstrate that they can read and interpret a food label.
BI: Upon completion of the health education program, 80% of participants will report that they will be “likely” or “highly likely” to eat 5 or more fruits and vegetables daily. |
| Physical Activity |
K: Upon completion of the health education program, 90% of participants will be able to identify that women who are pregnant should exercise 30 min daily.
BI: Upon completion of the health education program, 75% of participants will report that they will be “likely” or “highly likely” to exercise 30 min daily. |
| Smoking |
K: Upon completion of the health education program, 80% of women will be able to identify smoking as the leading behavioral cause of low birth weight infants.
BI: Upon completion of the health education program, 70% of women who smoke will report that they will be “likely” or “highly likely” to quit smoking.
R: Upon completion of the health education program, 100% of women who smoke will receive resource information about smoking cessation groups and resources in the area. |
| Breastfeeding |
K: Upon completion of the health education program, 85% of women will be able to identify common barriers to breast feeding.
K: Upon completion of the health education program, 85% of women will be able to identify 5 healthy benefits of breast feeding.
BI: Upon completion of the health education program, 75% of women will report that they will be “likely” or “highly likely” to breastfeed.
R: Upon completion of the health education program, 100% of women will receive resource information about area lactation consultants. |
| Safe Infant Sleep |
K: Upon completion of the health education program, 80% of participants will be able to identify the correct infant sleep position.
BI: Upon completion of the health education program, 80% of participants will report that they will be “likely” or “highly likely” to place their infant on their back to sleep every night. |
| Maternal Mental Health |
K: Upon completion of the health education program, 85% of women will be able to list 3 warning signs of post-partum depression.
R: Upon completion of the health education program, 100% of women will develop a “stress reduction toolbox” whereby they take inventory of positive supporting people and resources that they can call in times of stress. |
| |
K=Knowledge Objective; S=Skill Objective, B= Behavioral Objective; R=Resource Objective; BI=Behavioral Intention Objective |
Table 1: Program Evaluation Objectives of Six Topic Areas.
Potential participants were recruited via informational flyers placed at the Health Department, Head Start and Early Head Start program offices, WIC Distribution Centers and large retail stores in and around the Jackson County Mississippi area. To be eligible for participation, individuals had to be 18 years of age or older, currently pregnant or planning to become pregnant or have a child at home less than one year of age. Classes were held at the local Head Start Centers in Vancleave, Moss Point and Gautier, Mississippi. Based on information obtained from focus groups conducted with childbearing aged women 18-44 at Jackson County Head Start Centers on preventative and reproductive health and to encourage attendance by mothers who were dropping off or picking up other children from the Head Start Centers, sessions either began in the morning directly after drop off or were scheduled so that they would conclude in the afternoon just prior to pick up. Additionally, the session duration was offered as either six-two hour sessions or four-three hour sessions. After informed consent was obtained from a participant, they were enrolled in the health education program and asked to complete the pre-intervention survey. Participants received a 50 dollar gift card to a local grocery store if they attended five of the six sessions and completed the preand post-intervention surveys. Depending on the time of day the class was offered (morning or afternoon), either a healthy breakfast or lunch was served.
Results
Participants
Twenty-nine women participated in the pilot health education program. Most women were African America (n=20, 69.0%), had completed high school (n=14, 48.3%) and earned between $0 and $15,000 annually (n=16, 66.7%). Women ranged in age from 19.8-38.1 years old (x ?=29.6 ± 4.8). Many of the women who participated were pregnant when the program began (n=11, 37.9%) and some had an infant less than one year of age (n=5, 17.3%). The women reported their number of previous pregnancies, along with the infants’ weight at birth and length of gestation. Altogether, data was available on 63 infants born to participants. Infant mortality risk factors were high in the participant group with 17.5% (n=11) of infants born with low birth weight and 38.1% (n=24) of infants being born premature. Additionally, 17.2% (n=5) of participants reported smoking up to two packs of cigarettes daily, every day.
Program evaluation
Although 29 women enrolled in the health education class, only 21 (72.4%) completed at least 5 sessions and both preand post-assessments. Women who discontinued the program reported that they either had pregnancy complications and had been instructed to go on bed rest by their physician (n=5), lacked child care (n=2) or lacked transportation to sessions (n=1).
Participants were asked to complete a session evaluation survey at the end of each session. The survey consisted of a question that asked participants to rate their overall session satisfaction and overall satisfaction with the health educator on a five point Lkert-type scale from ‘excellent’ to ‘poor’. The survey also contained space for the participant to provide comments about what they liked most and least about each session. Session feedback was consistently positive. The highest rated sessions were the Safe Infant Sleep session and the Maternal Mental Health session. Both of these sessions were rated ‘excellent’ by 100% (n=29) of participants. The sessions that addressed Smoking and Breastfeeding were rated as ‘excellent’ or ‘very good’ by 96.2% of participants. The Pre- and Postnatal Nutrition and Physical Activity educational sessions were rated as ‘excellent’ or ‘very good’ by 95.6% of participants.
There were several comments provided by participants that reflected what they liked most about the sessions. After compiling all the comments, themes became evident. One theme was that many participants stated that they did not know that infant mortality was such a prevalent health disparity in the community. Participants overwhelmingly felt supported by the group process. For example, comments from the Maternal Mental Health session were, “session made [them] feel like they weren’t alone,” or that they “weren’t the only one feeling stress from life events.” Several participants commented that they “liked the size of the class“ and “enjoyed getting to know the other women in the class”.
The health educator that delivered the content for all of the sessions was rated as ‘excellent’ or ‘very good’ for all sessions by 100% of participants. Comments received consisted of, “the health educator took her time explaining things that were difficult to do (interpret food label)” and “the health educator was very informative and really seemed to care about what she was teaching.”
The only comments received that suggested areas for improvement were to address ways to reduce financial stress during the Maternal Mental Health session and to allow more time for learning how to interpret the food label during the Preand Postnatal Nutrition session.
Results of participants’ progress toward meeting the programs’ objectives can be found (Tables 2). In all, 16 objectives were developed a priori. Participants’ post-intervention assessments indicated that 14 objectives were met and two objectives were not met. The first was a skill-based objective from the Pre- and Postnatal Nutrition session that required 75% of participants to demonstrate that they could read and interpret a food label. For the participant to be credited with learning the skill, they had to demonstrate that they could correctly identify the amount of food in one serving and they had to calculate the number of calories from fat in the serving of food (i.e., multiply the number of fat grams shown on the label by nine). This proved difficult for many participants. The second unmet objective was a knowledge-based objective from the Breastfeeding session that required 85% of participants to identify five healthy benefits of breastfeeding. A review of responses showed that 90.5% of participants (n=19) could successfully identify at least four healthy benefits of breastfeeding (Figure 1).
| Characteristics of Participants at Baseline |
n (%) |
| |
n (%) |
| Race |
n=29 |
| African American |
20 (69.0) |
| Caucasian |
2 (6.9) |
| Multi-racial |
(24.1) |
| |
|
| Educational Level |
n=29 |
| |
8 (27.6) |
| High School Graduate |
14 (48.3) |
| Some College |
4 (13.8) |
| Completed AS or BS degree |
3 (10.3) |
| |
|
| Income level |
n=24 |
| $0 - $15,000 |
16 (66.7) |
| $15,001-$25,000 |
4 (16.7) |
| $25,001-$35,000 |
4 (16.7) |
| Currently pregnant |
11 (37.9) |
| Have infant>1 year at home |
5 (17.2) |
| Plan to become pregnant in the next year |
14 (48.3) |
| Currently Smoke Cigarettes |
5 (17.2) |
| Self-reported Characteristics of Participants’ Previous Births |
n=63 |
| Percentage of infants born with low birth weight (<2500g) |
11 (17.5) |
| Percentage of infants born premature (<37 weeks gestation) |
24 (38.1) |
| |
|
| |
Median (Range) |
| Number of children at home |
2.0 (0-11) |
| |
Mean (Sd) |
| Age of Participants |
29.6 (4.8) |
Table 2: Characteristics of Participants (n=29).
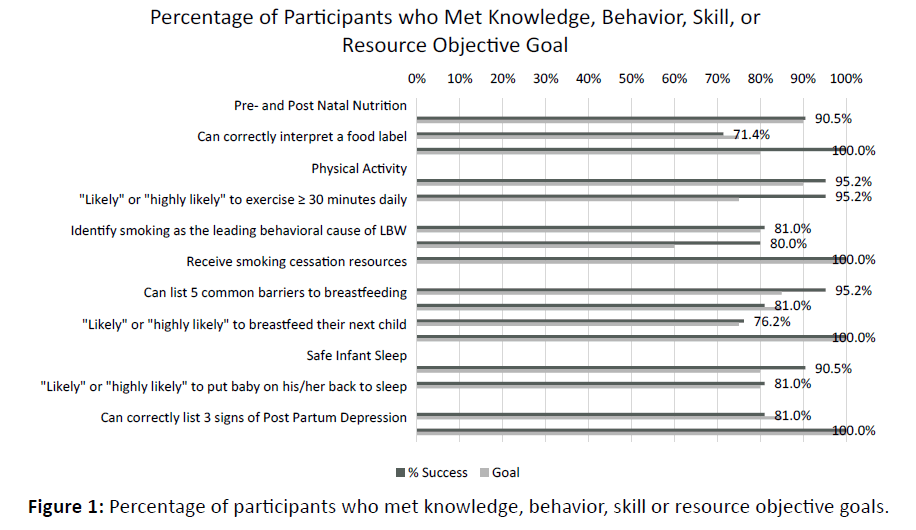
Figure 1: Percentage of participants who met knowledge, behavior, skill or resource objective goals.
Discussion
The racial health disparity in the incidence of infant mortality in Mississippi must be addressed through communitybased educational programming that prioritizes the needs of individuals in specific communities impacted by infant mortality. This pilot project evaluated one such intervention that provided education about ways in which to reduce the most common determinants of infant mortality in Mississippi. The intervention was successful in improving knowledge, skills and behavioral intentions surrounding common determinants of infant mortality. Though there were many successes throughout the program, but there were many barriers that were encountered.
First and foremost, infant mortality is not recognized in the community as a health priority. Many women reported that they were not aware that Mississippi had the highest infant mortality rate in the country or that African American families were disproportionately impacted. Women reported that they received information about being at risk for breast cancer and diabetes, but that they had never received information about infant mortality. Additionally, this type of loss is not often talked about in the community, which makes it difficult for infant
mortality to be seen as a community priority. In focus groups conducted with similar groups of Mississippi women, findings suggest that to talk about death or dying is to bring “bad luck” [6]. There were also findings that suggested that knowledge was not always a good predictor of behavior. For example, though 90.5% of participants knew that safe infant sleep practices require that a baby is put on his/her back to sleep, only 81.0% of participants stated that they would be ‘highly likely’ to actually put their baby to sleep on his/her back. This represents a dichotomy between ‘knowing’ and ‘doing’. Many women stated that their mother or grandmother had encouraged them to place their baby on their stomach to sleep and that they trusted that person to know what was best. With regard to placing an infant in a safe sleep environment, some mothers reported not having a dedicated safe sleeping space for their infant. Thus knowledge was not able to be aligned with behavior. One study conducted with parents of new-borns in Georgia found that Medicaid recipients who received bassinets from the hospital were 74% less likely to co-sleep [7].
The head start partnership offered a space to hold educational sessions, was convenient for mothers who already had an older child attending a Head Start program. For mothers who did not have a child enrolled in Head Start, the Head Start Center building was well-known and recognized as a regular meeting place in the community. Involving Head Start in the participant recruiting process was also helpful. Many studies describing health education interventions report successful partnerships with Head Start Centers. Some successful partnerships have been in the areas of nutritional interventions [8,9]. When offering the program again, participant feedback will be incorporated into the program. The areas of content surrounding unmet objectives should be considered in the context of the population being served [10-12]. With almost 67.7% of participants earning $15,000 or less annually, financial stress and ways to reduce that stress should be an integral part of the program content. These content components will be added to the Maternal Mental Health session. Further, in reviewing barriers to reading the food label, it is important to note that approximately one-third of participants did not have a high school diploma. Additional capacity-building exercise data 2007-2013es and skills development examples will be included in the Pre-and Postnatal Nutrition session to ensure both comprehension and application of content knowledge [13].
This project used a non-experimental post-test only study design and this first delivery served primarily as a way to evaluate the program’s materials and content with the priority population. In the future, the program will be delivered as a randomized control trial in which women who consent to participation are randomly assigned to a control (waiting group) or a treatment (educational group). At the conclusion of the treatment group’s intervention period, the control group would then be offered the educational program.
Reducing preterm birth is a national public health priority. Addressing knowledge gaps through risk-reduction education may reduce behaviors associated with determinants of infant mortality such as low birth weight and preterm birth. Partnering with Head Start Centers to provide participatory health education interventions is a strategy that has been largely ignored. Head Start Centers are convenient locations that can serve as hubs of education for the entire family.
Ethical approval
In order to ensure that the study maintained the highest ethical standards, a human subjects review application was presented to the Institutional Review Board of the University of Southern Mississippi and was approved prior to participant enrollment (Project Number: 16022504).
Acknowledgement
We would like to thank the Mississippi State Department of Health Office of Health Disparity Elimination for funding that made this pilot project possible.
Source of Funding
This project was funded by the Mississippi State Department of Health Office of Health Disparity Elimination grant, “Safeguarding Our Little Ones’ Lives”. Susan Mayfield- Johnson is partially supported by the National Institute of General Medical Sciences of the National Institutes of Health under Award Number 1U54GM115428. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Conflict of Interest
The authors state that there are no conflicts of interest; this includes ownership of shares, consultancy, speaker's honoraria or research grants from commercial companies or professional or governmental organizations with an interest in the topic of the paper.
References
- Office of Disease Prevention and Health Promotion (2017) Healthy People 2020.
- Mississippi State Department of Health (2016) Mississippi State Department of Health Infant Mortality Report.
- Lu MC, Johnson KA (2014) Toward a national strategy on infant mortality. Am. J. Public Health. United States. 104:S1- S15.
- Richardson SD, Josberger RE (2017) Maternal medicaid recipient status and congenital malformations among New York state live births in 2010. Birth Defects Res. 109:1460-1470.
- Hakeem GF, Oddy L, Holcroft CA, Abenhaim HA (2015) Incidence and determinants of sudden infant death syndrome: A population-based study on 37 million births. World J Pediatr.11:41-47.
- Northington L, Graham J, Winters K, Fletcher A (2011) Assessing knowledge of sudden infant death syndrome among african american women in two mississippi communities. J Cult Divers.18:95-100.
- Walcott R L, Salm Ward TC, Ingels JB, Llewellyn NA, Miller TJ, et al. (2017) A Statewide Hospital-Based Safe Infant Sleep Initiative: Measurement of Parental Knowledge and Behavior. J Community Health. 42:1-9.
- Song WO, Song S, Nieves V, Gonzalez A, Crockett ET, et al. (2016) Nutritional health attitudes and behaviors and their associations with the risk of overweight/obesity among child care providers in Michigan Migrant and Seasonal Head Start Centers. BMC Public Health. 16:1-11.
- Morshed AB, Davis SM, Keane PC, Myers OB, Mishra SI (2016) The Impact of the CHILE Intervention on the Food Served in Head Start Centers in Rural New Mexico. J Sch Health. 86:414-423.
- Cruz TH, Davis SM, Myers OB, Oâ€Âââ€Å¾Â¢Donald ER, Sanders SG, et al. (2016) Effects of an obesity prevention intervention on physical activity among preschool children. Health Promot Pract.17:693-701.
- Wallace ME, Green C, Richardson L, Theall K, Crear-Perry J (2017) “Look at the Whole Meâ€ÂÂÂÂ: A mixed-methods examination of black infant mortality in the US through womenâ€Âââ€Å¾Â¢s lived experiences and community context. Int. J. Environ. Res. Publ. Health.14:727.
- Harper-Hanigan K, Ross G, Sims T, Trotter K, Turman J, et al. (2017) Womenâ€Âââ€Å¾Â¢s perspectives of needs surrounding adverse birth outcomes: A qualitative assessment of the neighbourhood impact of adverse birth outcomes. Matern Child Health J. 21:2219-2228.
- US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics, Division of Vital Statistics. Natality public use data 2007-2013. CDC WONDER Online Database; November 2013.

