Keywords
cetuximab; Drug Therapy; Epidermal Growth Factor; erlotinib; Pancreatic Neoplasms; panitumumab; Protein Kinase Inhibitors; Receptor, Epidermal Growth Factor
Abbreviations
ADL: activities of daily life; BSA: body surface area; CTC: common toxicity criteria; CTCAE: common terminology criteria for adverse events; CTG: Clinical Trials Group; HR: hazard ratio; NCI: National Cancer Institute, U.S. National Institute of Health; NCIC: National Cancer Institute of Canada; SPF: sunburn protection factor
Conflict of interest
The authors have no potential conflicts of interest
INTRODUCTION
With approximately 37,680 new cases and 34,290 deaths estimated in 2008, pancreatic adenocarcinoma represents the fourth leading cause of cancer-related deaths in the United States [1]. At the time of diagnosis, 80% of the patients present with locally advanced, unresectable or metastatic disease, representing a significant therapeutic dilemma [2]. Surgery is the only curative treatment for pancreatic cancer, but even then long-term survival is less than 20%, suggesting the need of adjuvant treatment (chemotherapy or/and radiotherapy). Gemcitabine, a nucleoside analogue, has demonstrated modest benefit in overall survival and symptoms control [3], while the addition of a second cytotoxic agent (5-FU, cisplatin, oxaliplatin) demonstrated a significant advantage in terms of response rates and progression free survival, but did not yield a significant overall survival advantage [2].
Recently, the phase III National Cancer Institute of Canada Clinical Trials Group (NCIC-CTG) study has shown a statistically significant survival benefit of the combination of gemcitabine plus the epidermal growth factor receptor (EGFR) inhibitor erlotinib compared with gemcitabine alone [4]. The combined treatment arm demonstrated an 18% reduction in the risk of death or an overall 22% improvement in survival than the gemcitabine alone arm, and it was statistically superior in 1-year survival (23.8% vs. 19.4%; P=0.028) and in median survival (6.4 vs. 6.0 months) [4]. Based on these data, the US Food and Drug Administration (FDA) has granted approval for erlotinib to be administered in combination with gemcitabine for the treatment of advanced pancreatic cancer.
Erlotinib is a highly specific epidermal growth factor receptor (HER1/EGFR) tyrosine kinase inhibitor [5]. It inhibits ATP binding to HER1/EGFR tyrosine kinase in normal and tumour cells. Several human malignancies are associated with aberrant expression of epidermal growth factor receptor. The latter has been related to chemoresistance and poor prognosis [5]. Tyrosine kinase HER1/EGFR is a potential target for therapeutic intervention in ovarian, head, neck, lung, breast, bladder and other squamous cell cancers [5, 6, 7].
The most common side effect in patients receiving erlotinib is skin rash, as discussed below, and diarrhea. Other reported sideeffects included interstitial lung disease [8, 9] especially following therapy with gemcitabine and erlotinib, possibly due to drug interaction [10].
Skin rash is the commonest side effect of erlotinib administration in metastatic pancreatic cancer patients, sometimes leading to the discontinuation of this, potentially beneficial treatment. Furthermore, treatment of this particular group of patients is mainly palliative and preservation of the quality of life should be the main priority of the treating physician. Skin rash often hampers significantly the quality of life and therefore needs insistent management. In this manuscript we review the existing data regarding the pathogenesis of the erlotinib induced skin rash and we provide guidelines for its management
ERLOTINIB INDUCED SKIN RASH
Incidence
Skin rash has been documented as one of the commonest adverse reactions in patients receiving erlotinib and other EGFR inhibitors [4, 8, 9, 11] occurring in at least 79% patients treated with erlotinib [2]. In fact there is high incidence of rash in patients treated with EGFR inhibitors, ranging from 50 to 100% [9]. Grade 3-4 rash (the authors used the Common Terminology Criteria v2.0 (CTC) classification of the National Cancer Institute (NCI), U.S. National Institute of Health: https://ctep.cancer.gov/forms/CTCv20_4-30-992.pdf) [12] was documented in 9% of erlotinib treated patients requiring dose reduction in 6% and discontinuation in 1% of patients [11]. Similar results (5%) occurred in the pancreatic cancer trial, with dose reduction in 2% patients and discontinuation in 1% [4].
Pathogenesis of Erlotinib-Induced Skin Rash
Pathogenesis underlying erlotinib-associated rash remain incompletely understood but interference with the follicular and interfollicular epidermal-growth signaling pathway is considered to play a major role. The rash develops as early as three days after commencement of erlotinib therapy, with median onset the eight days [10]. It resembles acne and has macroscopically been described as well demarcated erythematous papulopustular with lesions ranging from pin-head to lentil size. Crusting and pruritus has also been noted [11], sometimes similar to seborrheic dermatitis or Pityrosporum folliculitis. Although rash is commonly referred to as “acneiform”, it is not acne and should not be treated as acne. Commonly affected areas include the face, neck and upper thorax [10]. On a microscopic level, lymphocytic perifolliculitis or suppurative superficial folliculitis secondary to follicular rupture has been visualized by Busam et al. [13].
interference with the follicular and interfollicular epidermal-growth signaling pathway is considered to play a major role. The rash develops as early as three days after commencement of erlotinib therapy, with median onset the eight days [10]. It resembles acne and has macroscopically been described as well demarcated erythematous papulopustular with lesions ranging from pin-head to lentil size. Crusting and pruritus has also been noted [11], sometimes similar to seborrheic dermatitis or Pityrosporum folliculitis. Although rash is commonly referred to as “acneiform”, it is not acne and should not be treated as acne. Commonly affected areas include the face, neck and upper thorax [10]. On a microscopic level, lymphocytic perifolliculitis or suppurative superficial folliculitis secondary to follicular rupture has been visualized by Busam et al. [13].
In addition to stimulating epidermal growth, inhibiting differentiation, EGFR also plays a critical role in protecting against UV-induced damage, inhibiting inflammation, and accelerating wound healing. EGFR is known to be expressed in epidermal keratinocytes, sebaceous and eccrine glands, and hair follicle epithelium, and the greatest expression occurs in proliferating and undifferentiated keratinocytes, which are located in the basal and suprabasal layers of the epidermis and outer root sheath of the hair follicle. Druginduced inhibition of EGFR is thought to alter keratinocyte proliferation, differentiation, migration, and attachment, and this may help to explain the papulopustular reaction and xerosis.
Erlotinib inhibits epidermal growth factordependent cell proliferation at nanomolar concentration and also blocks cell-cycle proliferation [15]. These changes are accompanied in vitro by release of inflammatory cell chemoattractants that recruit leukocytes that lead to keratinocyte apoptosis and subsequently tenderness, papulopustules, and periungual inflammation. These changes may also favor bacterial overgrowth, thus exacerbating inflammation. Mouse models suggest that the rash is transient and disappears with prolonged treatment, perhaps as a result of EGFR receptor blockade. Mitra and Simcock [16] have demonstrated that erlotinib induced skin rash spared skin in previous radiated field. In fact Lacouture et al. [17] have explained that radiation therapy leads to destruction of healthy hair follicles and sebaceous glands. Hence EGFR inhibitors do not affect previously irradiated areas. In contrast, acute radiation may lead to inflammation of the target area due to proliferating stem-cell derived skin cells being radiosensitive. Finally, Harari et al. [18] have suggested that erlotinib may act as a radiosensitizer: papulopustular eruption occurred at a recently irradiated site after commencing erlotinib treatment. The amount of radiation necessary to induce rash is not clear. In conclusion it seems that the time frame between irradiation and administration of erlotinib is crucial in the development of rash in irradiated areas.
Manifestation of Rash
In pivotal studies, the severity of rash was graded according to the NCI-CTC version 2.0 criteria (https://ctep.cancer.gov/forms/CTCv20_4- 30-992.pdf) [12] prior to 2006, and then according to the NCI Common Terminology Criteria for Adverse Events (CTCAE) version 3.0 criteria (https://ctep.cancer.gov/forms/ CTCAEv3.pdf) [19] (Figure 1, Table 1). However, this criterion is designed primarily as a surveillance tool, and its use to select interventions and predicting their effectiveness is not clear. In addition, EGFR inhibitor-associated rashes are generally
Figure 1. Erlotinib induced grade 2 skin rash in a
pancreatic cancer patient. The skin rash was graded
according to the National Cancer Institute: Common
Terminology Criteria for Adverse Events (NCICTCAE)
version 3.0 [19].
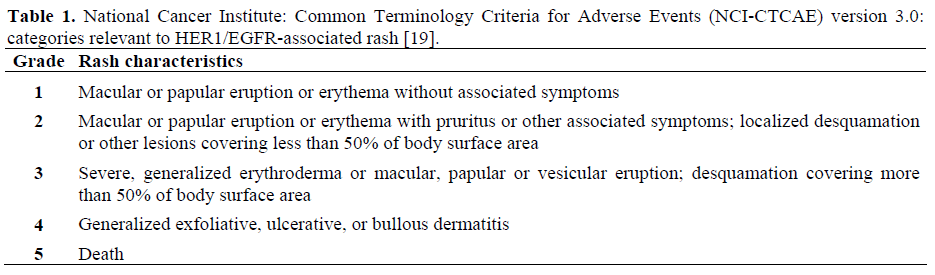
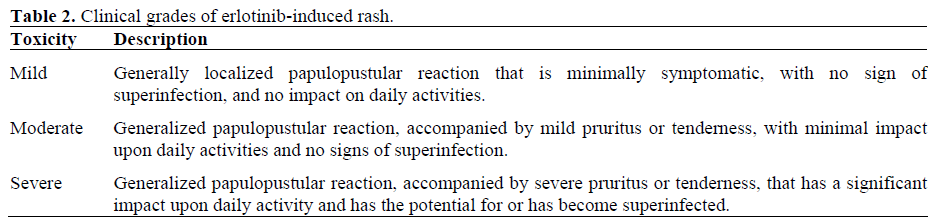
confined to the face and upper trunk, and can be of high severity at such anatomic sites. Moreover, discoloration, pitting, and ridging associated with grade 1 nail changes do not occur in response to EGFR inhibitor treatment. To overcome these limitations, a simpler, more EGFR inhibitor-focused grading system has been proposed (Table 2).
Clinical Significance
It has been suggested that rash could be used as an objective response to therapy and possibly be associated with prolonged survival. Studies with several different EGFR agents show correlation between rash and clinical efficiency. Cutaneous rash seems to be a surrogate marker of clinical benefit [20].
In the NCIC-CTG study, the majority of patients (81%) developed grade 2 rash. Patients receiving erlotinib and developing a rash showed median survival 7.1 months (grade 1) or 11.1 months (grade 2) in contrast to 3.3 months in patients who did not develop rash while taking erlotinib. Rash development was linked to overall and progression free survival and these correlations increased with grade (grade 1 vs. no rash: hazard ratio (HR) 0.47, P<0.001; grade 2 or more vs. no rash: HR 0.29; P<0.001) [4]. However, rash was also present in 18% of placebo taking patients with median survival 8.2 months. Placebotaking patients who did not develop rash had median survival 4.7 months. In the combined treatment arm (gemcitabine plus erlotinib) 81% of the patients developed a rash, compared with 30% of patients in the control group.
The results are difficult to analyze, since gemcitabine itself is known to induce skin rash. The rash seemed to correlate with complete response, partial response and stable disease (grade 2 or more rash vs. no rash HR 0.47, P<0.001) [21]. Patients on erlotinib and gemcitabine showed an escalating medial survival of 10.8 months (grade 2 skin rash), 5.7 months (grade 1) and 5.4 months (no rash). Perez-Soler et al. have reported that rash was experienced by all patients with an objective response to erlotinib as well as in 95% of 22 patients with stable disease in contrast to 54% of 28 patients with progressive disease [4]. Finally, skin rashes have also been described during treatment with other EGFR inhibitors such as cetuximab [22] and panitumumab [23] and have been linked to better survival.
It has been suggested that the rash clinically improves with continuation of treatment. Nevertheless, severe rash development may be a determining cause of treatment discontinuation by patients on erlotinib outside clinical trials. If rash development is in fact a surrogate marker for treatment success, then patients discontinuing treatment are potentially stopping a life prolonging treatment. This is why it is crucial to exploit all means available in the treatment of the erlotinib-induced skin rash, in order to discourage patients from stopping it.
Dose Escalation
One important question is whether increasing the dose of erlotinib can induce rash or increase the severity of rash in those patients who do not develop rash at the initial prescribed dose. The dose of erlotinib as a single agent and in combination studies in non-small-cell lung cancer is 150 mg per day. In the pivotal NCIC study, there were 23 patients treated at a starting dose of 150 mg of erlotinib of whom 11 required protocolprescribed dose reductions for toxicity, suggesting that this may be too high a starting dose [4]. The pharmacokinetics of erlotinib has shown significant variability in previous studies with clearance rates and area under the curve varying up to seven-fold. It is possible that escalation of the dose of erlotinib beyond 100 mg in patients not experiencing toxicity may be useful.
EGFR Polymorphism
One question arises that why some patients develop rash and others do not following erlotinib. The possible explanations may include, but not limited to individual differences in drug exposure, the integrity of the immune system or EGFR polymorphisms. As described earlier that the rash usually develops within 2 weeks of start of therapy [24], rash may be used a biomarker in future studies as after the lead-in period, patients could be stratified by whether rash occurred and randomized to different therapies or doses of erlotinib.
Management
Since data suggest that development of rash in patients who develop rash following erlotinib is suggestive of efficacy, developing effective strategies to manage rash while continuing erlotinib therapy is important. Optimal management of rash in patients on erlotinib remains somewhat controversial, but a proactive approach should be undertaken to allow patients to continue receiving therapy without dose interruption or drug discontinuation. It is also important to counsel patients about the positive aspects of developing rash on erlotinib as part of clinical management of this side effect.
General Guidelines
Skin care. All patients should be strongly encouraged to use a thick alcohol-free emollient to prevent and alleviate the skin dryness [22, 23].
Protection from sunlight. Patients can minimize the extent or intensity of the eruption by avoiding sunbathing or direct, strong sunlight, high-heat or humidity during treatment [22, 23]. Use sunscreen of sunburn protection factor (SPF) 15 or higher.
Make-up related issues. The rash can be covered with makeup. A dermatologistapproved cover-up can be used although any type of foundation may be useful. The makeup should be removed with a hypoallergenic (skin-friendly) liquid cleanser [22, 23].
Local therapy. Most of local therapy involved usage of topical antibiotics (clindamycin gel or lotion) and topical steroids. Anecdotal reports of benefit from topical antiinflammatory (acne) preparations have been reposted. Topical antibiotics are usually used when pustules are present or about to develop. Usage or benefits of topical steroids is controversial. The manufacturers of cetuximab (Bristol-Myers Squibb, Co., New York, NY, USA; Imclone Systems, Inc., New York, NY, USA) advise against the use of topical steroids because of the potential to cause infectious complications. But other institutions have used high potency agents like clobetasol propionate in grade 1 or 2 rash in order to combat inflammation and prevent infection [22, 23]. Also hydrocortisone valerate topical steroid cream or ointment has been used in early rash with good result. Pathology of rash caused by EGFR inhibitors differ from the acne vulgaris therefore medications for acne vulgaris such as benzoyl peroxide should not used. In one institution, acne wash, such as benzoyl peroxide at bedtime was used and helped control cetuximab-related rash, but led to dry skin and a burning sensation and was not as effective as steroid creams and topical antibiotics [22, 23]. No such data exists for erlotinib.
Systemic therapy. Systemic therapy such steroids (to decrease discomfort) and oral antibiotics has been used in grade 3 or 4 rash in order to relive the symptoms or treat the complication of rash. If infection is suspected from the rash is suspected oral antibiotics such as tetracyclines (minocycline) can be used to treat the infection. Tetracycline has weak anti-inflammatory effects and reasonably good activity against Staphylococcus aureus.
Treatment of Rash with Respect to Stage
If patients develop rash related to erlotinib, the following interventions are suggested, based on severity of the reaction (Table 3, Figure 2) [22, 23, 24, 25, 26, 27, 28].
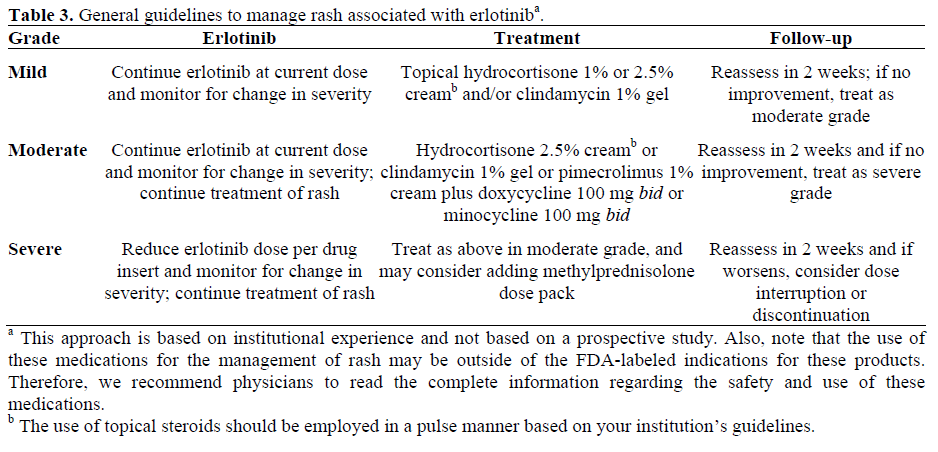
Figure 2. Management algorithm for erlotinibassociated
rash (adapted from [28]).
Mild Toxicities
The erlotinib dosage should not be altered for mild toxicities. Use of topical hydrocortisone (1% or 2.5% cream) or clindamycin (1% gel) can be considered.
Moderate Toxicities
The erlotinib dosage should be altered based on clinical judgment. Treatment options may include:
• hydrocortisone (2.5% cream);
• clindamycin (1% gel);
• pimecrolimus (1% cream);
• doxycycline (100 mg, po twice a day);
• minocycline (100 mg, po twice a day).
Severe Toxicities
The erlotinib dose should be reduced. Concomitant intervention is the same as for moderate toxicities, however, addition of methylprednisolone dose pack may be considered. If rash does not resolve within 2-4 weeks, despite treatment, then interruption of erlotinib therapy is recommended.
Future Perspectives
Current data suggest that at least a grade 2 rash is needed for survival benefit to pancreatic cancer patients. Still many issues remain unsolved, such as the effect of gemcitabine on rash development, the correlation of EGFR status or the presence of EGFR mutations with the presence of the rash. It is of particular interest to investigate whether, increasing the erlotinib dose until rash development would result to increased clinical benefit. Specificity of inhibition with regards to other tyrosine kinase receptors has not been fully characterized yet. It has not been fully understood yet why patients receiving placebo developed rash and showed prolonged survival. Further studies should assess the type of patients likely to develop rash. The genotype of patients developing rash and responding to treatment might play a significant role in treatment progress.
CONCLUSION
In conclusion, erlotinib-induced cutaneous rash, should be managed as intensively as possible, in order to continue a potentially beneficial treatment. Further studies are needed in order to identify which patients have an increased likelihood to develop rash and whether increasing the erlotinib dose and therefore the potential of rash development would offer a clinical benefit.
References
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, Thun MJ. Cancer statistics, 2008. CA Cancer J Clin 2008; 58:71-96. [PMID: 18287387]
- Saif MW. Pancreatic cancer: highlights from the 42nd annual meeting of the American Society of Clinical Oncology, 2006. JOP. J Pancreas (Online) 2006; 7:337-48. [PMID: 16832131]
- Burris HA 3rd, Moore MJ, Andersen J, Green MR, Rothenberg ML, Modiano MR, et al. Improvements in survival and clinical benefit with gemcitabine as firstline therapy for patients with advanced pancreas cancer: a randomized trial. J Clin Oncol 1997; 15:2403-13. [PMID: 9196156]
- Moore MJ, Goldstein D, Hamm J, Figer A, Hecht JR, Gallinger S, et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: a phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J Clin Oncol 2007; 25:1960-6. [PMID: 17452677]
- Rusch V, Mendelsohn J, Dmitrovsky E. The epidermal growth factor receptor and its ligands as therapeutic targets in human tumors. Cytokine Growth Factor Rev 1996; 7:133-41. [PMID: 8899291]
- Davies DE, Chamberlin SG. Targeting the epidermal growth factor receptor for therapy of carcinomas. Biochem Pharmacol 1996; 51:1101-10. [PMID: 8645330]
- Baselga J, Mendelsohn J. The epidermal growth factor receptor as a target for therapy in breast carcinoma. Breast Cancer Res Treat 1994; 29:127-38. [PMID: 8018961]
- Mitchell EP, Perez-Soler R, Van Cutsem E, Lacouture ME. Clinical presentation and pathophysiology of EGFRI dermatologic toxicities. Oncology (Williston Park) 2007; 21(11 Suppl 5):4-9. [PMID: 18154212]
- Gerdes S, Mrowietz U. Follicular rash during therapy with erlotinib (Tarceva). J Dtsch Dermatol Ges 2006; 4:855-7. [PMID: 17010175]
- Boeck S, Hausmann A, Reibke R, Schulz C, Heinemann V. Severe lung and skin toxicity during treatment with gemcitabine and erlotinib for metastatic pancreatic cancer. Anticancer Drugs 2007; 18:1109-11. [PMID: 17704662]
- Gutzmer R, Werfel T, Kapp A, Elsner J. Cutaneous side effects of EGF-receptor inhibition and their management. Hautarzt 2006; 57:509-13. [PMID: 16205868]
- National Cancer Institute, U.S. National Institute of Health. Common Toxicity Criteria v2.0 (CTC). https://ctep.cancer.gov/reporting/ctc_archive.html (Publish date April 30,1999. Accessed January 14, 2008).
- Busam KJ, Capodieci P, Motzer R, Kiehn T, Phelan D, Halpern AC. Cutaneous side-effects in cancer patients treated with the antiepidermal growth factor receptor antibody C225. Br J Dermatol 2001; 144; 1169-76. [PMID: 11422037]
- Tan AR, Steinberg SM, Parr AL, Nguyen D, Yang SX. Markers in the epidermal growth factor receptor pathway and skin toxicity during erlotinib treatment. Ann Oncol 2008; 19:185-90. [PMID: 17878175]
- Pollack VA, Savage DM, Baker DA, Tsaparikos KE, Sloan DE, Moyer JD, et al. Inhibition of epidermal growth factor receptor-associated tyrosine phosphorylation in human carcinomas with CP- 358,774: dynamics of receptor inhibition in situ and antitumor effects in athymic mice. J Pharmacol Exp Ther 1999; 291:739-48. [PMID: 10525095]
- Mitra SS, Simcock R. Erlotinib induced skin rash spares skin in previous radiotherapy field. J Clin Oncol 2006; 24:e28-9. [PMID: 16735697]
- Lacouture ME, Hwang C, Marymont MH, Patel J. Temporal dependence of the effect of radiation on erlotinib-induced skin rash. J Clin Oncol 2007; 25:2140. [PMID: 17513824]
- Harari PM, Huang S. Radiation combined with EGFR signal inhibitors: head and neck cancer focus. Semin Radiat Oncol 2006; 13:38-44. [PMID: 16378905]
- National Cancer Institute, U.S. National Institute of Health. Common Terminology Criteria for Adverse Events v3.0 (CTCAE). https://ctep.cancer.gov/reporting/ ctc_v30.html (Publish date August 9, 2006; Accessed January 14, 2008)
- Perez-Soler R. Rash as a surrogate marker for efficacy of epidermal growth factor receptor inhibitors in lung cancer. Clin Lung Cancer 2006; 8 Suppl 1:S7- 14. [PMID: 17239291]
- Tang PA, Tsao MS, Moore MJ. A review of erlotinib and its clinical use. Expert Opin Pharmacother 2006; 7:177-93. [PMID: 16433583]
- Saif MW, Kim R. Incidence and management of cutaneous toxicities associated with cetuximab. Expert Opin Drug Saf 2007; 6:175-82. [PMID: 17367263]
- Saif MW, Cohenuram M. Role of panitumumab in the management of metastatic colorectal cancer. Clin Colorectal Cancer 2006; 6:118-24. [PMID: 16945167]
- Wacker B, Nagrani T, Weinberg J, Witt K, Clark G, Cagnoni PJ. Correlation between development of rash and efficacy in patients treated with the epidermal growth factor receptor tyrosine kinase inhibitor erlotinib in two large phase III studies. Clin Cancer Res 2007; 13:3913-21. [PMID: 17606725]
- Lacouture ME, Melosky BL. Cutaneous reactions to anticancer agents targeting the epidermal growth factor receptor: a dermatology-oncology perspective. Skin Therapy Lett 2007; 12:1-5. [PMID: 17762902]
- Gridelli C, Maione P, Amoroso D, Baldari M, Bearz A, Bettoli V, et al. Clinical significance and treatment of skin rash from erlotinib in non-small cell lung cancer patients: Results of an Experts Panel Meeting. Crit Rev Oncol Hematol 2007; 66:155-62. [PMID: 18083041]
- Peréz-Soler R, Saltz L. Cutaneous adverse effects with HER1/EGFR-targeted agents: is there a silver lining? J Clin Oncol 2005; 23:5235-46. [PMID: 16051966]
- Lynch TJ Jr, Kim ES, Eaby B, Garey J, West DP, Lacouture ME. Epidermal growth factor receptor inhibitor-associated cutaneous toxicities: an evolving paradigm in clinical management. Oncologist 2007; 12:610-21. [PMID: 17522250]



