Keywords
Antibodies, Monoclonal; cetuximab; erlotinib; Pancreatic Neoplasms; Protein Kinase Inhibitors; Protein-Tyrosine Kinase; Receptor, Epidermal Growth Factor
Abbreviations
ATP: adenosine triphosphate; ASCO: American Society of Clinical Oncology; EGF: epidermal growth factor; EGFR (alias: ErbB, ErbB1): epidermal growth factor receptor (erythroblastic leukemia viral (v-erb-b) oncogene homolog, avian) [Homo sapiens]; ErbB2 (alias: HER-2, HER-2/neu): v-erb-b2 erythroblastic leukemia viral oncogene homolog 2, neuro/glioblastoma derived oncogene homolog (avian) [Homo sapiens]; ErbB3: verb- b2 erythroblastic leukemia viral oncogene homolog 3 (avian) [Homo sapiens]; FDA: Food and Drug Administration; PI3K: phosphatidylinositol 3-kinase; TGF-alpha: transforming growth factor alpha; TKI: tyrosine kinase inhibitor
INTRODUCTION
Cancer of the exocrine pancreas is the fourth most common malignancy in the United States. The annual incidence rate is almost identical to the mortality rate with approximately 25,000 new cases diagnosed each year in the United States and 24,800 deaths. A minority of patients (15-20%) present with resectable disease as pancreatic cancer tends to metastasize to regional lymph nodes early in the course of the disease and many patients have subclinical liver metastases at the time of diagnosis [1]. Of patients with locally advanced or metastatic disease, the median survival is 9 and 4 months respectively and a mere 1-4% will be alive at 5 years [2]. Even among those who are able to undergo resection with curative intent, a majority (70-75%) will relapse and succumb to their disease within 5 years.
Consequently, a sizeable number of patients will receive systemic therapy during the course of their disease, either as first line therapy, as part of adjuvant treatment, upon relapse or as first line therapy. 5-fluorouracil was the first agent to be widely used in the treatment of advanced pancreatic cancer but response rates were less than 20% and it was not known to provide significant palliative benefits. Gemcitabine, the current standard of care in first line treatment, was approved based on a relatively dramatic improvement in clinical benefit response (24% versus 5%) but median survival was only modestly improved from 4.4 months to 5.6 months [3]. Unfortunately, combination therapy with other cytotoxic agents has either failed to provide significant benefit or has done so at the expense of intolerable toxicities. As such, there is an obvious need for agents which will not only improve upon currently available treatment regimens but which will do so with acceptable toxicities as palliation and quality of life are paramount in a disease with such poor outcomes.
The Epidermal Growth Factor Receptor (EGFR) and Its Role in Pancreatic Cancer
EGFR (also known as HER-1 or ErbB1) is a 170 kDa membrane spanning glycoprotein composed of an amino terminal extracellular ligand binding domain, a hydrophobic transmembrane region and a cytoplasmic domain that contains both the tyrosine kinase domain as well as receptor regulatory motifs. Upon binding to one of its natural ligands, the EGFR homodimerizes or heterodimerizes with another member of the ErbB receptor family, which in turn activates protein tyrosine kinase activity and leads to tyrosine autophosphorylation. These phosphorylated tyrosines serve as binding and activating sites for a number of signal transducers and adaptor molecules that, in turn, are responsible for a wide array of downstream signaling pathways. The two main signaling routes are the ras-raf-mitogen activated protein kinase pathway and the phosphatidylinositol 3-kinase (PI3K)/Akt pathway [4]. EGFR has a number of natural ligands including: epidermal growth factor (EGF), transforming growth factor-alpha (TGF-alpha), heparin binding growth factor, amphiregulin, betacellulin and epiregulin [5]. Within normal cells, the EGFR is tightly regulated but inappropriate or constitutive activation can occur as a result of EGFR mutation, over-expression, structural rearrangements and/or relief of its normal auto-inhibitory and regulatory constraints [4]. In the transformed cell, unregulated EGFR activation can promote a range of oncogenic activities such as proliferation, migration, stromal invasion, tumor neo-vascularization and resistance to pro-apoptotic signals [6]. Over-expression or inappropriate activation is now known to be manifest in a number of human malignancies including upper aerodigestive tract, breast, ovary, bladder, kidney, and gliomas [4]. Human pancreatic cancer is also known to over-express EGFR [7]. More importantly, there is data that has demonstrated a statistically significant decrease in survival in pancreatic cancer patients over-expressing the EGFR and at least one of its ligands [8] and thus may be a poor prognostic factor and a molecular signature of a more malignant phenotype [9].
Two distinct therapeutic approaches, monoclonal antibodies and small-molecule tyrosine kinase inhibitors (TKIs) are currently employed in the treatment of pancreatic cancer. Most are in various stages of clinical study as monotherapy, in conjunction with other cytotoxic agents and in conjunction with radiotherapy. One TKI, erlotinib or Tarceva®, has already received Food and Drug Administration (FDA) approval as treatment for metastatic pancreatic cancer based on a phase III study which will be discussed later. In addition to their activity as monotherapy, both classes of drugs are thought to sensitize cancer cells to nonspecific cytotoxic drugs, presumably by interruption of EGFRmediated survival signals that then make the tumor more vulnerable to these drugs and other cellular stresses [4]. See Table 1 for list of EGFR targeted agents currently in clinical development.

The Monoclonal Antibodies
The monoclonal antibodies specifically bind to the extracellular ligand-binding domain of EGFR and thereby competitively inhibit ligand binding as well as preventing receptor dimerization, autophosphorylation and downstream signal transduction. Additionally it is thought that there are two other unique mechanisms: monoclonal antibodies may also recruit Fc receptor expressing immune effector cells leading to antibody dependent cell mediated cytotoxicity and binding of the monoclonal antibodies may lead to downregulation from the cell surface (endocytosis) thereby promoting cell cycle arrest and death [4].
Most available monoclonal antibodies are murine, chimeric or humanized, and thus have the potential to elicit an immune response that infrequently, but not insignificantly, results in infusion reactions and can interfere with drug clearance. In addition to cetuximab (Erbitux®), which is now in broad use in colorectal cancer and increasingly so in head and neck cancer, other agents in this class include matuzumab and hR3 (TheraCIM). Additionally, a new fully human monoclonal antibody, panitumumab, has demonstrated significant clinical benefit in a large phase III trial for patients with metastatic colorectal cancer. The advantages of the monoclonal antibodies are that they are highly specific with predictable pharmacokinetics that result in long serum half lives and are thus amenable to less frequent administration.
In vitro and in vivo studies done using a human pancreatic cancer cell line implanted within an orthotopic nude mouse model demonstrated significant activity of Erbitux®, both as monotherapy and in combination with gemcitabine, compared with mice treated with gemcitabine alone [10]. These effects were evidenced by assays demonstrating marked synergy for the combination therapy in terms of decreased EGFR phosphorylation, decreased proliferation, decreased angiogenesis and increased apoptosis. Macroscopically visible tumors were only seen in 5/10 mice treated with Erbitux® alone, 0/9 in mice treated with combination therapy versus 10/10 in the gemcitabine group. Additionally, there was noted to be marked reduction in the number of lymph node and liver metastases [10]. The combination of cetuximab and gemcitabine has also been studied in vivo in combination with radiation and also demonstrated synergistic activity in two different cell lines, one of which resulted in 100% complete response for more than 250 days [11].
Several phase I studies have demonstrated cetuximab to be well tolerated, both alone and in combination with other cytotoxic therapy as well as with radiotherapy [12, 13, 14, 15]. The maximum tolerated dose has not been reached and toxicities have been mild with a high prevalence of skin toxicities. Studies have included co-administration with 5- fluorouracil, gemcitabine, carboplatin and cisplatin, none of which impacted on the pharmacokinetics of cetuximab [12, 13, 14, 16]. Based on these results, the standard loading dose of 400 mg/m2 followed by weekly 250 mg/m2 was chosen for a multicenter phase II trial of cetuximab in combination with gemcitabine 1,000 mg/m2 for treatment naïve patients with locally advanced or metastatic pancreatic cancer [17]. Sixty-one patients were initially screened and 41 patients were enrolled in the study based on EGFR status as determined by immunohistochemistry; 4 patients were 1+ (faint or barely perceptible membrane staining), 20 patients were 2+ (weakmoderate staining of complete cell membrane) and 17 patients were 3+ (strong staining of complete cell membrane). The primary endpoints of this study were overall response and time to progression. A 12% partial response was seen after 2 cycles and an additional 63% had stable disease. Median survival was 7.1 months and 31.7 % were alive at one year. In keeping with previous observations of the correlation between rash and efficacy of EGFR targeted agents, all five of the patients achieving partial response had a rash and skin toxicity was associated with longer survival. Similar to what was seen in the phase I studies, cetuximab was well tolerated with rash and asthenia observed in a significant number of the patients (88% and 85%, respectively). Other significant toxicities, such as nausea, weight loss and abdominal pain, were ascribed more to the primary disease itself. Only five patients experienced a grade 3 rash and there were no treatment discontinuations as a result. Three patients had allergic reactions, all of which were grade 2.
Currently, the Southwestern Oncology Group is conducting a large phase III trial that randomizes patients with locally advanced or metastatic pancreatic cancer to first-line treatment with either gemcitabine alone or in combination with cetuximab [18]. There also several other phase II trials looking at cetuximab in combination with a number of other agents including concomitant administration with other targeted agents including erlotinib and bevacizumab. Presently, there is no published data, but these are ongoing trials which are listed on the National Cancer Institute (NCI) website (https://www.cancer.gov).
A recent phase I trial of another humanized monoclonal antibody, matuzumab or EMD- 72000, given concurrently with gemcitabine to patients with advanced pancreatic cancer demonstrated it to be well tolerated and with reliable pharmacokinetics. Thirteen of the 17 patients experienced skin toxicity although these were all grade 1 and 2. Eight of the 12 patients evaluated for response demonstrated either partial response or stable disease while three of six in the cohort treated at the highest dose achieved partial response [19]. A second humanized monoclonal antibody, nimotuzumab, has also gone through phase I testing in patients with pancreatic cancer with a reasonable toxicity profile. As monotherapy, results were very modest and phase II testing will be done in combination with gemcitabine [20].
The Tyrosine Kinase Inhibitors (TKIs)
The TKIs are a novel class of drugs that were developed based on findings that mutations in the adenosine triphosphate (ATP) binding pocket affected tyrosine kinase activity and were therefore thought to be critical to EGFR mediated cell cycle progression [4]. The TKIs are low molecular weight agents that target the intracellular domain of EGFR and compete with ATP for binding to the kinase domain, thereby impeding downstream signaling. Unlike the aforementioned monoclonal antibodies which are fairly specific to EGFR, the TKIs demonstrate some cross reactivity with the ATP binding domains of other members of the ErbB family [21]. The two main drugs in this class, erlotinib and gefitinib, initially came in to widespread use in the treatment of non small cell lung cancer but are now increasingly being applied to a wider range of malignancies including head and neck, colorectal, ovarian and gliomas and as mentioned earlier, erlotinib has been FDA approved for the treatment of metastatic pancreatic cancer as well.
Both drugs have undergone extensive preclinical study and have demonstrated significant efficacy. Erlotinib was found to have marked effects on downstream signaling and increased apoptosis in xenografts of two pancreatic cancer cell lines with differential expression of EGFR. Similar to cetuximab, erlotinib was synergistic with gemcitabine, almost doubling the response rate [22]. Li et al. demonstrated that gefitinib not only decreased cellular proliferation and signal transduction but also may affect the metastatic potential of pancreatic cancer by inhibiting anchorage-independent growth and invasiveness [23].
This section will exclusively focus on erlotinib as it is the only TKI that is currently FDA approved for treatment of patients with pancreatic cancer.
Phase I studies have demonstrated 150 mg to be the maximally tolerated dose for continuous administration. In a group of 40 patients with advanced solid malignancies, the main dose limiting toxicities were severe diarrhea and skin toxicity [24]. Fifty-nine percent of all patients had a cutaneous reaction which generally occurred between days 8-10 and tended to resolve despite continued treatment, in some cases completely resolving. Three patients actually discontinued treatment due to the rash which they deemed intolerable despite the fact that the investigators evaluated it as grade 2. Other common toxicities included mucositis, hyperbilirubinemia, and headache which were only mild to moderate in severity. Two patients achieved partial response and another six had stable disease for at least 5-month duration. There was a correlation seen between the area under the curve (AUC) and the maximum concentration (Cmax) and cutaneous toxicity but not with other toxicities or with response. Moreover, no direct association was observed between EGFR status and clinical outcome.
There is also phase I data on erlotinib given concurrently with gemcitabine in patients with pancreatic cancer. Safety data was presented at the 2003 meeting of the American Society of Clinical Oncology (ASCO) with clinical outcomes presented the following year [25, 26]. Toxicities were similar to the aforementioned study with the exception of some hematological toxicities which were more likely attributable to the gemcitabine. Pharmacokinetics analysis did not demonstrate any significant interactions and no dose limiting toxicities were observed on this trial. Of the 12 patients with pancreatic cancer treated on this study, there was one partial response, 3 minor responses and 6 patients with stable disease for an overall disease control rate of 70% and a median duration of treatment of 4 months.
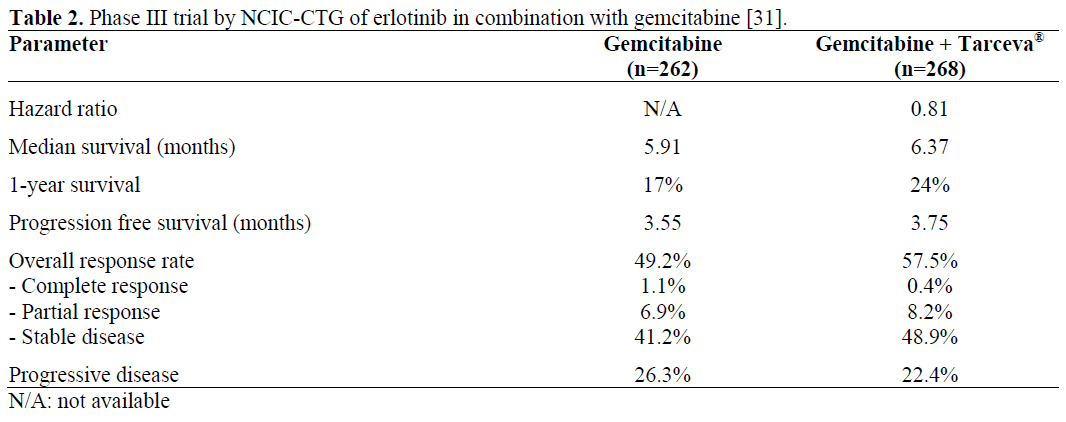
As opposed to results in non small cell lung cancer where multiple trials including Intact I and II, TALENT and TRIBUTE [27, 28, 29, 30] all failed to demonstrate added efficacy of TKIs when given in combination with cytotoxic therapy, the results of a recent phase III trial of erlotinib in combination with gemcitabine led to its approval by the FDA as first line treatment for unresectable pancreatic cancer. Reported at the 2005 ASCO GI meeting, this was the first phase III trial to ever demonstrate an overall survival benefit from combination therapy for pancreatic cancer (see Table 2) [31]. Five hundred sixty nine chemotherapy naïve patients were randomized to receive gemcitabine 1,000 mg/m2 weekly for seven weeks with one week off followed by three out of four weeks with erlotinib at 100 mg/day (a small cohort of 48 patients was treated with 150 mg/day) or placebo. Eligibility was not dependent on EGFR status. The study was a double blind placebo controlled study adequately powered for overall survival to be the primary endpoint. Secondary endpoints included progression free survival, quality of life, response rate and toxicity. Overall survival was 6.4 months for the combination arm versus 5.9 for the control arm with a P value equal to 0.025. Twenty-four percent of those on the combination arm were alive at one year versus 17% for the control arm. Interestingly, while the overall response rate was significantly higher in the arm receiving erlotinib (58 versus 49%), this was primarily due to an increase in stable disease with no significant difference in partial response.
The combination regimen was relatively well tolerated with the primary toxicities being rash (72%; with 6% were grade 3 or 4) and diarrhea (51%; with 6% being grade 3 or 4). Other toxicities that were significantly more common the combination arm were infection and stomatitis. Additionally, 2.1% of patients on the control arm developed interstitial lung disease versus 0.4% on the control arm. Other than diarrhea, which favored the placebo arm, there were no other significant differences in quality of life parameters between the two arms.
Erlotinib is also being evaluated in combination with capecitabine for patients with metastatic pancreatic cancer who have already failed first line therapy with gemcitabine [32]. Preliminary results of 28 patients accrued to a phase II trial were presented at the 2005 ASCO meeting. Capecitabine was given at 1,000 mg/m2 twice a day for 14 out of 21 days and the dose of erlotinib was 150 mg. Median number of cycles received was almost 4. The regimen was generally well tolerated with 14% of patients experiencing grade 3 and 4 rash and diarrhea. Eleven percent have achieved partial response and 57% have achieved stable disease with median survival of 6.7 months, all of which are fairly encouraging for pancreatic cancer salvage therapy.
Gefitinib has also been studied as part of a salvage regimen for pancreatic cancer based on preclinical data that demonstrated increased efficacy in combination with docetaxel as compared to docetaxel alone. Preliminary results of a phase II study were presented at the most recent ASCO [33]. Results have not been quite as impressive as those discussed previously although this may be due to the fact that docetaxel is possibly less active than either capecitabine or gemcitabine in pancreatic cancer. In this study with 31 patients enrolled thus far, the best response has been stable disease seen in 5 patients and median survival is 4.4 months. Given a significant incidence of neutropenic fever, the dose of docetaxel has been reduced from 75 mg/m2 to 60 mg/m2 with enrollment ongoing at this time.
As mentioned in the monoclonal antibody section, there are ongoing trials looking at both erlotinib and cetuximab in combination with other targeted agents including with each other. A preliminary analysis of one phase II study randomizing patients to gemcitabine and bevacizumab with either cetuximab (GBC) or erlotinib (GBE) was presented at the most recent ASCO [34]. Both arms have demonstrated significant activity with response rates of 19% and 21% respectively and stable disease rate of 59% and 67% respectively. Both regimens have been fairly well tolerated thus far with the bulk of the toxicities ascribed to bevacizumab.
EGFR Targeted Agents in Combination with Radiotherapy
Several key lessons from both preclinical and clinical studies underlie the examination of EGFR inhibitors as radiotherapy sensitizers in cancer therapy: 1) positive correlation between EGFR expression and cellular resistance to radiation in many cell types [35]; 2) the degree of radioresistance correlates with the level of EGFR over-expression [7]; 3) cell survival and recovery during a course of radiotherapy are influenced by activation of EGFR/TGF-alpha that is induced after exposure to radiation [36]; and 4) inhibition of EGFR signaling augmented radiation sensitivity [37, 38]. Moreover, there is specific preclinical data supporting the additive benefits of cetuximab in combination therapy with radiotherapy [11].
The recent landmark study by Bonner et al., comparing radiotherapy and cetuximab versus radiotherapy alone for patients with locally advanced head and neck cancer, demonstrated marked improvement in efficacy with little in the way of additional toxicity [39]. Spurred by the above observations, as well as the encouraging results from the Bonner study [39], a multicenter phase II study is currently underway in Germany employing “trimodal therapy” with radiotherapy, gemcitabine and cetuximab as first line therapy for patients with locally advanced pancreatic cancer. Preliminary results on the first 20 patients were presented at the 2006 ASCO meeting [40]. At a median follow up of six months, median survival has not been reached and there were 8/20 partial responses and 9/20 stable diseases. Early toxicity assessment shows the regimen to be fairly well tolerated and while 18 patients developed some type of acneiform rash, no doses of cetuximab have had to be omitted. Several phase I studies have also been performed to assess the feasibility and efficacy of TKIs in combination with radiotherapy. One of the trials used a novel regimen of concomitant gemcitabine, paclitaxel and erlotinib concurrent with radiotherapy followed by maintenance erlotinib until disease progression [41]. The maximally tolerated dose of erlotinib during the radiotherapy phase was 50 mg. There were multiple dose limiting toxicities described including diarrhea, rash, myelosuppression and small bowel stricture but results were encouraging with a reported 46% rate of partial response. At this time, investigation of so-called “trimodality therapy” for pancreatic cancer has not progressed to phase III study.
Modes of Resistance to EGFR Therapy: The Future for Improved Targeting and Alternative Anti-EGFR Strategies
It is becoming increasingly apparent that the complexity of the EGFR signaling cascade provides a wealth of mechanisms for resistance to EGFR targeted agents in patients with pancreatic cancer. Conversely, as development proceeds with additional targeted agents for moieties located downstream of EGFR or in pathways which “crosstalk” with EGFR, the opportunities arise for combination targeted therapies which may overcome resistance or provide synergy with those agents which are currently available. A number of studies have already been done based on prior observations of different pancreatic cancer cell lines manifesting markedly disparate sensitivities to EGFR antagonism.
Both over-expression of other members of the ErbB receptor family (ErbB2 (also know as HER-2 or HER-2/neu) and ErbB3) as well as constitutive activation of molecules downstream of EGFR (mitogen activated protein kinase, Akt or STAT3) via alternative mechanisms (e.g., BAX, FGF and GRB2) have been identified [42, 43]. In turn, these molecules provide additional rational targets to either augment the effects of EGFR targeted agents in patients whose tumors are predisposed to be responsive or conversely sensitize those which are de novo resistant or have become resistant to this class of drugs. Preclinical studies have already demonstrated synergistic anti-tumor effects of erlotinib when used in combination with the PI3K inhibitor wortmannin [21]. Additionally, lapatinib, a dual inhibitor of EGFR and HER- 2/neu that is newly approved for the treatment of metastatic breast cancer, demonstrated superior efficacy when compared to erlotinib in pancreatic cancer cell lines with disparate levels of EGFR expression [44].
HER-2/neu and Its Role in Pancreatic Cancer
HER-2 or ErbB2, another member of the EGFR family of receptors, deserves special discussion based on the aforementioned results with lapatinib as well as the widespread use and profound benefits of trastuzumab (Herceptin®) already seen in breast cancer. In cells that co-express HER-2, ligand activated EGFR preferentially recruits HER-2 into a heterodimer with increased potency and duration of PI3K activation as this can couple with PI3K directly whereas other ErbB homo- and hetero-dimers cannot [4]. This unique quality may in some part underlie the observation that breast cancers over-expressing HER-2/neu have a particularly aggressive phenotype with increased invasiveness and greater proclivity for relapse [44].
It is unknown if this may bestow similar characteristics in pancreatic cancer although preclinical data has demonstrated constitutive activation of molecules downstream of EGFR such as STAT3 that has been observed to lead to a growth factor independent phenotype in pancreatic cancer cell lines and which was blocked by antagonism of ErbB2 kinase activity but was only slightly reduced with blockade of EGFR [45]. Over-expression of HER-2 in pancreatic cancer as compared to normal pancreatic tissues has been demonstrated by immunohistochemistry and immunoreactivity [46] and was found to be amplified in 21% of specimens from a pancreatic cancer tissue archive [47]. While trastuzumab was found to have marked in vitro activity in cell lines expressing high levels of HER-2/neu [48], concurrent treatment with gemcitabine in patients with metastatic pancreatic cancer did not result in superior response rates than what has been seen with gemcitabine monotherapy [49]. These results may in part be explained by the fact that 88% of those in the study were only 2+ by immunohistochemistry and may have in fact been fluorescent in situ hybridization negative, but it raises the question of the need for concomitant EGFR blockade and this may very well be an important field of study in the future.
Novel EGFR-Based Approaches
In addition to the aforementioned studies of novel combinations of monoclonal antibodies and TKIs with and without anti-VEGF therapy, there are several ongoing preclinical studies employing unique approaches to the targeting of the EGFR in pancreatic cancer. One approach is based on the fusion of an exotoxin to a monoclonal antibody directed against an epitope preferentially expressed on the tumor. In vitro study of a fusion product of EGFR with Pseudomonas exotoxin A demonstrated marked binding activity and specificity against a pancreatic cancer cell line and achieved a 50% inhibition of cell proliferation [50]. While there are theoretical concerns regarding potential systemic effects of the toxin, this is likely to be an ongoing field of study given the previous success and increasing use of Ontak® or denileukin diftitox (monoclonal antibody against IL2 conjugated to diphtheria toxin) which is now FDA approved for T cell lymphomas. Another novel approach which has been tested both in vitro and in animal models developed a population of activated T cells which had been specifically “armed” by fusion with a bispecific antibody formed by cross-linking of anti-EGFR and anti-CD3. Studies in nude mice demonstrated equivalent efficacy to cetuximab in achieving retardation of growth of established pancreatic tumor xenografts although was not similarly effective in a colorectal tumor cell line [51]. Given the fact that its mechanism of action is independent of the signaling pathway, this may be an interesting therapeutic option and warrants further clinical investigation.
Discussion
Pancreatic cancer persists as a major therapeutic challenge largely characterized by chemotherapy-refractory disease and poor responses to currently available treatments. Thus far EGFR targeted therapies have demonstrated promising results with favorable toxicity profiles and studies of currently available agents proceed in later phase trials as well as in combination with other agents both in the first and second lines. Nonetheless, even dual therapy with gemcitabine and erlotinib, which was the first combination therapy in pancreatic cancer to ever demonstrate statistically significant benefits in overall survival, did so with modest results. Concomitant administration of the monoclonal antibodies and TKIs together and with other targeted agents may both augment their therapeutic activity as well as offset mechanisms of resistance.
Perhaps more importantly will be to truly target our therapy with the EGFR agents as well as other biologic agents by identifying those patients who are most likely to derive benefit and achieve meaningful responses. This is particularly crucial in a disease such as pancreatic cancer that has such a short life expectancy that the “window” for any given treatment may be quite small. Already we have seen changes in treatment paradigms for EGFR therapy with increasing evidence that EGFR over-expression in colorectal cancer is not essential for response and there is conflicting data in lung cancer with regard to the significance of tyrosine kinase mutations. Consequently, further study should include the development of more predictive assays and improved exploitation of surrogate biomarkers of response such as the development of skin rash or re-analysis of downstream markers of EGFR inhibition early in the course of treatment.
References
- Brand RE, Tempero MA. Pancreatic cancer. CurrOpinOncol 1998; 10:362-66. [PMID 9702405]
- Wanebo HJ, Vezeridis MP. Pancreatic carcinoma in perspective. A continuing challenge. Cancer 1996; 78:580-91. [PMID 8681296]
- Burris HA 3rd, Moore MJ, Andersen J, Green MR, Rothenberg ML, Modiano MR, et al. Improvements in survival and clinical benefits with gemcitabine as firstline therapy for pts with advanced pancreatic cancer: a randomized trial. J ClinOncol 1997; 15:2403-13. [PMID 9196156]
- Arteaga CL. The epidermal growth factor receptor: from mutant oncogene in nonhuman cancers to therapeutic target in human neoplasia. J ClinOncol 2001; 19:32s-40s. [PMID 11560969]
- Yarden Y, Sliwkowski MX. Untangling the ErbBsignalling network. Nat Rev Mol Cell Biol 2001; 2:127-37. [PMID 11252954]
- Baselga J. Why the epidermal growth factor receptor? The rationale for cancer therapy. Oncologist 2002; 7 Supp 4:2-8. [PMID 12202782]
- Xiong HQ, Abbruzzese JL. Epidermal growth factor receptor-targeted therapy for pancreatic cancer. SeminOncol 2002; 29(5 Suppl 14):31-7. [PMID 12422311]
- Yamanaka Y, Friess H, Kobrin MS, Buchler M, Beger HG, Korc M. Coexpression of epidermal growth factor receptor and ligands in human pancreatic cancer is associated with enhanced tumor aggressiveness. Anticancer Res 1993; 13:565-9. [PMID 8317885]
- Ueda S, Ogata S, Tsuda H, Kawarabayashi N, Kimura M, Sugiura Y, et al. The correlation between cytoplasmic overexpression of epidermal growth factor receptor and tumor aggressiveness: poor prognosis in patients with pancreatic ductal adenocarcinoma. Pancreas 2004; 29:e1-8. [PMID 15211117]
- Bruns CJ, Harbison MT, Davis DW, Portera CA, Tsan R, McConkey DJ, et al. Epidermal growth factor receptor blockade with C225 plus gemcitabine results in regression of human pancreatic carcinoma growing orthotopically in nude mice by antiangiogenic mechanisms. Clin Cancer Res 2000; 6:1936-48. [PMID 10815919]
- Buchsbaum DJ, Bonner JA, Grizzle WE, Stackhouse MA, Carpenter M, Hicklin DJ, et al. Treatment of pancreatic cancer xenografts with Erbitux (IMC-C225) anti-EGFR antibody, gemcitabine, and radiation. Int J RadiatOncolBiolPhys 2002; 54:1180- 93. [PMID 12419447]
- Baselga J, Pfister D, Cooper MR, Cohen R, Burtness B, Bos M, et al. Phase I studies of antiepidermal growth factor receptor chimeric antibody C225 alone and in combination with cisplatin. J ClinOncol 2000; 18:904-14. [PMID 10673534]
- Robert F, Blumenschein G, Herbst RS, Fossella FV, Tseng J, Saleh MN, Needle M. Phase I/IIa study of cetuximab with gemcitabine plus carboplatin in patients with chemotherapy-naive advanced non-smallcell lung cancer. J ClinOncol 2005; 23:9089-96. [PMID 16301597]
- Bourhis J, Rivera F, Mesia R, Awada A, Geoffrois L, Borel C, et al. Phase I/II study of cetuximab in combination with cisplatin or carboplatin and fluorouracil in patients with recurrent or metastatic squamous cell carcinoma of the head and neck. J ClinOncol 2006; 24:2866-72. [PMID 16717293]
- Robert F, Ezekiel MP, Spencer SA, Meredith RF, Bonner JA, Khazaeli MB, et al. Phase I study of antiepidermal growth factor receptor antibody cetuximab in combination with radiation therapy in patients with advanced head and neck cancer. J ClinOncol 2001; 19:3234-43. [PMID 11432891]
- Shin DM, Donato NJ, Perez-Soler R, Shin HJ, Wu JY, Zhang P, et al. Epidermal growth factor receptortargeted therapy with C225 and cisplatin in patients with head and neck cancer. Clin Cancer Res 2001; 7:1204-13. [PMID 11350885]
- Xiong HQ, Rosenberg A, LoBuglio A, Schmidt W, Wolff RA, Deutsch J, et al. Cetuximab, a monoclonal antibody targeting the epidermal growth factor receptor, in combination with gemcitabine for advanced pancreatic cancer: a multicenter phase II Trial. J ClinOncol 2004; 22:2610-16. [PMID 15226328]
- Southwest Oncology Group, National Cancer Institute (NCI), Cancer and Leukemia Group B, National Cancer Institute of Canada. Gemcitabine with or without Cetuximab as first-line therapy in treating patients with locally advanced unresectable or metastatic adenocarcinoma of the pancreas. National Cancer Institute, ID=NCT00075686.
- Graeven U, Kremer B, Sudhoff T, Killing B, Rojo F, Weber D, et al. Phase I study of the humanised anti- EGFR monoclonal antibody matuzumab (EMD 72000) combined with gemcitabine in advanced pancreatic cancer. Br J Cancer 2006; 94:1293-9. [PMID 16622465]
- Strumberg D, Scheulen ME, Hilger RA, Krauss J, Marschner N, Lordick F, Bach F, Reuter D, Edler L, Mross K. Safety, efficacy and pharmacokinetics of nimotuzumab, a humanized monoclonal anti-epidermal growth factor receptor (EGFR) antibody, as monotherapy in patients with locally advanced or metastatic pancreatic cancer (PC). ASCO Annual Meeting 2006; Abs 12504.
- Herbst R. ZD1839: targeting the epidermal growth factor receptor in cancer therapy. Expert OpinInvestig Drugs 2002; 11(6):837-49. [PMID 12036427]
- Ng SS, Tsao MS, Nicklee T, Hedley DW. Effects of the epidermal growth factor receptor inhibitor OSI- 774, Tarceva, on downstream signaling pathways and apoptosis in human pancreatic adenocarcinoma. Mol Cancer Ther 2002; 1:777-83. [PMID 12492110]
- Li J, Kleeff J, Giese N, Buchler MW, Korc M, Friess H. Gefitinib ('Iressa', ZD1839), a selective epidermal growth factor receptor tyrosine kinase inhibitor, inhibits pancreatic cancer cell growth, invasion, and colony formation. Int J Oncol 2004; 25:203-10. [PMID 15202007]
- Hidalgo M, Siu LL, Nemunaitis J, Rizzo J, Hammond LA, Takimoto C, et al. Phase I and pharmacologic study of OSI-774, an epidermal growth factor receptor tyrosine kinase inhibitor, in patients with advanced solid malignancies. J ClinOncol 2001; 19:3267-79. [PMID 11432895]
- Dragovich T, Patnaik A, Rowinsky E, Karp D, Huberman M, Clinebell T, et al. A phase I B trial of gemcitabine and erlotinib HCL in patients with advanced pancreatic adenocarcinoma and other potentially responsive malignancies. ASCO Annual Meeting 2003; Abs 895.
- Porterfield BW, Dragovich T, Patnaik A, Rowinsky E, Huberman M, Clinebell T, et al. Erlotinib + gemcitabine in patients with unresectable pancreatic carcinoma: Results from a phase IB trial. ASCO Annual Meeting 2004; Abs 4110.
- Giaccone G, Herbst RS, Manegold C, Scagliotti G, Rosell R, Miller V, et al. Gefitinib in combination with gemcitabine and cisplatin in advanced non-small-cell lung cancer: a phase III trial. INTACT 1. J ClinOncol 2004; 22:777-84. [PMID 14990632]
- Herbst RS, Giaccone G, Schiller JH, Natale RB, Miller V, Manegold C, et al. Gefitinib in combination with paclitaxel and carboplatin in advanced non-smallcell lung cancer: a phase III trial. INTACT 2. J ClinOncol 2004; 22:785-94. [PMID 14990633]
- Gatzemeier U, Pluzanska A, Szczesna A, Kaukel E, Roubec J, Brennscheidt U, et al. Results of a phase III trial of erlotinib (OSI-774) combined with cisplatin and gemcitabine (GC) chemotherapy in advanced nonsmall cell lung cancer (NSCLC). J ClinOncol 2004; 22(14S):7010.
- Herbst RS, Prager D, Hermann R, Miller V, Fehrenbacher L, Hoffman P, et al. TRIBUTE - A phase III trial of erlotinibHCl (OSI-774) combined with carboplatin and paclitaxel (CP) chemotherapy in advanced non-small cell lung cancer (NSCLC). J ClinOncol 2004; 22(14S):7011.
- Moore MJ, Goldstein D, Hamm J, Kotecha J, Gallinger S, Au HJ, et al. Erlotinib improves survival when added to gemcitabine in patients with advanced pancreatic cancer. A phase III trial of the National Cancer Institute of Canada Clinical Trials Group [NCIC-CTG]. ASCO Gastrointestinal Cancers Symposium 2005; Abstract 77.
- Blaszkowsky LS, Kulke KH, Ryan DP, Clark JW, Meyerhardt J, Zhu AX, et al. A phase II study of erlotinib in combination with capecitabine in previously treated patients with metastatic pancreatic cancer. ASCO Annual Meeting 2005; Abs 4099.
- Shadad F, Matin K, Evans T, Volkin R, Kiefer G, Schlesselman J, et al. Phase II study of gefitinib and docetaxel as salvage therapy in patients (pts) with advanced pancreatic adenocarcinoma (APC). ASCO Annual Meeting 2006; Abs 4120.
- Kindler H, Bylow K, Hochster H, Friberg G, Micetich K, Locker G, et al. A randomized phase II study of bevacizumab and gemcitabine plus cetuximab or erlotinib in patients with advanced pancreatic cancer: A preliminary analysis. ASCO Annual Meeting 2006; Abs 4040.
- Baumann M, Krause M. Targeting the epidermal growth factor receptor in radiotherapy: radiobiological mechanisms, preclinical and clinical results. RadiotherOncol 2004; 72:257-66. [PMID 15450723]
- Bowers G, Reardon D, Hewitt T, Dent P, Mikkelsen RB, Valerie K, et al. The relative role of ErbB1-4 receptor tyrosine kinases in radiation signal transduction responses of human carcinoma cells. Oncogene 2001; 20:1388-97. [PMID 11313882]
- Schmidt-Ullrich RK, Mikkelsen RB, Dent P, Todd DG, Valerie K, Kavanagh BD, et al. Radiation-induced proliferation of the human A431 squamous carcinoma cells is dependent on EGFR tyrosine phosphorylation. Oncogene 1997; 15:1191-7. [PMID 9294612]
- Huang SM, Harari PM. Modulation of radiation response after epidermal growth factor receptor blockade in squamous cell carcinomas: inhibition of damage repair, cell cycle kinetics, and tumor angiogenesis. Clin Cancer Res 2000; 6:2166-74. [PMID 10873065]
- Bonner JA, Harari PM, Giralt J, Azarnia N, Shin DM, Cohen RB, et al. Radiotherapy plus cetuximab for squamous-cell carcinoma of the head and neck. N Engl J Med 2006; 354:567-78. [PMID 16467544]
- Iannitti D, Dipetrillo T, Akerman P, Barnett JM, Maia-Acuna C, Cruff D, et al. Erlotinibandchemoradiation followed by maintenance erlotinib for locally advanced pancreatic cancer: a phase I study. Am J ClinOncol 2005; 28:570-5. [PMID 16317266]
- Arnoletti JP, Buchsbaum DJ, Huang ZQ, Hawkins AE, Khazaeli MB, Kraus MH, Vickers SM. Mechanisms of resistance to Erbitux (anti-epidermal growth factor receptor) combination therapy in pancreatic adenocarcinoma cells. J GastrointestSurg 2004; 8 960-9. [PMID 15585383]
- Huang ZQ, Buchsbaum DJ, Raisch KP, Bonner JA, Bland KI, Vickers SM. Differential responses by pancreatic carcinoma cell lines to prolonged exposure to Erbitux (IMC-C225) anti-EGFR antibody. J Surg Res 2003; 111:274-83. [PMID 12850474]
- Baerman KM, Caskey LS, Dasi F, Earp HS, Calvo BF. EGFR/HER2 targeted therapy inhibits growth of pancreatic cancer cells. ASCO Annual Meeting 2005; Abs 84.
- Slamon DJ, Clark GM, Wong SG, Levin WJ, Ullrich A, McGuire WL. Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science 1987; 235:177- 182. [PMID 3798106]
- DeArmond D, Brattain MG, Jessup JM, Kreisberg J, Malik S, Zhao S, Freeman JW. Autocrine-mediated ErbB-2 kinase activation of STAT3 is required for growth factor independence of pancreatic cancer cell lines. Oncogene 2003; 22:7781-95. [PMID 14586404]
- Yamanaka Y, Friess H, Kobrin MS, Buchler M, Kunz J, Beger HG, Korc M. Overexpression of HER2/neu oncogene in human pancreatic carcinoma. Hum Pathol 1993; 24:1127-34. [PMID 8104858]
- Safran H, Steinhoff M, Mangray S, Rathore R, King TC, Chai L, et al. Overexpression of the HER- 2/neu oncogene in pancreatic adenocarcinoma. Am J ClinOncol 2001; 24: 496-9. [PMID 11586103]
- Buchler P, Reber HA, Buchler MC, Roth MA, Buchler MW, et al. Therapy for pancreatic cancer with a recombinant humanized anti-HER2 antibody (herceptin). J GastrointestSurg 2001; 5:139-46. [PMID 11331475]
- Safran H, Iannitti D, Ramanathan R, Schwartz JD, Steinhoff M, Nauman C, et al. Herceptin and gemcitabine for metastatic pancreatic cancers that overexpress HER-2/neu. Cancer Invest 2004; 22:706- 12. [PMID 15581051]
- Bruell D, Stocker M, Huhn M, Redding N, Kupper M, Schumacher P, et al. The recombinant anti-EGF receptor immunotoxin 425(scFv)-ETA' suppresses growth of a highly metastatic pancreatic carcinoma cell line. Int J Oncol 2003; 23:1179-86. [PMID 12964002]
- Reusch U, Sundaram M, Davol PA, Olson SD, Davis JB, Demel K, et al. Anti-CD3 x anti-epidermal growth factor receptor (EGFR) bispecific antibody redirects T-cell cytolytic activity to EGFR-positive cancers in vitro and in an animal model. Clin Cancer Res 2006; 12:183-90. [PMID 16397041]

