Keywords
C-Reactive Protein; Debridement; Enteral Nutrition; Pancreatitis, Acute Necrotizing; Parenteral Nutrition
Abbreviations
CTSI: computed tomography severity index; EN: enteral nutrition; TPN: total parenteral nutrition
INTRODUCTION
Patients with severe acute pancreatitis suffer from nutritional impairment during the course of the disease and nutritional support is mandatory [1, 2, 3, 4]. Total parenteral nutrition (TPN) and enteral nutrition (EN), generally delivered beyond the duodenum are the two options available. While a meta-analysis demonstrated decreased pancreatic infection rates, need for surgical intervention, hospital stay and costs in EN patients [5] and a prospective randomized control study showed a significantly decreased mortality rate in EN patients [6], another randomized study showed that total TPN was more effective in providing increased calories and proteins in comparison to EN [7]. Yet another recent meta-analysis of high quality studies has demonstrated that EN results in clinically relevant and statistically significant risk reduction of infectious complications, pancreatic infections and mortality in patients with predicted severe acute pancreatitis [8]. EN has also been shown to be beneficial as an adjunct to the management of severe acute pancreatitis by obviating the systemic inflammatory response syndrome and in modifying the course of the disease [9].
Various approaches adopted for nutritional support in recent clinical trials include TPN, nasojejunal feeding, nasogastic feeding, and dual enteral and parenteral nutritional support [1, 10, 11, 12]. Spanier et al. [13] evaluated nutritional management in a Dutch cohort (EARL study) and concluded that nutritional interventions were rapidly undertaken with enteral feeding via the jejunum as the preferred route. A critical analysis of trials comparing EN with TPN has concluded that, although there is evidence to support EN as the preferred option, both EN and TPN have a role [10]. Nutritional supplementation with the addition of specific agents - immunomodulation and probiotics is still an unresolved issue [13, 14, 15, 16, 17, 18, 19]. The present study was undertaken to compare the two forms of nutrition in severe acute pancreatitis as regards inflammatory markers, serum albumin and outcome.
METHODS
All patients with severe acute pancreatitis admitted to Nehru Hospital affiliated with the Postgraduate Institute of Medical Education and Research, Chandigarh, India between July 2006 and December 2007 were included in the study. Severe acute pancreatitis was defined using the Atlanta criteria [20]: clinical features, hyperamylasemia (three times the normal upper limit), and radiological evidence of severe acute pancreatitis (contrast enhanced CT (CECT) scan evidence of pancreatic necrosis and a computed tomography severity index (CTSI) equal to, or greater than, 7). The exclusion criteria were acute or chronic pancreatitis, patients who had undergone intervention prior to admission, patients requiring inotropic support at inclusion, or complications requiring surgical intervention at the time of inclusion.
Fifty consecutive patients with severe acute pancreatitis with a CTSI equal to or greater than 7 were randomized to receive either EN (n=25) or TPN (n=25). All patients were managed routinely by gastrointestinal decompression, prophylactic antibiotics (ciprofloxacin/metronidazole or imipenem/cilastatin), intravenous fluids and organ system support. Nutritional support was initiated within 72 hours of admission and was continued for a minimum of 14 days. The need for further continuation of nutritional support was decided on the basis of the patients’ clinical status. Image-guided fine needle aspiration or percutaneous drainage of pancreatic or peripancreatic collection as a temporizing measure was resorted to in patients who continued to be toxic.
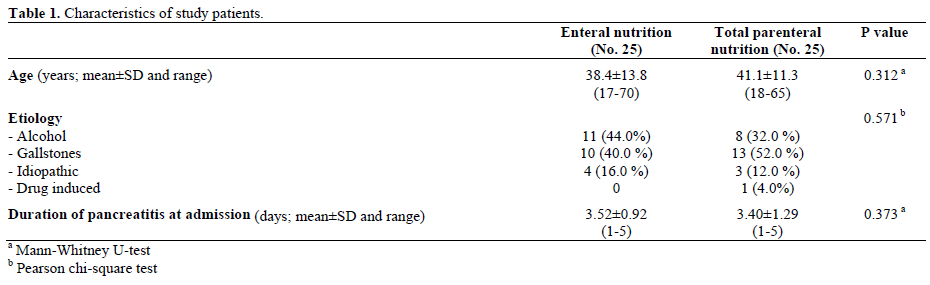
The characteristics of the study patients are shown in Table 1. No significant differences were found between the two groups of patients. Their age ranged from 17- 70 years in EN group and 18-65 years in TPN group. The etiological factors were alcohol (n=19, 38.0%) gallstones (n=23, 46.0%), idiopathic (n=7; 14.0%) and drug-induced (n=1, 2.0%). The mean duration of presentation was 3.52±0.9 days in the EN group and 3.40±1.29 days in the TPN group.
Data Collection
The following data were collected prospectively from all patients: i) demographic data including gender, age and etiology of pancreatitis; ii) clinical data including number of days of abdominal pain, and paralytic ileus defined by abdominal distension and absence of bowel sounds; iii) biochemical data including serum levels of amylase at hospital admission and thereafter periodically, serum C-reactive protein (CRP) using the latex slide agglutination test (Telco Diagnostics, Anaheim, CA ,U.S.A.) before the initiation of nutrition and on the 3rd, 5th, 7th and 14th day of nutrition support, serum albumin and transferrin before the initiation of nutritional support and repeated on the 7th and 14th day of nutritional support; iv) radiological data including pancreatic necrosis and peripancreatic fluid collections determined by CECT performed before the initiation of nutritional support and repeated on day 14 to look for any changes in the CTSI [21]; v) radiological or surgical intervention; vi) hospital stay and vii) mortality.
Nutritional Support
Patients were randomized using odd/even numbers to either enteral nutrition or total parenteral nutrition. The targeted caloric and protein requirements were 2,500- 2,700 kcal/day, and 120-130 g/day of protein. Feeding for study purposes was given for 14 days, and the last evaluation was done on day 14. Jejunal feeding was started at low flow rates - an initial rate of 20-30 mL/h until achievement of the full regime of EN.
Delivery of Enteral Nutrition
For placement of an enteral tube, the patients were shifted to an endoscopic suite and a 16F single lumen 125 cm long red rubber feeding tube was placed over a 400 cm long stainless steel guidewire (Wilson Cook, Winston, Salem, U.S.A.) beyond the ligament of Treitz using fluoroscopic control. Seven of 25 patients required a second attempt at placement of the tube in the desired position. A test feed with 500 mL of normal saline was administered over a period of 4-5 hours and jejunostomy feed was started subsequently. Minor complications such as diarrhea and distension were managed by altering the infusion rate and adding an antimotility agent.
Parenteral Nutrition
A 16G central venous catheter was inserted through the subclavian or internal jugular vein. A chest X-ray was taken after insertion to check the catheter tip position and also to check for complications of central venous line placement. Commercially available parenteral nutrition formula (PNA: parenteral nutrition admixture; Claris Lifesciences Ltd., Ahmedabad, India) was administered. The target caloric and protein requirements were similar to the enteral group. Glycemic control and metabolic parameters were monitored. All patients in the parenteral group could be weaned to oral diet (those managed conservatively) and feeding through a jejunostomy catheter placed intraoperatively (those operated on).
STATISTICS
Statistical data analysis was performed by using the Statistical Package for Social Sciences (SPSS Inc., Chicago, IL, U.S.A.) for Windows version 13.0. A non-parametric Mann-Whitney U-test was used to compare the continuous values between groups. Comparison between pre-nutritional and postnutritional variables was carried out using the nonparametric Wilcoxon signed-rank test. Categorical data were described as absolute and relative frequencies, and were compared by the Pearson chi-square or the Fisher’s exact (2x2 tables) tests. Two-tailed P values of less than 0.05 were considered statistically significant.
ETHICS
The protocol for the study was approved by Ethical Committee of our institution and written informed consent was obtained from all patients. The study protocol conforms to the ethical guidelines of the "World Medical Association Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects" adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964, as revised in Tokyo 2004.
RESULTS
C-Reative Protein (CRP)
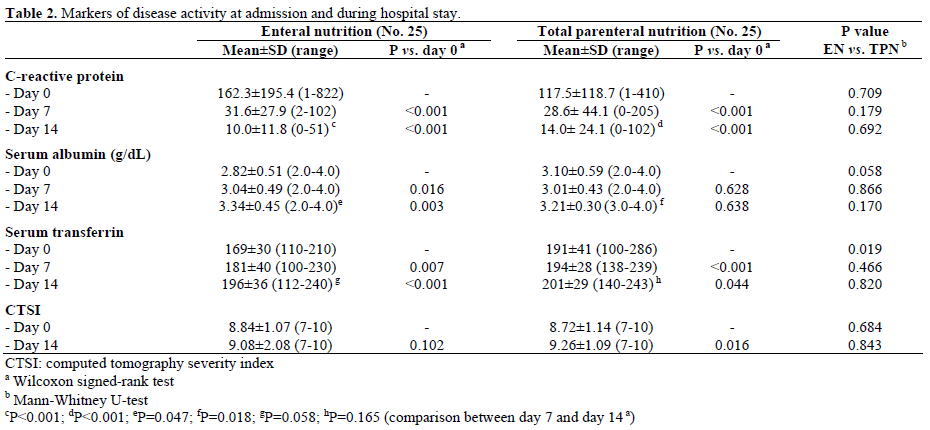
At admission, the CRP level was found to be high in both groups (Table 2). In the EN group, a decreasing trend was observed during the course of the nutritional support. A similar trend was observed in the TPN group. The decrease in CRP level was statistically significant in both groups.
Serum Albumin
In the EN group, a significant sequential rise in serum albumin was observed after admission up to day 14. In the TPN group, no significant differences were observed during the course of the nutritional support (Table 2). However, the two groups did not differ statistically (Table 2).
Serum Transferrin
In the EN group, a significant rise in transferrin value was observed during the course of nutritional support (Table 2). In TPN, the transferrin value also increased during the course of nutritional support, but the differences between the two groups were not statistically different at days 7 and 14 (Table 2).
CTSI
The mean CTSI on admission in the EN group was 8.84±1.07, and it was 9.08±2.08 on the 14th day of nutritional support. The CTSI increased during the study period in 8 patients (32.0%) while no change was observed in 16 patients (64.0%); one patient (4.0%) showed a reduction in the CTSI. In the TPN group, the mean index on admission was 8.72±1.14 and was 9.26±1.09 on day 14 of nutritional support. The disease severity index increased in 7 patients (28.0%) and, in the other 18 (72.0%), the CTSI was unchanged. There was no significant difference in the CTSI on admission and on day 14 of nutritional support between the two groups (Table 2).
Management
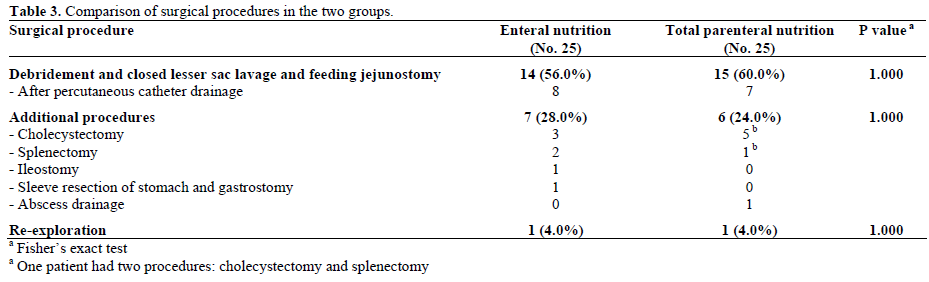
Supportive treatment was instituted in all patients. Six patients (24.0%) in each of the two groups, EN and TPN, were managed successfully without any radiological or surgical intervention. Thirteen patients (52.0%) in the EN group underwent percutaneous catheter drainage; five of these patients were managed successfully with percutaneous catheter drainage alone. In the TPN group, 11 patients (44.0%) underwent percutaneous catheter drainage and four of them were managed successfully without surgical intervention. Therefore, surgical intervention was undertaken in 14 patients (56.0%) in the EN group and 15 patients (60.0%) in the TPN group. The median time interval to surgical intervention was 18 days (range: 0-42 days) in the EN group and 18 days (0-43 days) in the TPN group (P=0.369). The surgical procedures employed were pancreatic debridement, closed lesser sac drainage and placement of a feeding jejunostomy tube (Table 3).
Morbidity
There was no significant difference in locoregional complications between the two groups: 13 patients (52.0%) in the EN group and 10 (40.0%) in the TPN group had locoregional complications (P=0.571).
Infective Complications
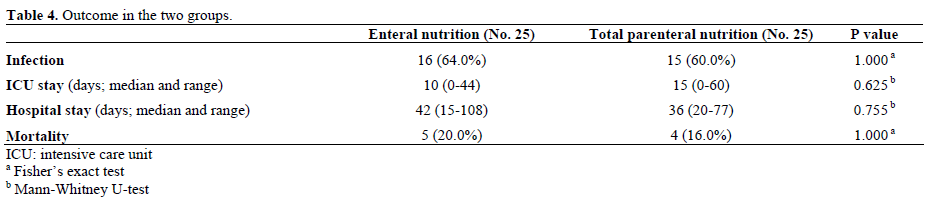
Documented infection was not significantly different between the two groups (Table 4; P=1.000): 16 (64.0%) patients in the EN group had documented infection (positive culture of FNA: 5, blood: 5, culture of operative specimen:11 and culture of drain fluid: 8) while, in the TPN group, 15 (60.0%) patients had positive cultures (FNA: 11, blood: 8, operative specimen: 6,and drain fluid: 5). There was a significant difference in the organisms found in the two groups (Table 5). While Escherichia coli was the predominant organism in the EN group, Staphylococcus aureus, Enterococci and Candida albicans were more often found in the TPN group. Statistical significance was reached only for gram positive organisms (P<0.001).
Mortality
The mortality rate was similar (P=1.000) between the EN (20.0%) and the TPN (16.0%) groups (Table 4). In the EN group, all 5 deaths occurred due to sepsis and multiorgan failure; 4 out of 5 deaths occurred in the post-operative period. In the TPN group, all 4 deaths occurred in the post-operative phase: 3 due to sepsis and multiorgan failure and one due to operative hemorrhage.
Hospital Stay
There was no significant difference in hospital stay between the two groups (P=0.755; Table 4). The duration of hospital stay in the EN group ranged from 15 to 108 days (median 42 days) and, in the TPN group, it ranged from 20 to 77 days (median 36 days). Similar behavior was observed for the intensive care unit (ICU) stay (Table 4).
DISCUSSION
Nutritional support is emerging as a vital component of the management of severe acute pancreatitis, and enteral nutrition is reported to be the best nutritional support in severe acute pancreatitis [2]. EN avoids TPN complications, maintains intestinal health and may prevent the progression of multiple organ failure [2].
This prospective randomized study focused on the effects of EN delivered beyond the ligament of Treitz via an endoscopically-placed nasojejunal feeding tube and compared it with TPN. It has been suggested that EN ameliorates the inflammatory response better than TPN in severe acute pancreatitis [22, 23]. Both forms of nutritional support helped in significantly reducing serum CRP levels during the period of nutritional support in our study. In patients with infective complications, the serum CRP level was significantly high until day 5 in the EN group and until day 7 in the TPN group as compared to patients without infective complications (data not shown). Other studies have also not shown any significant reduction in CRP levels after 7 days in the enteral feeding group; Loule et al. [22] reported that CRP levels were reduced to 50% of the enrolment levels a average of 5 days faster for EN than TPN, and Zhao et al. [23] found a reduction of CRP on day 4 in the EN group and on day 7 in the TPN group.
Powell et al. [24] reported that early EN did not ameliorate the inflammatory response in patients with severe acute pancreatitis. In their study, the introduction of EN did not affect the serum concentrations of interleukin-6 (IL-6), soluble tumor necrosis factor receptor I (STNFRI) and CRP over the first 4 days of the study. Pearce et al. [16] have shown that, after 3 days of feeding, 13% of patients had reduced their CRP by 40 mg/L or more in the study group. In the control group, 3.8% of patients had reduced their CRP by this amount. Serum transferrin levels rose significantly in both the EN and the TPN groups in our study, corresponding to the changes in serum CRP. The improvement was more marked, however, in EN group (Table 2).
In our study, the serum albumin level increased gradually during the nutritional support in both groups. The increase in albumin levels was found from the beginning of nutritional support in the enteral group. In the TPN group, a significant increase was observed only between day 7 and day 14 days of nutritional support. Loule et al. [22] observed that both EN and TPN were equally effective in improving serum albumin level. Zhao et al. [23] showed a significant increase of body weight and pre-albumin levels in the EN group while serum albumin levels were not increased. In another study regarding EN, serum albumin concentration increased from 3.0 to 3.8 g/dL (P<0.001) [25].
There are limited studies on the effect of nutritional support on the CTSI. No significant difference has been reported on CECT findings in the studies reported [22, 26, 27]. We looked at the change in the CTSI at 14 days after admission, and a significant increase of the CTSI score was seen in the TPN group. However, there was no significant difference in the CTSI score between the two groups both at admission and after nutritional support. Makola et al. [25] have reported a decrease in the CTSI from 4 to 2 in their patients following enteral nutrition. Our patients had a much higher CTSI at admission than those reported by Makola et al. [25] denoting a more severe disease state which still evolved in the following14 days.
The type of nutrition has also been shown to influence infectious complications. Petrov et al. [6] reported significantly lower infections in the EN group as compared to the TPN group. We found similar rates of infection in the two groups (Table 4). However, there was a striking difference in the type of organisms found in the two groups (Table 5). Patients given TPN were more often infected by gram-positive organisms and fungi as compared to those given EN who were more often infected by a gram-negative organism. This observation has an important bearing on the outcome of severe acute pancreatitis as fungal infection carries a higher risk of mortality. Though proper aseptic precautions were maintained, the occurrence of infections with gram positive organisms such as Staphylococci in the TPN group suggests that it could be due to the invasion of central line catchers with cutaneous commensals.

In our study, no significant difference was found in the rate of surgical intervention in either group. Modena et al. [26] reported a significantly lower rate of surgical intervention in the EN group. In their series, 38 out of 43 patients (88.4%) in the TPN group required surgical intervention versus 11 patients out of 44 (25.0%) in the EN group (P<0.01). Petrov et al. [6] also reported a lower surgical intervention rate in the EN group as compared to the TPN group. Our observations are different, perhaps due to a more severe disease state in our patients. There was no significant difference in hospital stay in the two groups; the median duration of the hospital stay was 42 days for the EN group, and 36 days for the TPN group. Some studies have shown a reduced hospital stay in the EN group [28, 29] and several studies have reported a reduced mortality rate in the EN group. Modena et al. [26] and Petrov et al. [6] have reported significantly lower mortality rates in the EN group as compared to the TPN group. In our study, no significant difference was observed between the EN (20.0%) and the TPN (16.0%) groups.
In conclusion, our prospective study has shown that TPN and EN were equally effective in ameliorating the inflammatory response and improving the nutritional status of the patients. Mortality, hospital stay and ICU stay were also similar in the two groups. The two forms of nutrition differed, however, in terms of infective organisms. The use of TPN was more often associated with infection with gram positive and fungal organisms whereas the use of EN was associated with gram negative organisms.
Conflict of interest The authors have no potential conflicts of interest
References
- Thomson A. Nutritional support in acute pancreatitis. Curr Opin Clin Nutr Metab Care 2008; 11:261-6. [PMID 18403922]
- Ioannidis O, Lavrentieva A, Botsios D. Nutrition support in acute pancreatitis. JOP. J Pancreas (Online) 2008; 9:375-90. [PMID 18648127]
- García Almansa A, García Peris P. Nutritional management of patients with acute pancreatitis: when the past is present. Nutr Hosp 2008; 23 (Suppl 2) :52-8. [PMID 18714411]
- Skipworth JR, Pereira SP. Acute pancreatitis. Curr Opin Crit Care 2008;14:172- 8. [PMID 18388680]
- Marik PE, Zaloga GP. Meta-analysis of parenteral nutrition versus enteral nutrition in patients with acute pancreatitis. BMJ 2004; 328:1407-10. [PMID 15175229]
- Petrov MS, Kukosh MV, Emelyanov NV. A randomized controlled trial of enteral versus parenteral feeding in patients with predicted severe acute pancreatitis shows a significant reduction in mortality and in infected pancreatic complications with total enteral nutrition. Dig Surg 2006; 23:336-45. [PMID 17164546]
- Abou-Assi S, Craig K, O'Keefe SJ. Hypocaloric jejunal feeding is better than total parenteral nutrition in acute pancreatitis: results of a randomized comparative study. Am J Gastroenterol 2002, 97:2255- 62. [PMID 12358242]
- Petrov MS, van Santvoort HC, Besselink MG, van der Heijden GJ, Windsor JA, Gooszen HG. Enteral nutrition and the risk of mortality and infectious complications in patients with severe acute pancreatitis: a meta-analysis of randomized trials. Arch Surg 2008; 143:1111-7. [PMID 19015471]
- Gramlich L, Taft AK. Acute pancreatitis: practical considerations in nutrition support. Curr Gastroenterol Rep 2007; 9:323-8. [PMID 17883982]
- Thomson A. Enteral versus parenteral nutritional support in acute pancreatitis: a clinical review. J Gastroenterol Hepatol 2006; 21:22-25. [PMID 16706807]
- Eatock FC, Chong P, Menezes N, Murray L, McKay CJ, Carter CR, Imrie CW. A randomized study of early nasogastric versus nasojejunal feeding in severe acute pancreatitis. Am J Gastroenterol 2005; 100:432-9. [PMID 15667504]
- Jiang K, Chen XZ, Xia Q, Tang WF, Wang L. Early nasogastric enteral nutrition for severe acute pancreatitis: a systematic review. World J Gastroenterol 2007; 13:5253-60. [PMID 17876897]
- Spanier BW, Mathus-Vliegen EM, Tuynman HA, Van der Hulst RW, Dijkgraaf MG, Bruno MJ; EARL Study Group. Nutritional management of patients with acute pancreatitis: a Dutch observational multicentre study. Aliment Pharmacol Ther 2008; 28:1159-65. [PMID 18657130]
- Muftuoglu MA, Isikgor S, Tosun S, Saglam A. Effects of probiotics on the severity of experimental acute pancreatitis. Eur J Clin Nutr 2006; 60:464-8. [PMID 16340953]
- Karakan T, Ergun M, Dogan I, Cindoruk M, Unal S. Comparison of early enteral nutrition in severe acute pancreatitis with prebiotic fiber supplementation versus standard enteral solution: a prospective randomized double-blind study. World J Gastroenterol 2007; 13:2733-7. [PMID 17569144]
- Pearce CB, Sadek SA, Walters AM, Goggin PM, Somers SS, Toh SK, et al. A double-blind, randomised, controlled trial to study the effects of an enteral feed supplemented with glutamine, arginine, and omega-3 fatty acid in predicted acute severe pancreatitis. JOP. J Pancreas (Online) 2006; 7:361-71. [PMID 16832133]
- Sahin H, Mercanligil SM, Inanç N, Ok E. Effects of glutamineenriched total parenteral nutrition on acute pancreatitis. Eur J Clin Nutr 2007, 61:1429-34. [PMID 17311061]
- Petrov MS, Atduev VA, Zagainov VE. Advanced enteral therapy in acute pancreatitis: is there a room for immunonutrition? A metaanalysis. Int J Surg 2008; 6:119-24. [PMID 18325863]
- Oláh A, Romics L Jr. Early enteral nutrition in acute pancreatitis-benefits and limitations. Langenbecks Arch Surg 2008; 393:261-9. [PMID 18266002]
- Bradley EL 3rd. A clinically based classification system for acute pancreatitis. Summary of the International Symposium on Acute Pancreatitis, Atlanta, Ga, September 11 through 13, 1992. Arch Surg 1993; 128:586-90. [PMID 8489394]
- Balthazar EJ, Robinson DL, Megibow AJ, Ranson JH. Acute pancreatitis: value of CT in establishing prognosis. Radiology 1990; 174:331-6. [PMID 2296641]
- Louie BE, Noseworthy T, Hailey D, Gramlich LM, Jacobs P, Warnock GL. 2004 MacLean-Mueller prize enteral or parenteral nutrition for severe pancreatitis: a randomized controlled trial and health technology assessment. Can J Surg 2005; 48:298-306. [PMID 16149365]
- Zhao G, Wang CY, Wang F, Xiong JX. Clinical study on nutrition support in patients with severe acute pancreatitis. World J Gastroenterol 2003; 9:2105-8. [PMID 12970916]
- Powell JJ, Murchison JT, Fearon KC, Ross JA, Siriwardena AK. Randomized controlled trial of the effect of early enteral nutrition on markers of the inflammatory response in predicted severe acute pancreatitis. Br J Surg 2000; 87:1375-81. [PMID 11044164]
- Makola D, Krenitsky J, Parrish CR. Enteral feeding in acute and chronic pancreatitis. Gastrointest Endosc Clin N Am 2007; 17:747- 64. [PMID 17967379]
- Targarona Modena J, Barreda Cevasco L, Arroyo Basto C, Orellana Vicuña A, Portanova Ramírez M. Total enteral nutrition as prophylactic therapy for pancreatic necrosis infection in severe acute pancreatitis. Pancreatology 2006; 6:58-64. [PMID 16327282]
- Windsor AC, Kanwar S, Li AG, Barnes E, Guthrie JA, Spark JI, et al. Compared with parenteral nutrition, enteral feeding attenuates the acute phase response and improves disease severity in acute pancreatitis. Gut 1998; 42:431-5. [PMID 9577354]
- Gupta R, Patel K, Calder PC, Yaqoob P, Primrose JN, Johnson CD. A randomised clinical trial to assess the effect of total enteral and total parenteral nutritional support on metabolic, inflammatory and oxidative markers in patients with predicted severe acute pancreatitis (APACHE II > or =6). Pancreatology 2003; 3:406-13. [PMID 14526151]
- Sun B, Gao Y, Xu J, Zhou XL, Zhou ZQ, Liu C, Jiang HC. Role of individually staged nutritional support in the management of severe acute pancreatitis. Hepatobiliary Pancreat Dis Int 2004; 3:458- 63. [PMID 15313689]

