Keywords
Diabetes Mellitus; Pancreatitis
Abbreviations
CP chronic pancreatitis; DM diabetes mellitus; FMD
flow mediated dilatation
INTRODUCTION
Brachial artery flow mediated dilatation (FMD)
has been to be reduced in patient having endothelial
dysfunction in cases of atherosclerosis, coronary artery
disease and DM [1]. FMD evaluates the function of vascular
endothelial cells, and reduced FMD is a predictive factor
for major vascular complications including cardiovascular
diseases [2]. Adults with type 1 and type 2 DM were
reported to have decreased FMD [3, 4]. Interestingly,
endothelial dysfunction may precede the development
of DM. In this regard healthy non- diabetic subjects who
have first degree relative with type II DM display impaired
endothelium dependent vasodilatation as well as increased
plasma markers of endothelial cell activation [5].
However, there are no studies which studied
endothelial function in the form of FMD in type IIIc DM
or chronic pancreatitis (CP). We aimed to study brachial
artery flow mediated dilatation as a marker for endothelial
dysfunction in patients with DM associated with chronic pancreatitis and CP without DM, in comparison to normal
controls. We also studied FMD in relation to etiology of
pancreatitis either alcohol or idiopathic, history of smoking
along with pancreatic disease phenotype and status of DM.
METHODS
After approval from Institutional review board, a
total of ninety eight individuals were included in this
prospective cross sectional observational study, after
taking informed consent. All subjects in study were
included from Medical Gastroenterology OPD at Asian
Institute of Gastroenterology, Hyderabad.
A total of 143 patients were screened for study, out
of which 45 patients were excluded. Consort diagram is
depicted in Figure 1. Patients with acute exacerbation
of chronic pancreatitis, infected fluid collections, active
sepsis, hypertension, dyslipidaemia, coronary artery
disease, pregnancy, post pancreatic surgery, pancreatic
or extra pancreatic malignancy or severe co-morbidity
including chronic liver disease were excluded from study.
A total of ninety eight individuals were included in the
study and divided into three groups. Group A included
subjects with chronic pancreatitis with type IIIc DM; group
B included subjects with chronic pancreatitis without IIIc
DM; group C included subjects without CP or DM.
Figure 1. Consort diagram showing study and control population.
Chronic pancreatitis was diagnosed by presence
of typical history of recurrent pancreatic pain and
imaging evidence showing PD dilatation, PD stricture and calcification ductal and/or parenchymal. DM was
diagnosed as per criteria proposed by ADA [6]. Type IIIc
DM was differentiated from Type I and type II by clinical
history and anti- GADD or c-peptide whenever necessary
[7]. Demographic and clinical profile of enrolled patients
was noted. All included patients were subdivided according
aetiology of pancreatitis either alcohol related or idiopathic;
also history of smoking was noted. Pancreatic disease
phenotype was noted as exocrine, endocrine insufficiency,
parenchymal or ductal calcification, and pancreatic ductal
or common bile duct stricture and associated pancreas
divisum. Pancreatic pain characteristics were noted
as Izbicki’s score [8] and painDETECT [9]. Clinical and
laboratory data of patient with DM was collected which
included duration of diabetes mellitus, HbA1c. Controls
were selected from Medical gastroenterology OPD who
were diagnosed as functional bowel diseases, either acid
peptic disease or irritable bowel syndrome with adequate
matching for history of smoking and alcohol.
The brachial artery FMD assessment was performed
once in all included patients using 7.5 MHz phased
array linear transducer attached to HP Sonos 5500
echocardiography machine. Smoking was prohibited for
at least four hours before test. The sphygmomanometer
cuff was tied in the right arm with the patient in supine
position. The brachial artery was imaged in the antecubital
fossa and its diameter was measured. Brachial
artery was then occluded with the sphygmomanometer cuff inflation to at least 50mm Hg above systolic blood
pressure for five minutes. Brachial artery diameter was
measured again at one minute after deflation to assess
FMD. FMD was calculated as percentage change in brachial
artery diameter at 1 minute.
FMD = (Brachial artery diameter at 1min – Baseline
diameter) × 100/Baseline diameter
STATISTICAL ANALYSIS
The data for the present study was collected on predesigned
standard format. The data was entered in MS-excel
after editing for completeness and consistency of the data.
The values were expressed as mean and Standard deviation
for continuous variables and as proportion for categorical
variables. Student’s t test was applied for comparing the two
groups for continuous variables. The chi-square, median or
Fishers exact test was used for categorical variables in view
of the small sample size. Spearman correlation coefficient
analysis was used for continuous variables. Analysis of
variance was used to compare multiple groups followed
Tukey post hoc test. All reported P values are 2 tailed. A p
value of 0.05 was regarded as statistically significant. The
analysis was carried out using Statistical package for social
Sciences (SPSS 20th version).
RESULTS
A total of 103 patients with chronic pancreatitis
were screened for study population. Out of which 38 were excluded; 13 for acute exacerbation of CP or fluid
collection, 8 for mass lesion in pancreas, 9 for either type
I or type II DM and 8 for other significant comorbidities.
5 patients were diagnosed to have type I DM on basis of
young age, history of ketoacidosis, low c-peptide levels
(Mean 0.75 ng/ml) and Anti-GADD positivity. Four
patients were diagnosed to have type II DM on basis
of obesity, high c-peptide levels (Mean 3.8 ng/ml) and
Anti- GADD negativity. These 9 patients were excluded
as mentioned in Figure 1. To A total of 40 patients were
screened for control group, out of which 7 were excluded
due to presence significant comorbidities. A total of 98
were enrolled in the present study, which were divided
into three groups. Group A (n=31) included patients with
CP and type IIIc DM; group B (n=34) included patients with
CP without diabetes; and group C (n=33) included patients
without CP or DM. All subgroups were adequately matched
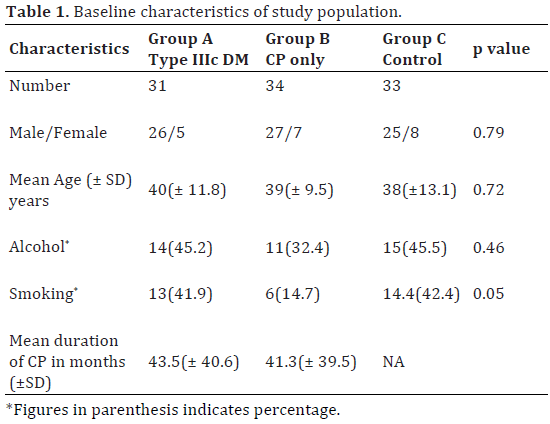
for age, sex and history of smoking or alcohol intake. Table
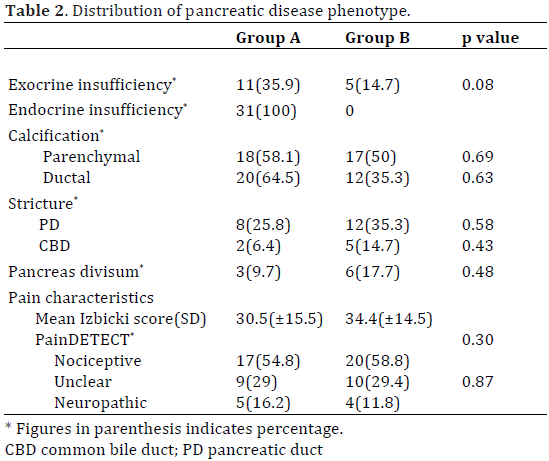
1 depicts demographic characteristics of study population. Table 2 describes pancreatic disease phenotypes along
with pain characteristics of group A and B.
There was a statistically significant difference between
groups as determined by one- way ANOVA (F (2, 95) =
68.1, p value 0.0001) as depicted in Figure 2. A Tukey
post hoc test revealed that the mean FMD was statistically
significantly lower in group A (2.74±1.28) compared to
group B (4.39±1.90) and group C (8.31±2.51, p<0.01).
There was statistical difference between group B and C
(p<0.01).
Figure 2. Comparison of mean FMD in pre-specified groups.
Subgroup analysis (Figure 3) revealed that mean
FMD in the alcohol related CP (2.441±1.128) compared to
idiopathic CP (4.324±1.802, p value 0.0055) and control
(8.315±2.515, p value 0.0001). In alcohol related CP, there
was no statistically difference of FMD between overall,
smokers and non-smokers (p value >0.05). In idiopathic
CP, there was no difference in mean FMD between overall,
smokers and non-smokers (p value >0.05). In smokers,
mean FMD of alcohol related CP (2.041±0.685) and
idiopathic CP (3.92±1.095) was not statistically different
(p value 0.9310), however significantly lower than
controls who smoke (7.548±1.51, p value 0.0001). In nonsmokers,
mean FMD of alcohol related CP (3.153±1.43) and
idiopathic CP (4.35±1.838) was not statistically different
(p value 0.7626), however significantly lower than control
who don’t smoke (8.88±2.966, p 0.0001).
Figure 3. FMD analysis with respective to etiology and smoking.
There was no significant difference in FMD as per
presence of exocrine insufficiency, PD stricture, CBD
stricture, parenchymal or ductal calcification (p value
>0.05) by Chi-square test. There was no statistical
correlation between PD size, Izbicki score and painDETECT
(p value >0.05), however, there was statistically significant
correlation between HbA1c and FMD (p value 0.005) using
Spearman correlation coefficient analysis.
DISCUSSION
In the current study, we attempted to study endothelial
dysfunction in the form of brachial artery FMD in patient with chronic pancreatitis with or without type IIIc DM.
We also evaluated pancreatic disease phenotype in the
form of structural changes and pain scores (Izbicki score
[8] and painDETECT [9]) and its relation with endothelial
dysfunction.
To best of our knowledge, this is the first study which
evaluated presence of endothelial dysfunction is type IIIc
DM and CP. We used non-invasive, easy to perform and
reproducible method to study endothelial dysfunction
in the form of brachial artery reactivity. Brachial artery
FMD is high – frequency ultrasonographic imaging of the
brachial artery to assess endothelium dependent dilation
of brachial artery following sheer stress [10]. The sheer
stress provokes the release of nitric oxide, resulting
in vasodilation the can be quantified and expressed as
percentage as an index of endothelial function. Endothelium
derived NO is principal mediator of FMD [11].
There is now adequate data exists to suggest that
endothelial dysfunction occurs in both type I [12] and
type II DM [13] as well as in insulin resistance without DM
[5]. Also Ito H, et al in recent study found that The FMD
was also lower in the subjects both with coronary artery
disease (5.6±2.8%) and without coronary artery disease
(6.1±3.3%) among the patients with diabetes compared to those without both diabetes and CHD [14]. However, there
are no studies in literature which evaluated endothelial
dysfunction in type IIIc DM or CP. In our study we found
that there is significant endothelial dysfunction in patient
with type IIIc DM and CP. compared to controls. There
was significant endothelial dysfunction in idiopathic
CP compared to controls indicating that CP itself can
have endothelial dysfunction, also there was significant
endothelial dysfunction in alcohol related CP and
idiopathic CP suggesting possible additional role of alcohol
in promoting endothelial dysfunction. In patients with
alcohol related or idiopathic CP, smoking may exacerbate endothelial dysfunction. However due to small number of
patient who smoke in idiopathic CP group it is difficult to
interpret.
There was no difference in endothelial dysfunction
according to diseases phenotype of CP. There was no
correlation between PD size, Izbicki score and painDETECT,
indicating that endothelial dysfunction in CP is not related
to anatomical abnormalities and pain characteristics in the
CP. However, there was linear correlation between HbA1c
and FMD, indicating poor glycaemic control is related to
more endothelial dysfunction, which is in concordance to
previously publish studied in type I and type II DM [15, 16].
Presence of endothelial dysfunction in CP and type
IIIc DM may have role in progression of inflammation
and fibrosis in chronic pancreatitis. Also presence of
endothelial dysfunction in smokers and alcohol drinkers
may be the factor responsible for faster progression of
chronic pancreatitis in these patients. These findings
need to be confirmed by larger studies and also it
should be correlated with other markers of endothelium
activation.
Conflicts of interests
The authors indicated no potential conflict of interests.
References
- Naylor LH, Green DJ, Jones TW, Kalic RJ, Suriano KL, Shah M, et al.
Endothelial function and carotid intima-medial thickness in adolescents
with type 2 diabetes mellitus. J Pediatr 2011; 159:971–974. [PMID:
21722916]
- Yeboah J, Folsom AR, Burke GL, Johnson C, Polak JF, Post W, et
al. Predictive value of brachial flow-mediated dilation for incident
cardiovascular events in a population-based study:the multi-ethnic study
of atherosclerosis. Circulation 2009; 120:502–509. [PMID: 19635967]
- Jin SM, Noh CI, Yang SW, Bae EJ, Shin CH, Chung HR, et al. Endothelial
dysfunction and microvascular complications in type 1 diabetes mellitus.
J Korean Med Sci 2008; 23:77–82. [PMID: 18303203]
- Johnstone MT, Creager SJ, Scales KM, Cusco JA, Lee BK, Creager MA.
Impaired endothelium-dependent vasodilation in patients with Insulin-
Dependent Diabetes Mellitus. Circulation 1993; 88:2510-2516. [PMID:
8080489]
- Balletshofer BM, Rittig K, Enderle MD, Volk A, Maerker E, Jacob S,
et al. Endothelial dysfunction is detectable in young normotensive first
degree relatives of subjects with type 2 DM in association with insulin
resistance. Circulation 2000; 101:1780-1784. [PMID: 10769277]
- American Diabetes Association. Standards of medical care in
diabetes–2014. Diabetes Care 2014; 37:S14–S80. [PMID: 24357209]
- Rickels MR, Bellin M, Frederico GS, Andersen DK, Chari ST, Brand R,
et al. Detection, evaluation and treatment of diabetes mellitus in chronic
pancreatitis: Recommendations from Pancreas Fest 2012. Pancreatology
2013; 13:336-342. [PMID: 23890130]
- Izbicki JR, Bloechle C, Knoefel WT, Kuechler T, Binmoeller KF,
Broelsch CE. Duodenum-preserving resection of the head of the pancreas
in chronic pancreatitis. A prospective, randomized trial. Ann Surg 1995;
221:350–358. [PMID: 7726670]
- Rados I, Sakic Zdravcevic K, Hrgovic Z. Pain detect questionnaire and
lumbar epidural steroid injection for chronic radiculopathy. Eur Neurol
2013; 69:27–32. [PMID: 23128915]
- Celermajer DS, Sorensen KE, Gooch VM, Spiegelhalter DJ, Miller OI,
Sullivan ID, et al. Non-invasive detection of endothelial dysfunction in
children and adult at risk of atherosclerosis. Lancet 1992; 340:1111-
1115. [PMID: 1359209]
- Corretti MC, Anderson TJ, Benjamin EJ, Celermajer DS, Charbonneau
F, Creager MA, et al. Guidelines for the ultrasound assessment of
endothelium dependent flow mediated vasodilatation of brachial artery.
A report of the international brachial artery reactivity task force. J Am
Coll Cardiol 2002; 39:257-265. [PMID: 11788217]
- Dogra G, Rich L, Stanton K, Watts GF. Endothelium dependent and
independent vasodilatation studies at normoglycemia in type I diabetes
mellitus with and without microalbuminuria. Diabetologia 2001; 44:593-
601. [PMID: 11380077]
- Yu HI, Sheu WH, Lai CJ, Lee WJ, Chen YT. Endothelial dysfunction
in type 2 diabetes mellitus subjects with peripheral artery disease. Int J
Cardiol 2001; 78:19-25. [PMID: 11259809]
- Ito H, Nakashima M, Meguro K, Furukawa H, Yamashita H, Takaki A,
et al. Flow mediated dilatation is reduced with the progressive stages
of glomerular filtration rate and albuminuria in type 2 diabetic patients
without coronary heart disease. J Diabetes Res 2015; 2015:728127.
[PMID: 26064988]
- Kotb NA, Gaber R, Salah W, Elhendy A. Relations among glycemic
control, circulating endothelial cells, nitric oxide, and flow mediated
dilation in patients with type 2 diabetes mellitus. Exp Clin Endocrinol
Diabetes 2012; 120:460-465. [PMID: 22639396]
- Voidonikola, PT, Stamatelopoulos KS, Alevizaki, M, Kollias GE,
Zakopoulos NA, Lekakis JP, et al. The association between glycemia and
endothelial function in nondiabetic individuals:the importance of body
weight. Obesity 2008; 16:2658–2662. [PMID: 18846051]




